Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Echocardiography wikipedia , lookup
Electrocardiography wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Jatene procedure wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
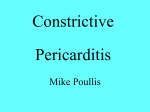
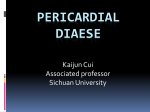
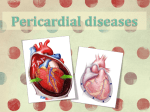
® CARDIOLOGY BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, GROUP PUBLISHER Bruce M. White EDITORIAL DIRECTOR Constrictive Pericarditis: A Case Study Debra Dreger SENIOR EDITOR Miranda J. Hughes, PhD ASSISTANT EDITOR Rita E. Gould EXECUTIVE VICE PRESIDENT Barbara T. White, MBA EXECUTIVE DIRECTOR OF OPERATIONS Jean M. Gaul PRODUCTION DIRECTOR Suzanne S. Banish PRODUCTION ASSOCIATES Tish Berchtold Klus Mary Beth Cunney Series Editor: A. Maziar Zafari, MD, PhD, FACC Assistant Professor of Medicine, Division of Cardiology, Department of Medicine, Emory University School of Medicine, Atlanta, GA; Director, CCU, Atlanta Veterans Affairs Medical Center, Decatur, GA Contributors: William J. Nicholson, MD Cardiology Fellow, Division of Cardiology, Department of Medicine, Emory University School of Medicine, Atlanta, GA; Cardiology Fellow, Atlanta Veterans Affairs Medical Center, Decatur, GA Andro G. Kacharava, MD, PhD Assistant Professor of Medicine, Division of Cardiology, Emory University School of Medicine, Atlanta, GA; Staff Cardiologist, Atlanta Veterans Affairs Medical Center, Decatur, GA PRODUCTION ASSISTANT Stacey Caiazzo Table of Contents ADVERTISING/PROJECT MANAGER Patricia Payne Castle MARKETING MANAGER Deborah D. Chavis NOTE FROM THE PUBLISHER: This publication has been developed without involvement of or review by the American Board of Internal Medicine. Endorsed by the Association for Hospital Medical Education The Association for Hospital Medical Education endorses HOSPITAL PHYSICIAN for the purpose of presenting the latest developments in medical education as they affect residency programs and clinical hospital practice. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Clinical and Physical Findings . . . . . . . . . . . . . . 3 Physiology and Pathology. . . . . . . . . . . . . . . . . . 5 Diagnostic Imaging Modalities . . . . . . . . . . . . . . 5 Hemodynamics . . . . . . . . . . . . . . . . . . . . . . . . . 7 Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 Summary Points . . . . . . . . . . . . . . . . . . . . . . . . 10 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 Cover Illustration by Stacey Caiazzo Copyright 2003, Turner White Communications, Inc., 125 Strafford Avenue, Suite 220, Wayne, PA 19087-3391, www.turner-white.com. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White Communications, Inc. The editors are solely responsible for selecting content. Although the editors take great care to ensure accuracy, Turner White Communications, Inc., will not be liable for any errors of omission or inaccuracies in this publication. Opinions expressed are those of the authors and do not necessarily reflect those of Turner White Communications, Inc. Cardiology Volume 9, Part 2 1 CARDIOLOGY BOARD REVIEW MANUAL Constrictive Pericarditis: A Case Study William J. Nicholson, MD, and Andro G. Kacharava, MD, PhD I. INTRODUCTION Constrictive pericarditis (CP) is a relatively rare postinflammatory disorder with different causes. The diagnosis of CP and its distinction from restrictive cardiomyopathy (RCM) remain notoriously difficult. Patients with both conditions present with increased left-sided and rightsided filling pressures, and their symptoms may resemble congestive heart failure (CHF). It is paramount to diagnose and distinguish these 2 entities because surgical pericardiectomy is potentially curative in CP. Constrictive pericarditis is a condition in which the pericardial sac undergoes a process of progressive thickening and fibrosis; the natural elasticity of the pericardial sac is lost, subsequently placing the heart in a nonpliable and rigid encasement, impairing diastolic filling of the ventricles. Restrictive cardiomyopathy refers to idiopathic or systemic disorders involving the myocardium characterized by restrictive diastolic filling of the ventricles. Many clinical and hemodynamic findings are common to both CP and RCM, making the 2 disorders difficult to distinguish. The purpose of this review is to discuss the clinical presentation of CP and to focus on the hemodynamic, echocardiographic, and radiologic findings differentiating it from RCM. Although the diagnosis can usually be achieved via these noninvasive and invasive studies, surgical exploration or biopsy occasionally is needed to make definitive diagnosis. A case patient is presented to illustrate the management of CP. ANATOMICAL CONSIDERATIONS The pericardium is an elastic, closed fibroserous sac surrounding the heart. It consists of 2 layers of tissue: an external (fibrous) and an internal (serous) layer. The internal or serous layer is made up of both visceral and parietal pericardium. The visceral layer is a thin monocellular layer adherent to the heart’s epicardium. The parietal pericardium is adjacent to the visceral pericardium on one side and becomes tightly opposed to the external fibrous layer on the other side. The space created between the visceral and parietal layers of the pericardium contains approximately 30 to 50 mL of serous fluid, which acts as a lubricant to minimize fric- 2 Hospital Physician Board Review Manual tion between the 2 layers of pericardium during the heart’s movement throughout the cardiac cycle.1 This fluid-filled space defines the pericardial cavity. The fibrous pericardium envelops the entire heart and extends over approximately 3 cm of the great vessels where it then attaches. Therefore, much of the ascending aorta, the main pulmonary artery, all 4 pulmonary veins, and portions of the inferior and superior venae cavae are contained within the pericardium.2 Fibrosis and scarring can affect each of the layers of the pericardium either separately or simultaneously. Development of adhesions and calcifications between the layers can lead to obliteration of the pericardial