Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
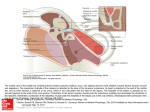
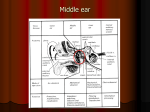
Build-A-Box A STEPWISE APPROACH TO MIDDLE EAR ANATOMY J McCarty | J Dornhoffer | R Riascos | E Angtuaco | RT Fitzgerald #1444 eEdE-156 PURPOSE & DISCLOSURE ANATOMY IMAGING PATHOLOGY MCQ’S To provide a step-by-step approach to the complex anatomy of the middle ear – building the tympanic cavity “box” and all of its contents from the ground up. John L. Dornhoffer, MD - inventor of the Olympus Dornhoffer Interpositional PORP Prosthesis, Dornhoffer HAPEX PORP/TORP & Dornhoffer Micron Titanium Footplate Shoes The remaining authors have no disclosures. THE BOX Introduction The tympanic cavity and its contents comprise the middle ear. Although irregularly shaped, this cavity within the temporal bone has been compared to a box with 6 sides. However, the tympanic cavity floor & roof are more spherical, bowing outward from the center of the cavity. THE EAR Introduction The ear is divided into 3 parts. + + External Middle Inner Pinna & External Auditory Canal Tympanic Cavity & All of Its Contents Cochlea, Vestibule, Semicircular Canals Sound Collection Sound Conduction Nerve Impulse Formation It is useful to keep a broad understanding of ear anatomy and function in mind when studying the detailed subject of otology. STEP 1: OSSICULAR CHAIN The middle ear aids in sound conduction. Ossicles The tympanic membrane converts sound collected by the external ear into vibrations. The ossicles then transmit and amplify sound towards the oval window and inner ear. Ossicular Chain = Malleus + Incus + Stapes OSSICULAR CHAIN ANATOMY Ossicles Head of the Malleus Anterior Process of the Malleus Lateral Process of the Malleus Manubrium of the Malleus Tympanic Membrane LATERALLateral Short Process of the Incus Long Process of the Incus Footplate of the Stapes Anterior Crus of the Stapes Lenticular Process of the Incus MEDIAL CT OF THE OSSICULAR CHAIN 3DVR Ossicles Axial Coronal Head MALLEUS Lateral Process Short Process Body Long Process Lenticular Process Capitellum Anterior Crus STAPES Posterior Crus Head Handle Handle Lateral Process INCUS Head Head Neck Sagittal Footplate Body Long Process Short Process Capitellum Posterior Crus Anterior Crus Body Short Process Body Lenticular Process Anterior Crus Capitellum Posterior Crus CASE BASED MULTIPLE CHOICE QUESTION (MCQ) CASE 1 Case 1 is an example of a: Ossicles Malleal & incudal prosthesis Coronal “TORP” = Total Ossicular Replacement Prosthesis “PORP” = Partial Ossicular Replacement Prosthesis A. B. C. D. Foreign body Stapedial prosthesis PORP TORP The most common repairable cause of ossicular prosthetic failure is: A. Migration B. Recurrent cholesteatoma C. Trauma Native stapes Axial Prostheses may migrate or dislocate. Stapes prostheses most commonly migrate inferiorly. Occasionally one may migrate medially through the oval window STEP 2: MUSCULATURE Muscles STAPEDIUS TENSOR TYMPANI Dampens Sound Dampens Sound Attaches to Head of the Stapes Attaches to Neck of the Malleus Innervation: CN VII Innervation: V3 Two Muscles: Stapedius + Tensor Tympani AXIAL IMAGING Muscles The tensor tympani is a thin elongated muscle that resides superior to the Eustachian tube. Only a small portion of this muscle traverses the tympanic cavity. Tensor Tympani Tensor Tympani 1 