Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
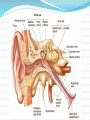
By Dr. Baseem N. Abdulhadi ENT Specialist CABMS (ENT), FIBMS (ENT) Sensory supply of the auricle Arterial supply of the auricle: 1) Anterior auricular branches from the superficial temporal artery. 2) Posterior auricular artery from the external carotid artery . 3) Branch from the occipital artery. The External auditor y canal The external auditory canal: • It does not follow a straight course. • It passes upward in an anterior direction, then turns slightly posteriorly still passing upward, and finally turns again in an anterior direction with a slight descent. • On otoscopic examination: gentle traction of the auricle superiorly, posteriorly and slightly laterally is needed to straighten the external auditory canal. Clinical correlates: Otitis externa is an inflammation of the external ear, usually from moisture in the canal leading to bacterial or fungal infection (swimmer’s ear) or to an infected hair follicle (boil). The condition can be painful because of tightness of the skin lining the canal that is abundantly innervated. Increased pain from traction on the auricle or opening the jaw helps distinguish otitis externa from otitis media. Right tympanic membrane The middle ear (tympanic cavity): It is an air-filled, mucous membrane-lined cavity in the temporal bone between the tympanic membrane laterally and the lateral wall of the inner ear medially. It consists of two parts: 1. The tympanic cavity proper: immediately adjacent to the tympanic membrane. 2. The epitympanic recess: superiorly. Boundaries (Walls) of the middle ear: The middle ear has 6 walls: 1. Roof (tegmental wall). 2. Floor (jugular wall). 3. Lateral wall (membranous wall). 4. Medial wall (labrynthine wall). 5. Posterior wall (mastoid wall). 6. Anterior wall (carotid wall). Contents of the middle ear: 1) Auditory ossicles (malleus, incus, and stapes). 2) Stapedius and tensor tympani muscles. 3) Chorda tympani nerve, a branch of CN VII. 4) Tympanic plexus nerves. Movements of the auditory ossicles Paralysis of the stapedius muscle: In patients with facial nerve paralsy, paralysis of the stapedius muscle is associated with excessive acuteness of hearing called hyperacusis; this condition results from uninhibited movements of the stapes Clinical correlates: Ear pain (otalgia) may be referred from the nasal cavity and paranasal sinuses via the trigeminal nerve, from the pharynx and larynx via the glosspharyngeal and vagus nerves, and from the cervical spine via spinal nerves. Otalgia may be associated with nausea and vomiting, a response mediated through the vagus nerve and its innervation of the upper gastrointestinal tract. The inner ear: 1) The bony labyrinth. a. Bony cochlea. b. Vestibule. Filled with perilymph c. Three semicircular canals. 2) The membranous labyrinth. a. Cochlear duct. b. Utricle and saccule. c. Three semicircular ducts. Filled with endolymph The cochlea: cross section Clinical correlates: Otosclerosis is a condition of abnormal bone formation around the stapes and the oval window, limiting the movement of the stapes and thus resulting in progressive conduction deafness. Conductive deafness is hearing impairment caused by a defect of a sound-conducting apparatus such as the auditory meatus, eardrum, or ossicles. Neural or sensorineural deafness is hearing impairment because of a lesion of the auditory nerve or the central afferent neural pathway. Meniere Syndrome (endolymphatic hydrops): It is related to excess endolymph production or blockage of the endolymphatic duct. Characterized by: 1. Tinnitus. 2. Hearing loss. 3. Vertigo. Thank you