cavity, creating a rigid inelastic “shell” around the heart with resultant pathophysiologic consequences (ie, CP). As the pericardial cavity is obliterated in patients with CP, even the physiologic amount of pericardial fluid may disappear; however, excessive amounts of effusive fluid may be present in some patients. As this fluid is subjected to the constricting effects of the scarred pericardium, increased pressure can result in cardiac compression or tamponade with resultant hemodynamic deterioration; this entity is known as effusive CP.3,4 In such cases, the constrictive hemodynamics are masked by tamponade and may only become obvious after the pericardial fluid is drained by pericardiocentesis. ETIOLOGIES Many different conditions can produce acute pericarditis, and nearly all are capable of inducing constriction, albeit some more frequently than others (Table 1).5 The notable exception is acute rheumatic fever, which can produce extremely dense pericardial adhesions that rarely lead to constriction.6 As with many other diseases, the dominant causes of CP have changed over the years. Tuberculosis was historically the leading cause of CP and remains a dominant cause in developing countries. Neoplasm, collagen vascular disease, infectious etiologies, radiation therapy, and previous cardiac surgery are some of the more common causes of constriction in modern developed countries.7 However, in numerous cases (even after microscopic and culture examination of pericardial scar tissue), an inciting etiology is not found. In fact, idiopathic or presumed viral etiologies are now the leading Constrictive Pericarditis: A Case Study cause of CP in developed countries, composing up to 42% of cases in some series.8 Nevertheless, a thorough search for tuberculosis (ie, evidence of granulomatous lesions) must be made before concluding that the pericardial disease is of unknown origin.9 RCM is the least common of the cardiomyopathic disorders.10 RCM may result from various primary localized cardiac processes or may be secondary to systemic infiltrative or storage diseases.11 Cardiac amyloidosis is the most common cause of RCM in developed countries, whereas endomyocardial fibrosis is endemic in parts of Africa, India, Asia as well as South and Central America.12 Although restrictive disease can arise from systemic disorders that are rarely encountered in clinical practice, conditions such as amyloidosis, sarcoidosis, and hemochromatosis are more common. Idiopathic RCM is an uncommon disorder manifested by the characteristic hemodynamic abnormalities of restriction in the absence of any identifiable cause. Because restrictive physiology is seen in patients with various systemic disorders, idiopathic RCM is a diagnosis of exclusion. Although RCM can occur in elderly persons, it should be differentiated from the age-related changes in diastolic compliance.13 II. CLINICAL AND PHYSICAL FINDINGS CASE PATIENT 1 PRESENTATION Patient 1 is a 52-year-old woman who presents to the general medical clinic complaining of 6 months of dyspnea. The patient has gained approximately 25 lb during the preceding several months, with increased abdominal girth and discomfort as well as marked lower extremity swelling. Before her present complaints, she had been in good health and was taking no medications. Her last medical visit was 15 years earlier when she had a cholecystectomy. Initial physical examination reveals a frail cachectic woman with pitting lower extremity edema, hepatomegaly, and tense ascites. Breath sounds are diminished at the bases bilaterally. Cardiovascular examination is remarkable for a resting tachycardia, jugular venous distention (JVD), and an early diastolic sound thought to be an S3. Liver transaminase levels are elevated, and the patient’s albumin is slightly reduced. A paracentesis is performed, which reveals a transudate effusion. Radiologic evaluation of the chest and abdomen as well as colonoscopy for potentially malignant etiologies of the prominent ascites and liver disease are both unrevealing. However, a computed tomography (CT) scan Table 1. Causes of Constrictive Pericarditis Idiopathic Infectious* Drugs† Radiation Chest trauma Cardiovascular surgery Heart transplantation Epicardial defibrillator patches Connective tissue disease‡ Renal failure (on chronic dialysis) Myocardial infarction Neoplasms Sarcoidosis Mulibrey nanism (Perheentupa syndrome) Porphyria cutanea tarda Asbestosis Whipple’s disease Chylopericardium *Tuberculosis, viral, bacterial, or histoplasmosis. † Hydralazine, cromolyn sodium, procainamide, penicillins, isoniazid, minoxidil, phenylbutazone, or methysergide. ‡ Systemic lupus erythematosus, rheumatoid arthritis, or dermatomyositis. Adapted from Myers RB, Spodick DH. Constrictive pericarditis: clinical and pathophysiologic characteristics. Am Heart J 1999;138(2 Pt 1): 219–3, with permission from Elsevier Science. of the chest shows mild thickening of the pericardium. Liver biopsy shows congestion and nonspecific cirrhosis without evidence of infiltrative disease. Subsequent echocardiographic evaluation and cardiac catheterization are consistent with the diagnosis of CP and help in differentiating it from RCM. • What symptoms and signs are frequently associated with CP? • Can these findings reliably differentiate CP from RCM? DISCUSSION The clinical presentation and physical findings are similar in CP and RCM.5,14 Symptoms are typically insidious in onset and are closely related to the degree of systemic and central venous congestion as well as the degree of fluid retention. Poor appetite, cachexia, abdominal discomfort resulting from splanchnic engorgement, Cardiology Volume 9, Part 2 3 Constrictive Pericarditis: A Case Study A C A central venous pressure, particularly if there is a history of a predisposing condition. A clinical history of pericarditis, tuberculosis, trauma, or radiation therapy makes a diagnosis of CP more likely, whereas a history of a predisposing systemic disease (such as amyloidosis or sarcoidosis) would favor RCM. X V Normal X′ A Y V X X′ B Y Constrictive pericarditis Figure 1. Jugular venous pulsation. (A) Normal jugular venous pulsation. (B) Jugular venous pulsation in patients with CP. The sharp Y-wave dip forms the characteristic “W” shape known as the W-wave of Bloomfield. CP = constrictive pericarditis. (Adapted from Fuster V, Alexander RW, O’Rourke RA, et al, editors. Hurst’s the heart. 