2 3 4 1 Eustachian Tube 2 Eustachian Tube The stapedius is not well visualized on CT. 3 4 Sequential axial images (1 = cranial, 4 = caudal) CASE BASED MCQ CASE 2 Tumor invasion of the facial nerve tympanic segment would cause: Muscles 2 1 A. Hyperaccusis B. Conductive hearing loss C. Sensorineural hearing loss Axial Damage to the proximal facial nerve could lead to denervation of the stapedius and inability to adequately dampen sound. Facial nerve segments labeled 1 & 2 on the coronal image are: A. B. C. D. Canalicular & genu Genu & labyrinthine Labyrinthine & tympanic Tympanic & mastoid Coronal The “snails eyes” are the labyrinthine & tympanic segments of the facial nerve on coronal CT. STEP 3: LIGAMENTOUS SUPPORT Superior Malleal Ligament Ligaments Posterior Incudal Ligament Anterior Malleal Ligament Several ligaments stabilize the suspended ossicular chain. MALLEAL SUPPORT Anterior Malleal Ligament TEGMEN TYMPANI (attachment) * Superior Malleal Ligament Ligaments SCUTUM Lateral Malleal Ligament The malleus has the strongest support of the 3 ossicles. 4 Ligaments + Tensor Tympani Muscle INCUDAL & STAPEDIAL SUPPORT Annular Ligament Posterior Incudal Ligament Stapedius Ligaments Incudostapedial Joint INCUDAL STAPEDIAL The single posterior incudal ligament stabilizes the incus within the tympanic cavity. The annular ligament surrounds the footplate of the stapes, and stabilizes it to the oval window. AXIAL IMAGING Anterior Malleal Ligament Ligaments Posterior Incudal Ligament The ligaments stabilizing the ossicular chain may not be well visualized on CT. However, here the posterior incudal and anterior malleal ligaments are seen CASE BASED MCQ CASE 3 Incudal body Malleal head Ligaments Which ossicle is most commonly dislocated secondary to trauma? A. Malleus B. Incus C. Stapes CASE 4 Incudal body Malleal head The incus is the largest ossicle. It also happens to have the weakest support. Axial Laterally dislocated incus abuts the lateral wall of the epitympanum. Ice cream that fell of the cone. What is the most common ossicular traumatic injury? A. Incudal fracture B. Malleal fracture C. Malleoincudal joint disruption D. Incudostapedial joint disruption Although malleoincudal joint disruption is more often identified on CT, incudostapedial disruptions occur more often. Axial Disruption of the malleoincudal joint without lateral incudal displacement. Ice cream only separated from cone. STEP 4: NERVES Nerves JACOBSON’S N. CHORDA TYMPANI Branch of CN IX Branch of CN VII Courses over Cochlear Prominence Innervation: Sensory Courses b/w Incus & Malleus Innervation: Taste Anterior 2/3 of Tongue TRAVERSING NERVES Nerves In & Around the Middle Ear Nerves Course Innervation JACOBSON’S N. CHORDA TYMPANI CN IX CN VII TYMPANIC STAPEDIUS N. SEGMENT OF FACIAL N. CN VII CN VII MASTOID SEGMENT OF FACIAL N. CN VII Inferior Mastoid Arises close Pyramidal tympanic Medial wall of segment origin to pyramidal eminence to canaliculus tympanic B/w incus & eminence stylomastoid cochlear cavity malleus stapedius foramen prominence Sensory Taste Anterior 2/3 of Tongue Stapedius * * AXIAL IMAGING 1 CN VII Tympanic segment 3 CN VII Mastoid Segment 1 Nerves 2 3 2 CN VII Posterior Genu 4 CN VII Mastoid Segment 4 Sequential axial images (1 = cranial, 4 = caudal) CASE BASED MCQ CASE 5 Malleal Handle Nerves Red Mass What are the findings on clinical