10th ed. New York: McGraw-Hill Medical Publishing Division; 2001:228–9. Copyright 2001, with permission of the McGraw-Hill Companies.) ascites, and peripheral edema with general fatigue and weakness can cause the clinician to inappropriately work-up a diagnosis of liver disease. As central diastolic pressures increase and symptoms of dyspnea, orthopnea, and occasionally platypnea become more prominent, clinicians can erroneously diagnose CHF. As seen with patient 1, failure to recognize the significance of elevations in jugular venous pressure (JVP) in a patient presenting with clear lungs, unremarkable chest radiograph, hepatomegaly, and ascites may lead the clinician to pursue liver biopsy before the correct diagnosis is recognized.15 CP and RCM may present predominantly with symptoms of systemic or pulmonary venous congestion depending on the extent and area of pericardial scarring or on the restrictive involvement of the myocardium. Thus, it is difficult to establish the diagnosis on clinical grounds alone. Symptoms can develop from weeks to decades after an inciting event (which the patient often does not recall), making the diagnosis less obvious. Several studies have shown that the average duration of symptoms before diagnosis was nearly 2 years.16,17 For this reason, constriction and restriction should be considered in any patient with unexplained elevation in 4 Hospital Physician Board Review Manual Neck Vein Examination Examination of the neck veins is essential when considering the diagnosis of CP. Increased JVP has been reported in 93% of patients with CP18 and is frequently encountered in RCM. Kussmaul’s sign, or inspiratory JVD, replaces the normal inspiratory venous collapse of the jugular veins in patients with CP. Although usually present in CP, Kussmaul’s sign is not specific; it is frequently present in RCM and can be observed in tricuspid stenosis, right heart failure, or systemic venous congestion of any cause. Figure 1 demonstrates the normal jugular venous pulsation contrasted with that seen in patients with CP.19 The normal jugular venous pulsation consists of 3 positive waves (A, C, and V) and 3 negative waves (X, X′, and Y). The positive A-wave is caused by the right atrial pressure transmitted to the jugular veins during right atrial systole, and atrial relaxation results in the descent of the A-wave. The C-wave occurs during the beginning of right ventricular systole, resulting from the bulging of the tricuspid valve into the right atrium. The X-wave descent, representing the atrial relaxation, is a negative wave preceding the C-wave that occurs in systole and followed by X′-wave descent, which represents systolic down movement of the floor of the right atrium caused by the right ventricular contraction. The V-wave occurs after the X′-wave descent as a result of an increase in right atrial pressure and JVP caused by continued inflow of blood to the venous system during late ventricular systole when the tricuspid valve is still closed. The Y-wave descent, or diastolic collapse, is produced by opening of the tricuspid valve and the rapid inflow of blood into the right ventricle. A sharp Y-wave descent and a rapid ascent to the baseline (referred to as the Friedreich’s sign) are seen in CP (Figure 1B). The venous pressure is elevated in these conditions with a sharp Y-wave dip in the jugular venous pulsation forming a characteristic “W” shape known as the W-wave of Bloomfield. Cardiac Examination Cardiac examination can be helpful in diagnosing CP, differentiating it from RCM, and excluding other potential etiologies. In RCM, the heart size is preserved and the ventricular systolic impulse is usually normal or Constrictive Pericarditis: A Case Study enhanced; heart size is either normal or smaller in patients with CP. The non-pliable and rigid encasement of the heart in CP results in precordial palpation that is often quiet without an appreciable ventricular impulse. An S3 is frequently heard in RCM. The abruptly amputated ventricular filling during diastole is caused by constriction from the rigid pericardium and results in a pericardial knock in CP. The knock usually occurs 0.06 to 0.12 seconds after the S2 sound and may be made more prominent by having the patient squat, which increases afterload.20 In patient 1, pericardial knock was interpreted as an S3, evidence of certain degree of CHF, which together with liver cirrhosis were considered the most likely initial diagnoses. Significant pulsus paradoxus of greater than 10 mm Hg is infrequently encountered in pure CP or in RCM. The constricting pericardium does not transmit changes in pleural pressures (see next section); therefore, the presence of pulsus paradoxus suggests coexistent pulmonary disease or effusive CP.21 III. PHYSIOLOGY AND PATHOLOGY The rigid, non-pliable shell that encases the heart in CP sharply accentuates the ventricular pressure-volume relationship through several mechanisms. First, intrathoracic and intracardiac pressures are dissociated during respiration. The effect of the respiratory cycle on intrathoracic blood flow in CP is critical to understanding the pathophysiologic features.22,23 Normally, inspiration decreases intrathoracic pressure, which is transmitted to all intrathoracic structures including the pulmonary veins and cardiac chambers. However, the encased pericardium of CP isolates the cardiac chambers from changes in intrathoracic pressure. Therefore, as intrathoracic pressures decrease during inspiration, cardiac pressures remain high. Less of a pressure gradient is created between the pulmonary veins and the left-sided chambers of the heart, resulting in less total pulmonary venous return and decreased flow velocity during inspiration. This results in a decrease in left ventricular filling with inspiration. The opposite effect is seen with expiration in CP. The second physiologic hallmark of CP results from marked ventricular interdependence. The total cardiac volume is fixed by the non-pliable pericardium. Therefore, the total amount of blood entering the heart does not vary significantly during the respiratory cycle. During expiration, the increase in the intrathoracic pressure does not affect the cardiac chambers. However, the pulmonary veins and venae cavae are not shielded by the rigid pericardium, and flow velocities in these vessels are affected. Consequently, flow into the left ventricle with expiration is increased. The ventricular septum is not directly affected by the pericardium and is free to bulge into the right ventricle causing reduction in flow velocity in the venae cavae and decreased trans-tricuspid flow velocity.24 Echocardiography demonstrates these changes in flow velocities, as discussed in the next section. The third major effect of the inflexible pericardium of CP on cardiac hemodynamics is impairment of diastolic filling. The non-pliable pericardium of CP limits diastolic filling in all cardiac chambers, resulting in elevated enddiastolic pressures. Normally, approximately 75% of ventricular filling occurs during phase 2 (rapid filling) of diastole, and 10% to 20% occurs during phase 4 (atrial contraction).15 Because of the elevated atrial pressures in CP, up to 75% to 80% of ventricular filling occurs in the first 25% to 30% of diastole.25 Filling rapidly declines by mid-diastole and filling is severely limited in late diastole. Tachycardia would adversely affect diastolic ventricular filling in a normal patient. In patients with CP, where nearly all ventricular filling occurs by mid-diastole, tachycardia becomes an important means of maintaining cardiac output. Consequently, tachycardia and atrial fibrillation are relatively less important in CP.26 The hallmark of chronic CP is a thickened adherent pericardial sac that restricts filling of the cardiac chambers. Pathologically, pericardial inflammation leads to the deposition of fibrous strands and proliferation of cellular infiltrates.27 Eventually, calcification occurs with total or near total obliteration of the pericardial space as well as the remaining fluid, pus, or blood. In some instances, loculated large collections of fluid may compress individual cardiac chambers. Additionally, bandlike constrictions can develop and compromise any portion of the heart, including the valve rings and great vessels, mimicking intrinsic disease of the affected structures.28,29 IV. DIAGNOSTIC IMAGING MODALITIES ELECTROCARDIOGRAPHY (ECG) FINDINGS • Can the 12-lead ECG and routine chest radiography assist diagnosis of CP? • What additional studies are necessary to accurately diagnose CP? No specific ECG abnormalities are characteristic for either CP or RCM. Low QRS voltage and nonspecific T-wave changes are common in both conditions. A compensatory sinus tachycardia is frequently present in RCM and CP, as seen in patient 1. Atrial fibrillation may be present in CP (up to 10% of patients) and RCM; Cardiology Volume 9, Part 2 5 Constrictive Pericarditis: A Case Study RV RA LV RV LV LA A B Figure 2. MRI of the pericardium in a patient with constrictive pericarditis. Progressive cardiac failure developed during a viral illness in a 76-year-old woman. Gated, T1-weighted, spin–echocardiogram MRI of the heart in the transverse axial view (A) and oblique sagittal view (B) showed diffuse thickening of the entire pericardium, calcifications (arrows in A), RA enlargement, a moderate amount of fluid between the 2 pericardial layers, and increased signal in the cavity, indicative of stasis of blood. LA = left atrium; LV = left ventricle; MRI = magnetic resonance imaging; RA = right atrial; RV = right ventricle. (Reprinted with permission from De Benedetti E, Didier D. Images in clinical medicine. Constrictive pericarditis. N Engl J Med 2000;343:107. Copyright © 2000 Massachusetts Medical Society. All rights reserved.) however, ventricular arrhythmias and abnormalities of conduction, including atrioventricular block, are seen more frequently in RCM. Because these findings are nonspecific, it is not surprising that an ECG tracing rarely can help to differentiate between RCM and CP. However, the presence of a completely normal tracing should lead the clinician to reconsider the diagnosis of CP or RCM. RADIOLOGIC IMAGING Chest Radiography Chest radiography as a single noninvasive imaging modality can occasionally help to distinguish CP from RCM. Pericardial calcification is best seen in the lateral view. “Eggshell” calcifications or amorphous calcifications in the atrioventricular grooves may be seen. Although calcification may support the clinical suspicion of CP, its presence is not always specific because it may occur without cardiac compression.30 Blood Pool Radionuclide Ventriculography Blood pool radionuclide ventriculography usually demonstrates that the elapsed time to peak filling is decreased during inspiration, which may be a finding unique to CP.31,32 Computed Tomography and Magnetic Resonance Imaging (MRI) CT and MRI are the best radiologic modalities to demonstrate pericardial thickening. When imaging with multislice spin-echo (gated) MRI, the normal pericardium appears as a thin (< 3 mm), low-intensity signal between the high-intensity signal of the epicardial fat 6 Hospital Physician Board Review Manual and the medium-intensity signal of the myocardium.33 Although pericardial fluid also has a low-signal intensity, fluid appears bright on ciné MRI images, allowing one to distinguish fluid from pericardium and to accurately assess the pericardial thickness. Pericardial thickening of 4 mm or more favors a diagnosis of CP, whereas thickening more than 6 mm is highly specific for CP (Figure 2).34 It should be mentioned that the pericardium can be constricting even when it is so thin that it is not recognized as abnormal by any contemporary imaging techniques. Nevertheless, pericardial thickening of more than 5 mm, an enlarged right atrium, and a distorted tubular right ventricle are all highly predictive of pericardial constricting disease.34 In some cases of heavy pericardial