otoscopy? A. Red retrotympanic mass B. Blue retrotympanic mass C. White retrotympanic mass There’s a small red retrotympanic mass overlying the cochlear promontory without underlying erosions. Otoscopy Retracted TM Promontory Otoscopy Stapedial Head Red Mass A. B. C. D. Rounded mass on the promontory Intact middle ear floor Coronal What is the most likely diagnosis? Glomus tympanicum Glomus jugulotympanicum Aberrant carotid artery Persistent stapedial artery Glomus jugulotympanicum would have dehiscence of the middle ear floor & warrant a different surgical approach. Specimen STEP 4: NERVES Nerves TYPE LOCATION NERVE PARAGANGLIA Glomus Tympanicum Cochlear Promontory CN IX (Jacobson’s) Glomus Jugulare Jugular Foramen CN X Glomus Vagale B/w ICA & IJ CN X Carotid Body Glomus Carotid bifurcation (splaying ICA & ECA) CN X “Glomus” = “Paraganglioma” Arise from paraganglia (normal structures which accompany CN & ganglia) STEP 5: WALLS “Roof” or Tegmen Tympani Pyramidal Eminence “Posterior” or Mastoid Wall Walls Facial N. Recess “Medial” or Labyrinthine Wall Sinus Tympani “Floor” or Jugular Wall “Anterior” or Carotid Wall AXIAL IMAGING Anterior Wall Anterior Wall Medial wall 1 2 Walls 1 CP AAA h 2 3 4 E 5 6 Lateral Wall/TM CP FR PE ST Posterior Wall E Medial wall 4 CP CC Lateral Wall/ TM CC JB RW 5 6 Floor AAA = aditus ad antrum, E = Eustachian tube, Co = Cochlea, CP = cochlear promontory, ST = sinus tympani, PE = pyramidal eminence, FR = facial recess, RW = round window, CC = carotid canal, JB = jugular bulb CASE BASED MCQ CASE 6 TM Stellate mass From which structure does the mass arise? A. Tympanic Membrane B. Ossicular Chain C. Tegmen Tympani Stellate mass A soft tissue attenuation stellate mass arising from the TM projects into the external auditory canal. Walls A. B. C. This mass arises from the TM – the D. Coronal lateral wall of the middle ear – and protrudes into the EAC. What is the most likely diagnosis? Squamous Cell Carcinoma Cerumen Verruca Vulgaris Glomus A benign cutaneous wart cause by human papillomavirus (HPV). Axial TM involvement is very rare – until 2013, there were no reports of verruca on the TM in the English literature. CASE BASED MCQ CASE 7 Permeative changes Rounded mass Walls Coronal This mass causes permeative changes of the tympanic cavity floor and protrudes into the middle ear. A. B. C. D. What is the diagnosis? Cholesteatoma Glomus Tympanicum (GTP) Glomus Jugulotympanicum (GJP) Metastasis Mass A destructive soft tissue mass erodes through the middle ear floor and extends superiorly – overlying the cochlear promontory. This mass arises in association with which nerve? A. CN VII B. CN VIII C. CN IX D. CN X Arnold’s Nerve – a branch of CN X. Axial Involvement of the middle ear floor is the distinguishing factor differentiating GTP from GJP and necessitates a different surgical approach. STEP 6: SPACES Epitympanum Mesotympanum Spaces Hypotympanum The middle ear is further divided into several spaces. CROSS SECTIONAL IMAGING Protympanum Epitympanum Mesotympanum Mesotympanum Posterior Tympanum Hypotympanum Spaces Coronal CT Axial CT CASE BASED MCQ CASE 7 Epitympanic mass In which space does the mass reside? A. Protympanum B. Mesotympanum C. Prussak’s A small soft tissue mass resides in the epitympanum, eroding the TM. Spaces Coronal This mass extends through Prussak’s space, blunts the scutum