calcification, distinguishing between calcification and fibrous tissue may be difficult with MRI. In these cases, CT imaging of the pericardium may be better to assess pericardial thickness.22,35,36 Besides assisting in the diagnosis of CP, CT and MRI permit detailed planning of the surgical approach in patients by revealing the distribution and variations of pericardial thickness, calcification, and possible myocardial invasion. ECHOCARDIOGRAPHY No single pathognomic echocardiographic finding exists for CP. To distinguish CP from RCM, a combination of findings need to be used. Both M-mode and 2-dimensional echocardiography are not very helpful in making the distinction between these 2 conditions. In severe cases, the increased thickness and calcification of the pericardium can be seen with M-mode and 2-dimensional evaluation. Although evaluation of pericardial thickness with transthoracic echocardiography Constrictive Pericarditis: A Case Study is insensitive, measurement with a transesophageal echocardiogram (TEE) correlates strongly with measurements obtained by CT. One study demonstrated that the superior resolution achieved with TEE allowed better pericardial definition; a thickness of 3 mm or more on TEE was 95% sensitive and 86% specific for the detection of thickened pericardium.37 Doppler echocardiography and the relatively newer methods of color M-mode and tissue Doppler studies can differentiate CP from RCM. As previously mentioned, an important pathophysiologic consequence of CP is the greatly enhanced interventricular dependence resulting from a limited total cardiac volume with an uninvolved, freely moving septum. Thus, ventricular filling and emptying velocities assessed by mitral and tricuspid inflow velocities have much greater respiratory variation in CP in contrast to RCM where the interventricular septum is involved by the pathological process. Patients with CP have greatly exaggerated reciprocal variations in the rates of left and right ventricular filling related to the respiratory cycle when compared with normal subjects.38,39 In most patients with CP, mitral inflow velocity decreases as much as 25% and tricuspid velocity greatly increases with the first beat after inspiration. In contrast, respiratory variation in patients with RCM does not significantly differ from the normal. Doppler interrogation of the pulmonary and hepatic venous flow can further assist in the differentiation of these 2 conditions.40 These respiratory variations are illustrated in Figure 3. New Doppler methods have revealed that color Doppler M-mode evaluation of mitral inflow can help distinguish between RCM and CP. The flow propagation slope is steep in CP, whereas the same parameter is significantly lower in RCM (Figure 4).41 Additionally, tissue Doppler imaging has shown that patients with CP have a normal or a high normal early diastolic velocity (> 8 cm/sec), whereas patients with RCM have low early diastolic velocities (< 8 cm/sec; Figure 5).42 Doppler echocardiography has proven to be one of the most reliable noninvasive methods to help distinguish CP from RCM. tive process. Finally, catheterization provides information regarding the coronary anatomy in a patient who will undergo pericardiectomy and may need concomitant coronary artery bypass graft surgery. Although cardiac catheterization does not necessarily confirm the diagnosis of CP, Vaitkus and Kussmaul’s showed that the overall predictive accuracy of 3 major hemodynamic criteria can be very specific.43 A difference between right ventricular end diastolic (RVEDP) pressure and left ventricular end diastolic pressure (LVEDP) of 5 mm Hg or less, a right ventricular systolic pressure (RVSP) of 50 mm Hg or less, and a ratio of RVEDP to RVSP of 1:3 or more are 85%, 70%, and 76% sensitive, respectively, for correctly diagnosing CP. If all 3 of these criteria are met, a diagnosis of CP is correct in greater than 90% of patients. As previously discussed, the tight ventricular interaction in conjunction with insulation of the cardiac chambers from variations of intrathoracic pressures during the respiratory cycle are the 2 key mechanisms underlying the pathophysiology of CP. These fundamental principles explain why measuring respiratory variation in ventricular hemodynamics during catheterization is paramount in the diagnosis of CP.44 As a manifestation of ventricular interdependence, respiratory discordance occurs between the peak RVSP and left ventricular systolic pressure (LVSP) in CP. RVSP increases with inspiration as LVSP simultaneously decreases. The pulmonary capillary wedge pressure declines more than the LVEDP during inspiration, and the reduction in mitral valve inflow translates into the observed reduction in LVSP. In RCM, both the RVSP and LVSP decrease concordantly with inspiration.44 Several other findings on cardiac catheterization can assist in the diagnosis of CP such as increased distance between coronary arteries and the cardiac silhouette, which suggest the presence of thickened pericardium, as well as tethering of coronary arteries to the pericardium. V. HEMODYNAMICS • What is the definite therapy for CP? • What are the possible complications of complete pericardiectomy? Despite the availability of several noninvasive methods of assessment, cardiac catheterization is valuable when evaluating a patient with suspected RCM or CP. Catheterization permits quantification of left and right heart pressures. Additionally, endomyocardial biopsy can be performed and may identify coexisting cardiac disease or may confirm RCM resulting from an infiltra- VI. TREATMENT DISCUSSION The main reason that it is essential to distinguish RCM from CP is that the 2 disorders have distinctly different treatments. CP can be cured surgically with pericardiectomy. Although constrictive physiology Cardiology Volume 9, Part 2 7 Constrictive Pericarditis: A Case Study ECG E E E A S A D S D D ECG S A Apnea Apnea Inspiration Inspiration Normal Constrictive pericarditis A Expiration Restrictive myocardial disease Expiration Normal Constrictive pericarditis C Restrictive myocardial disease ECG E A E ECG E A A Apnea Apnea S D D S S Inspiration