and abuts the TM. What is the most likely diagnosis? A. Cholesteatoma B. SCC C. Cerumen Cholesteatomas can be either congenital (2%) or acquired (98%). Epitympanic mass Otoscopy Acquired cholesteotomas are most often seen in the epitympanum, medial to the pars flaccida (82%). PRUSSAK’S SPACE Malleal Neck Lateral Malleal Ligament Lateral Process Spaces Prussak’s Space Tympanic Membrane Coronal STEP 7: ADJACENT STRUCTURES Aditus Ad Antrum Eustachian Tube Adjacent Cochlear Promontory Round Window Oval Window AXIAL IMAGING FN 1 2 Co CP AAA CP TT h 1 2 3 4 E 5 E TM 6 TM CC CC JB Adjacent CP 4 FR PE ST RW 5 6 AAA = aditus ad antrum, FN = facial nerve, TT = tensor tympani, E = Eustachian tube, Co = Cochlea, CP = cochlear promontory, ST = sinus tympani, PE = pyramidal eminence, FR = facial recess, RW = round window, CC = carotid canal, JB = jugular bulb CASE BASED MCQ CASE 7 Thinned posterior wall What is the most likely diagnosis? A. High riding jugular bulb B. Aberrant carotid artery C. Glomus jugulotympanicum JB A. B. C. D. An enlarged & high riding jugular bulb Axial Adjacent The carotid canal is normal & there is no permeative destruction of the floor. What is the most common clinical presentation? Sensorineural hearing loss Conductive hearing loss Pulsatile tinnitus Otalgia extends along the middle ear floor GTP, GJP, & aberrant ICA’s also present with tinnitus. JB Coronal The overlying bone is thin and remodeled. FINAL MIDDLE EAR BOX Stapedius Aditus Ad Antrum Ossicular Chain Tensor Tympani Pyramidal Eminence Eustachian Tube Facial N. Recess Chorda Tympani N. Sinus Tympani Cochlear Promontory Round Window Final Box Oval Window Jacobson’s N. REFERENCES • • • • • • • • • • • • • • • • • • • • • • • Baráth, K., Huber, A. M., Stämpfli, P., Varga, Z., & Kollias, S. (2011). Neuroradiology of cholesteatomas. AJNR. American Journal of Neuroradiology, 32(2), 221–229. Fatterpekar, G. M., Doshi, A. H., Dugar, M., Delman, B. N., Naidich, T. P., & Som, P. M. (2006). Role of 3D CT in the evaluation of the temporal bone. Radiographics, 26 Suppl 1, S117–32. Han, W. W., Incesulu, A., McKenna, M. J., Rauch, S. D., Nadol, J. B. J., & Glynn, R. J. (1997). Revision stapedectomy: intraoperative findings, results, and review of the literature. The Laryngoscope, 107(9), 1185–1192. Hesselink, J. R., Davis, K. R., & Taveras, J. M. (1981). Selective arteriography of glomus tympanicum and jugulare tumors: techniques, normal and pathologic arterial anatomy. AJNR. American Journal of Neuroradiology, 2(4), 289–297. Juliano, A. F., Ginat, D. T., & Moonis, G. (2013). Imaging review of the temporal bone: part I. Anatomy and inflammatory and neoplastic processes. Radiology, 269(1), 17–33. Juliano, A. F., Ginat, D. T., & Moonis, G. (2015). Imaging Review of the Temporal Bone: Part II. Traumatic, Postoperative, and Noninflammatory Nonneoplastic Conditions. Radiology, 276(3), 655–672. Lane, J. I., Lindell, E. P., Witte, R. J., DeLone, D. R., & Driscoll, C. L. W. (2006). Middle and inner ear: improved depiction with multiplanar reconstruction of volumetric CT data. Radiographics, 26(1), 115–124. Lee, T. C., Aviv, R. I., Chen, J. M., Nedzelski, J. M., Fox, A. J., & Symons, S. P. (2009). CT grading of otosclerosis. AJNR. American Journal of Neuroradiology, 30(7), 1435–1439. Lemmerling, M. M., Stambuk, H. E., Mancuso, A. A., Antonelli, P. J., & Kubilis, P. S. (1997a). CT