Inspiration Expiration Normal B Constrictive pericarditis Expiration Restrictive myocardial disease Normal D Constrictive pericarditis Restrictive myocardial disease Figure 3. Schematic representations of flow patterns (using Doppler echocardiography) in normal subjects, patients with constrictive pericarditis, and patients with restrictive cardiomyopathy. A simultaneous ECG tracing is shown across the top. (A) Respiratory variation across the mitral valve. (B) Respiratory variation in flow across the tricuspid valve. Changes in flow are opposite of those seen across the mitral valve. (C) Respiratory variation in pulmonary venous flow. (D) Respiratory variation in hepatic venous flow. A-wave = late diastolic filling from atrial contraction; D-wave = peak diastolic flow velocity; ECG = electrocardiographic; E-wave = early diastolic filling; S-wave = peak systolic flow velocity. (Adapted from Leung DY, Klein AL. Restrictive cardiomyopathy: diagnosis and prognostic implications. In: Otto CM, editor. Practice of clinical echocardiography. Philadelphia: WB Saunders; 1997:474, with permission from Elsevier Science.) occurring in acute pericarditis may revert spontaneously,45 surgical removal of the pericardium is necessary in most cases. Complete pericardiectomy is the operative procedure of choice; however, it is surgically challenging.46,47 Removal should be as extensive as possible; however, sometimes calcified islands must be left or a palliative meshing of the pericardium may be required to minimize damage to the coronary arteries and myocardium. Removal of adherent pericardium 8 Hospital Physician Board Review Manual may require a prolonged procedure complicated by hypotension and arrhythmias. Most patients respond well to surgery, but the reported operative mortality of 12% is significant.46 Some patients have immediate and often profuse postoperative diuresis, although others may take weeks to months to recover after surgery. Poorer results are seen in patients with inadequate resection, uncorrected coronary artery disease, higher New York Heart Association classifications, and Constrictive Pericarditis: A Case Study APEX LA A APEX LA Figure 4. Color Doppler M-mode of diastolic flow from the left atrium (LA) toward the ventricular apex as imaged from the 4-chamber view in patients with constrictive pericarditis (A) or restrictive cardiomyopathy (B). The flow propagation slope of the first aliasing contour (white line) is steep for constrictive pericarditis, but the slope is significantly slower in restrictive cardiomyopathy. Respiratory monitoring is shown with inspiration (up arrow) and expiration (down arrow). (Reprinted from Rajagopalan N, Garcia MJ, Rodriguez L, et al. Comparison of new Doppler echocardiographic methods to differentiate constrictive pericardial heart disease and restrictive cardiomyopathy. Am J Cardiol 2001;87:93, with permission from Excerpta Medica, Inc.) B older age. Patients with radiation-induced CP and those with peripheral organ failure involving the liver or kidneys with ascites and edema also have poorer postoperative outcomes.46 Occasionally, the chronic external support of the tight pericardium can lead to myocardial atrophy, which can sometimes be detected preoperatively by decreased myocardial signals on MRI or CT. Releasing the heart surgically may allow rapid dilation of the ventricle, leading to systolic dysfunction and heart failure.47,48 Patients dying with low cardiac output after complete pericardiectomy have histologic findings consistent with myocardial atrophy. When this condition is advanced, the heart may continue to dilate as it fails, resulting in what has been called the exploding heart syndrome. Fortunately, the condition is reversible in some patients if they can be assisted for several days with maximal medical and circulatory support.49 On the other hand, treatment of RCM is often symptomatic. Diuretics are frequently used to relieve systemic and pulmonary venous congestion, which must be done with caution because high filling pressures are needed to maintain ventricular filling in RCM. Excessive use of diuretics may reduce filling and lead to decreased cardiac output with resultant systemic hypoperfusion manifested by fatigue, lightheadedness, and prerenal azotemia. Careful monitoring for these findings should alert the clinician that further diuresis should be avoided. As discussed earlier, efficient diastolic filling is compromised in RCM, leading to the understanding that rate-lowering drugs (such as β-blockers and calcium channel antagonists) may have a beneficial role. Slowing the heart thus allows for more diastolic time in each cardiac cycle and for improved ventricular relaxation and filling. Angiotensin–converting enzyme inhibitors have a proven beneficial role in systolic dysfunction; evidence suggests they may be beneficial in diastolic dysfunction and thus have a role in treating RCM.50 Rhythm disturbances can be detrimental in patients with RCM. Atrial fibrillation worsens diastolic dysfunction because of the loss of the atrial contribution to ventricular filling. Additionally, a rapid ventricular response can further compromise patients with RCM. Attempts should be made to maintain sinus rhythm via cardioversion or antiarrhythmic drugs such as amiodarone. If sinus rhythm cannot be achieved or maintained, then adequate rate control is necessary, and anticoagulation with warfarin is recommended. In fact, the hypercoagulable propensity of particular etiologies of RCM warrant anticoagulation to prevent thrombus formation regardless of the patient’s rhythm.51 Cardiology Volume 9, Part 2 9 Constrictive Pericarditis: A Case Study Normal Restriction Constriction A 50 cm/s 50 cm/s 20 cm/s B 5 cm/s 5 cm/s 5 cm/s Figure 5. A normal subject, a patient with restrictive cardiomyopathy, and a patient with constrictive pericarditis: representative examples of the (A) mitral annular M-mode, (B) transmitral Doppler flow velocities, and (C) tissue Doppler axial velocities. A marked difference in early diastolic velocity (arrows) despite similar early transmitral flow velocities is observed. (Reprinted from Garcia MJ, Thomas JD, Klein AL. New Doppler echocardiographic applications for the study of diastolic function. J Am Coll Cardiol 1998;32:871, with permission from the American College of Cardiology Foundation.) C Infiltrative disorders may result in advanced conduction system disease. Dual chamber pacing should be used to maintain properly timed atrial contraction to improve ventricular filling. Advanced diastolic dysfunction secondary to RCM is associated with a poor prognosis in patients with secondary causes such as amyloidosis or hemochromatosis. Idiopathic RCM also has a poor outcome, with 64% and 37% survival at 5 and 10 years, respectively.52 Cardiac transplantation can be performed in patients with refractory symptoms in idiopathic or familial RCM. Combined heart and liver transplantation in patients with hemachromatosis has yielded good results.53 Although transplantation has been a treatment option for sarcoidosis and amyloidosis, recurrence can occur in the transplanted heart.54 – 56 DIAGNOSIS AND TREATMENT OF PATIENT 1 Thickening of the pericardium observed on CT scan in patient 1 assisted in establishing the diagnosis of CP, which was further supported by Doppler echocardiographic and hemodynamic data obtained during cardiac catheterization. Pericardial biopsy confirmed the diagnosis of CP, and subsequent pericardiectomy is successful. • • • • • • VII. SUMMARY POINTS • The fibrous pericardium envelops the entire heart and much of the ascending aorta, the main pulmonary 10 Hospital Physician Board Review Manual • artery, all 4 pulmonary veins, and portions of the inferior and superior venae cavae in patients with CP. Tuberculosis has historically been the leading cause of CP; however, neoplasm, collagen vascular disease, infectious etiologies, radiation therapy, and previous cardiovascular surgery are some of the more common causes of constriction in modern developed countries. Symptoms are typically insidious in onset and consist of poor appetite, cachexia, abdominal discomfort (because of splanchnic engorgement, ascites), and peripheral edema along with general fatigue and weakness. However, it is difficult to establish the diagnosis of CP or RCM on clinical grounds alone. A sharp Y-wave descent and a rapid ascent to the baseline in jugular venous pulsations are seen in CP, RCM, or severe right-sided heart failure. In patients with constrictive pericarditis, the rigid pericardium causes an abruptly amputated ventricular filling during diastole, resulting in a pericardial knock that may be made more prominent by having the patient squat. The rigid, inelastic “shell” that encases the heart in CP sharply accentuates the ventricular pressure-volume relationship through several mechanisms. Pericardial calcification is often seen on the lateral radiograph in CP. MRI is very accurate in assessing pericardial thickness; thickening of 4 mm or more favors a diagnosis of CP, whereas thickening greater than 6 mm is very specific for CP. Constrictive Pericarditis: A Case Study • Ventricular filling and emptying velocities as assessed by mitral and tricuspid inflow velocities have much greater respiratory variation in CP when compared with RCM. • New Doppler methods have revealed that color Doppler M-mode evaluation of mitral inflow can help distinguish between RCM and CP. • Cardiac catheterization can be used to diagnose CP. A difference between right ventricular end diastolic pressure (RVEDP) and left ventricular end diastolic pressure of 5 mm Hg or less, a right ventricular systolic pressure (RVSP) of 50 mm Hg or less, and a RVEDP to RVSP ratio of 1:3 or more are consistent with CP. • CP can be cured surgically with pericardiectomy; however, the reported operative mortality is 12%. REFERENCES 1. Shabetai R, Mangiardi L, Bhargava A, et al. The pericardium and cardiac function. Prog Cardiovasc Dis 1979;22: 107–34. 2. Shabetai R. The pericardium. New York: Grune & Stratton; 1981. 3. Hancock EW. Subacute effusive-constrictive pericarditis. Circulation 1971;43:183–92. 4. Hancock EW. On the elastic and rigid forms of constrictive pericarditis. Am Heart J 1980;100(6 Pt 1):917–23. 5. Myers RB, Spodick DH. Constrictive pericarditis: clinical and pathophysiologic characteristics. Am Heart J 1999; 138(2 Pt 1):219–32. 6. Roberts WI, Spray TL. Pericardial heart disease: a study of causes, consequences, and morphologic features. In: Spodick, DH, editor. Cardiovascular clinics. Vol 7. No. 3. Philadelphia: Davis; 1976:11–66. 7. Cameron J, Oesterle SN, Baldwin JC, Hancock EW. The etiologic spectrum of constrictive pericarditis. Am Heart J 1987;113(2 Pt 1):354–60. 8. Robertson R, Arnold CR. Constrictive pericarditis with particular reference to etiology. Circulation 1962;26:525–9. 9. Fowler NO. Tuberculous pericarditis. JAMA 1991;266: 99–103. 10. Abelmann WH. Classification and natural history of primary myocardial disease. Prog Cardiovasc Dis 1984;27: 73–94. 11. Leung DY, Klein AL. Restrictive cardiomyopathy: diagnosis and prognostic implications. In: Otto CM, editor. The practice of clinical echocardiography. Philadelphia: W. B. Saunders; 1997:474. 12. Kushwaha SS, Fallon JT, Fuster V. Restrictive cardiomyopathy. N Engl J Med 1997;336:267–76. 13. Backes RJ, Gersh BJ. Cardiomyopathies in the elderly. Cardiovasc Clin 1992;22:105–25. 14. Schoenfeld MH. The differentiation of restrictive cardiomyopathy from constrictive pericarditis. Cardiol Clin 1990;8:663–71. 15. Goodwin JF. Cardiomyopathies and specific heart muscle diseases. Definitions, terminology, classifications and new and old approaches. Postgrad Med J 1992;68(Suppl 1): S3–6. 16. Killian DM, Furiasse JG, Scanlon PJ, et al. Constrictive pericarditis after cardiac surgery. Am Heart J 1989;118: 563–8. 17. Nataf P, Cacoub P, Dorent R, et al. Results of subtotal pericardiectomy for constrictive pericarditis. Eur J Cardiothorac Surg 1993;7:252–5. 18. Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999;100:1380–6. 19. Fuster V, Alexander RW, O’Rourke RA, et al, editors. Hurst’s the heart. 10th ed. New York: McGraw-Hill Medical Publishing Division; 2001:228–9. 20. Nicholson WJ, Cobbs BW Jr, Franch RH, Crawley IS. Early diastolic sound of constrictive pericarditis. Am J Cardiol 1980;45:378–82. 