of the normal suspensory ligaments of the ossicles in the middle ear. AJNR. American Journal of Neuroradiology, 18(3), 471–477. Lemmerling, M. M., Stambuk, H. E., Mancuso, A. A., Antonelli, P. J., & Kubilis, P. S. (1997b). Normal and opacified middle ears: CT appearance of the stapes and incudostapedial joint. Radiology, 203(1), Mas-Estelles, F., & Mateos-Fernández, M. (2012). Contemporary non–echo-planar diffusion-weighted imaging of middle ear cholesteatomas. Radiographics. Mukherji, S. K., Mancuso, A. A., Kotzur, I. M., Slattery, W. H., Swartz, J. D., Tart, R. P., & Nall, A. (1994). CT of the temporal bone: findings after mastoidectomy, ossicular reconstruction, and cochlear implantation. AJR. American Journal of Roentgenology, 163(6), 1467–1471. Netter FH. Atlas of Human Anatomy. Elsevier Health Sciences; 2010. Nikolaidis, V. (2011). Traumatic dislocation of the incudostapedial joint repaired with fibrin tissue adhesive. The Laryngoscope, 121(3), 577–579. Petrus, L. V., & Lo, W. W. (1997). The anterior epitympanic recess: CT anatomy and pathology. AJNR. American Journal of Neuroradiology, 18(6), 1109–1114. Phillips, G. S., LoGerfo, S. E., Richardson, M. L., & Anzai, Y. (2012). Interactive Web-based learning module on CT of the temporal bone: anatomy and pathology. Radiographics, 32(3), E85–105. Rowe, T. (1996). Coevolution of the mammalian middle ear and neocortex. Science. Stone, J. A., Mukherji, S. K., Jewett, B. S., Carrasco, V. N., & Castillo, M. (2000). CT evaluation of prosthetic ossicular reconstruction procedures: what the otologist needs to know. Radiographics, 20(3), 593–605. Shangkuan, W.-C., & Lin, M.-Y. (2014). Verruca vulgaris of tympanic membrane treated with topical immunotherapy. American Journal of Otolaryngology, 35(2), 242–245. Vattoth, S., Shah, R., & Curé, J. K. (2010). A compartment-based approach for the imaging evaluation of tinnitus. AJNR. American Journal of Neuroradiology, 31(2), 211–218. Weissman, J. L., & Hirsch, B. E. (1998). Beyond the promontory: the multifocal origin of glomus tympanicum tumors. AJNR. American Journal of Neuroradiology, 19(1), 119–122. Williams, M. T., Ayache, D., Elmaleh, M., Héran, F., Elbaz, P., & Piekarski, J. D. (2000). Helical CT findings in patients who have undergone stapes surgery for otosclerosis. AJR. American Journal of Roentgenology, 174(2), 387–392. Zayas, J. O., Feliciano, Y. Z., Hadley, C. R., Gomez, A. A., & Vidal, J. A. (2011). Temporal bone trauma and the role of multidetector CT in the emergency department. Radiographics, 31(6), 1741–1755. THANK YOU Jennifer McCarty, MD Roy Riascos, MD Twitter: @JMcCartyMD Email: [email protected] PGY5 Radiology Resident Department of Radiology University of Arkansas for Medical Sciences Associate Professor of Neuroradiology Chief, Division of Neuroradiology The University of Texas Health Sciences Center at Houston John L. Dornhoffer, MD, FACS Professor of Professor and Vice-Chair Samuel McGill Chair in Otolaryngology Research Department of Otolaryngology University of Arkansas for Medical Sciences Ryan T. Fitzgerald MD Assistant Professor of Radiology Department of Radiology, Neuroradiology Division University of Arkansas for Medical Sciences Edgardo Angtuaco, MD, FACR Professor, Department of Radiology Chief, Division of Neuroradiology and MRI University of Arkansas for Medical Sciences