21. Spodick DH. The normal and diseased pericardium: current concepts of pericardial physiology, diagnosis and treatment. J Am Coll Cardiol 1983;1:240–51. 22. Oh JK, Hatle LK, Seward JB, et al. Diagnostic role of Doppler echocardiography in constrictive pericarditis. J Am Coll Cardiol 1994;23:154–62. 23. Senni M, Redfield MM, Ling LH, et al. Left ventricular systolic and diastolic function after pericardiectomy in patients with constrictive pericarditis: Doppler echocardiographic findings and correlation with clinical status. J Am Coll Cardiol 1999;33:1182–8. 24. Santamore WP, Bartlett R, Van Buren SJ, et al. Ventricular coupling in constrictive pericarditis. Circulation 1986;74: 597–602. 25. Wolfe MW, Edelman ER. Transient systolic dysfunction after relief of cardiac tamponade. Ann Intern Med 1993; 119:42–4. 26. Braverman AC, Sundaresan S. Cardiac tamponade and severe ventricular dysfunction [letter]. Ann Intern Med 1994;120:442. 27. Holt JP. The normal pericardium. Am J Cardiol 1970; 26:455–65. 28. Nishimura RA, Kazmier F, Smith HC, Danielson GK. Right ventricular outflow obstruction caused by constrictive pericardial disease. Am J Cardiol 1985;55:1447–8. 29. Vallance PJ, Gray HH, Oldershaw PJ. Diagnostic features of localised pericardial constriction. Int J Cardiol 1988; 20:416–9. Cardiology Volume 9, Part 2 11 Constrictive Pericarditis: A Case Study 30. McGregor JH, Chen JT, Chiles C, et al. The radiographic distinction between pericardial and myocardial calcification. AJR Am J Roentgenol 1987;148:675–7. dynamic respiratory changes in left and right ventricular pressure for the diagnosis of constrictive pericarditis. Circulation 1996;93:2007–13. 31. Aroney CN, Ruddy TD, Dighero H, et al. Differentiation of restrictive cardiomyopathy from pericardial constriction: assessment of diastolic function by radionuclide angiography. J Am Coll Cardiol 1989;13:1007–14. 45. Sagrista-Sauleda J, Permanyer-Miralda G, Candell-Reira J, et al. Transient cardiac constriction: an unrecognized pattern of evolution in effusive acute idiopathic pericarditis. Am J Cardiol 1987;59:961–6. 32. Gerson MC, Colthar MS, Fowler NO. Differentiation of constrictive pericarditis and restrictive cardiomyopathy by radionuclide ventriculography. Am Heart J 1989;118: 114–20. 46. DeValeria PA, Baumgartner WA, Casale AS, et al. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg 1991;52:219–24. 33. White CS. MR evaluation of the pericardium. Top Magn Reson Imaging 1995;7:258–66. 47. McCaughan BC, Schaff HV, Piehler JM, et al. Early and late results of pericardiectomy for constrictive pericarditis. J Thorac Cardiovasc Surg 1985;89:340–50. 34. Soulen RL, Stark DD, Higgins CB. Magnetic resonance imaging of constrictive pericardial disease. Am J Cardiol 1985;55:480–4. 48. Douglas JM. The pericardium. In: Sabiston DC, Spencer FC, editors. Surgery of the chest. 6th ed. Philadelphia: W. B. Saunders; 1995:1365–86. 35. Olson MC, Posniak HV, McDonald V, et al. Computed tomography and magnetic resonance imaging of the pericardium. Radiographics 1989;9:633–49. 49. Levine HD. Myocardial fibrosis in constrictive pericarditis. Electrocardiographic and pathologic observations. Circulation 1973;48:1268–81. 36. O’Keefe D, McCarthy P, O’Regan P. Computed tomography in constrictive pericarditis. Ir Med J 1984;77:172–4. 50. Friedrich SP, Lorell BH, Rousseau MF, et al. Intracardiac angiotensin-converting enzyme inhibition improves diastolic function in patients with left ventricular hypertrophy due to aortic stenosis. Circulation 1994;90:2761–71. 37. Ling LH, Oh JK, Tei C, et al. Pericardial thickness measured with transesophageal echocardiography feasibility and potential clinical usefulness. J Am Coll Cardiol 1997; 29:1317–23. 38. Mertens LL, Denef B, DeGeest H. The differentiation between restrictive cardiomyopathy and constrictive pericarditis: the impact of the imaging techniques. Echocardiography 1993;10:497–508. 39. Hatle LK, Appleton CP, Popp RL. Differentiation of constrictive pericarditis and restrictive cardiomyopathy by Doppler echocardiography. Circulation 1989;79:357–70. 51. Gottdiener JS, Maron BJ, Schooley RT, et al. Twodimensional echocardiographic assessment of the idiopathic hypereosinophilic syndrome. Anatomic basis of mitral regurgitation and peripheral embolization. Circulation 1983;67:572–8. 52. Ammash NM, Seward JB, Bailey KR, et al. Clinical profile and outcome of idiopathic restrictive cardiomyopathy. Circulation 2000;101:2490–6. 40. Klein AL, Cohen GI. Doppler echocardiographic assessment of constrictive pericarditis, cardiac amyloidosis, and cardiac tamponade. Cleve Clin J Med 1992;59:278–90. 53. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 31-1994. A 25-yearold man with the recent onset of diabetes mellitus and congestive heart failure. N Engl J Med 1994;331:460–6. 41. Rajagopalan N, Garcia MJ, Rodriguez L, et al. Comparison of new Doppler echocardiographic methods to differentiate constrictive pericardial heart disease and restrictive cardiomyopathy. Am J Cardiol 2001;87:86–94. 54. Deng M, Park JW, Roy-Chowdury R, et al. Heart transplantation for restrictive cardiomyopathy: development of cardiac amyloidosis in preexisting monoclonal gammopathy. J Heart Lung Transplant 1992;11(1 Pt 1):139–41. 42. Garcia MJ, Thomas JD, Klein AL. New Doppler echocardiographic applications for the study of diastolic function. J Am Coll Cardiol 1998;32:865–75. 55. Dubrey S, Simms RW, Skinner M, Falk RH. Recurrence of primary (AL) amyloidosis in a transplanted heart with four-year survival. Am J Cardiol 1995;76:739–41. 43. Vaitkus PT, Kussmaul WG. Constrictive pericarditis versus restrictive cardiomyopathy: a reappraisal and update of diagnostic criteria. Am Heart J 1991;122:1431–41. 56. Oni AA, Hershberger RE, Norman DJ, et al. Recurrence of sarcoidosis in a cardiac allograft: control with augmented corticosteroids. J Heart Lung Transplant 1992; 11(2 Pt 1):367–9. 44. Hurrell DG, Nishimura RA, Higano ST, et al. Value of Copyright 2003 by Turner White Communications Inc., Wayne, PA. All rights reserved. 12 Hospital Physician Board Review Manual