Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Eradication of infectious diseases wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
Cross-species transmission wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Diseases of poverty wikipedia , lookup
HIV and pregnancy wikipedia , lookup
Henipavirus wikipedia , lookup
Focal infection theory wikipedia , lookup
Index of HIV/AIDS-related articles wikipedia , lookup
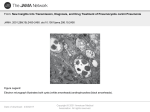
Journal de Mycologie Médicale (2009) 19, 270—275 CONGRESS OF THE FRENCH SOCIETY OF MEDICAL MYCOLOGY — NOVEMBER 29, 2008, PARIS/CONGRÈS SFMM — 29 NOVEMBRE 2008, PARIS Epidemiology of Pneumocystis infection in Human§ Épidémiologie de l’infection par Pneumocystis chez l’homme E.J. Calderón Instituto de Biomedicina de Sevilla, CIBER de Epidemiologı́a y Salud Pública, Servicio de Medicina Interna, Virgen del Rocı́o University Hospital, Avda Manuel Siurot s/n, 41013 Seville, Spain Received 28 June 2009; accepted 29 August 2009 Available online 23 October 2009 KEYWORDS Pneumocystis; Epidemiology; Transmission; Colonization MOTS CLÉS Pneumocystis ; Épidémiologie ; Summary Pneumocystis jirovecii (P. jirovecii) is an atypical fungus that causes pneumonia in immunosuppressed individuals and significant questions about its epidemiology and transmission remain unanswered. It is widely accepted that animal sources of P. jirovecii can be excluded because the Pneumocystis organisms that infect mammalian species are characterized by strong, close host species specificity. Similarly, an environmental reservoir of infection has not been found. Airborne transmission has been demonstrated in animal models and is assumed among humans. Highly sensitive PCR-technologies have allowed the detection of low numbers of Pneumocystis organisms in respiratory samples from colonized individuals who do not have Pneumocystis pneumonia. Studies have shown that individuals who have underlying Human immunodeficiency virus (HIV)-infection or other types of immunosuppression and those who are not immunosuppressed but have a chronic lung disease are often colonized by P. jirovecii. Further hypotheses claim that these groups may play a role in person-to-person transmission and that they may serve as reservoirs for future Pneumocystis infection in other susceptible individuals. On the other hand, P. jirovecii DNA was recently identified by molecular techniques in 35% of foetal lung and 5% of placenta samples from nonimmunodepressed women, who had a miscarriage, evidencing transplacental transmission in humans. Vertical transmission of P. jirovecii in humans could be an additional route of transmission of this stenoxenic microorganism that would ensure the persistence of Pneumocystis independent of environmental hazards. However, further studies are needed to confirm the role of this transmission route in the epidemiology of Pneumocystis infection in humans. # 2009 Elsevier Masson SAS. All rights reserved. Résumé Pneumocystis jirovecii (P. jirovecii) est un champignon atypique responsable de pneumonie chez les sujets immunodéprimés. Des questions significatives sur l’épidémiologie et la transmission demeurent sans réponse. On accepte en général que les animaux ne constituent pas une source d’infection pour l’homme car les Pneumocystis des divers mammifères présen- § Conférence présentée au symposium « Pneumocystis et pneumocystose 100 ans après », Présidence Patricia Roux et Eduardo Dei-Cas, faculté de médecine Necker, Paris le 29 novembre 2008. Adresse e-mail : [email protected]. 1156-5233/$ — see front matter # 2009 Elsevier Masson SAS. All rights reserved. doi:10.1016/j.mycmed.2009.08.001 Epidemiology of Pneumocystis infection in Human 271 Transmission ; Colonisation tent une très étroite spécificité d’hôte. Similairement, il n’y a pas d’évidence d’un réservoir environnemental. La transmission aérienne a été démontrée chez les modèles animaux et l’on suppose qu’elle existe aussi dans les populations humaines. Des techniques PCR hautement sensibles ont permis de détecter des faibles taux de Pneumocystis dans des échantillons pulmonaires de sujets colonisés par le champignon mais sans pneumonie. Des recherches ont montré que les patients VIH positifs ou immunodéprimés par d’autres causes ainsi que des sujets non immunodéprimés mais affectés de maladie chronique pulmonaire peuvent être colonisés par P. jirovecii. Il a été suggéré que ces groupes peuvent jouer un rôle dans la transmission interhumaine en faisant partie du réservoir et en pouvant transmettre l’infection par voie respiratoire aux sujets susceptibles. Par ailleurs, l’ADN de P. jirovecii a été identifié dans le poumon de 35 % des fœtus et dans 5 % des placentas de mères non immunocompromises développant des fausses couches, ce qui montre l’existence d’une transmission transplacentaire de Pneumocystis chez l’homme. Ainsi, la transmission verticale de P. jirovecii pourrait représenter une voie additionnelle de transmission pour ce microorganisme sténoxène ; elle assurerait sa persistance indépendamment des conditions environnementales. Des nouvelles recherches sont nécessaires pour confirmer cette voie de transmission et clarifier son rôle dans l’épidémiologie de l’infection humaine par Pneumocystis. # 2009 Elsevier Masson SAS. Tous droits réservés. Introduction presence of P. jirovecii in patients with underlying chronic diseases such as chronic obstructive pulmonary disease has been suggested to be a comorbidity factor [7,28]. The strategies used by these organisms to grow and survive in the context of an intact or debilitated host defenses are largely unknown and limited progress has been made in understanding its life cycle due in large part to the absence of a continuous in vitro culture system. Many questions about P. jirovecii epidemiology and transmission remain unanswered. Until now, human is the only known reservoir host for P. jirovecii and groups at risk for carriage probably represent a major species-specific reservoir of infection, which would allow P. jirovecii propagation [29]. Organisms that are known today as Pneumocystis carinii (P. carinii) were thought to be life cycle stages of American trypanosomes in 1909, but 3 years later were identified as a different genus and species altogether. During the next two decades, these organisms remained in the realm of medical curiosities until they were linked to epidemics of plasmacellular interstitial pneumonia that plagued institutionalized premature and malnourished infants in Europe around World War II [8,10]. For many years, the entity named ‘‘P. carinii’’ was considered like a unique pulmonary pathogen able to cause pneumonia in immunosuppresed hosts. Only for the last years, marked genetic divergence was documented among the Pneumocystis strains of different mammals and now it is well-recognized that each form of Pneumocystis possesses unique genetic characteristics and strict host specificity [1]. The explanation for such strict host specificity has not been determined and is largely unprecedented in the fungi. More recently, the form that infects humans has been renamed Pneumocystis jirovecii (P. jirovecii) and P. carinii is now the name used to describe specifically the organism that infects rats [38,41]. The dramatic increase in the incidence of Pneumocystis Pneumonia (PcP) with the emergence of Human immunodeficiency virus (HIV) pandemia made Pneumocytosis a major medical and public health problem in the 1980s. During the 1990s, advances in the treatment of HIV reduced the frequency of PcP. Although at the beginning of the 21st century, the incidence of frank pneumonia caused by these organisms has decreased in developed countries, the prevalence of AIDSrelated PcP in developing countries remains high and poorly controlled. Likewise, the number of patients who have an altered immune system or who are receiving chronic immunosuppressive medications and are thus at a risk for PcP is rapidly growing [16,27]. But at the beginning of the third millennium, the interest in Pneumocystis infection goes beyond PcP because a new spectrum of disease seems to emerge in immunocompetent hosts and mounting evidence points to new niches being exploited by these fungi. The Detection methods As P. jirovecii cannot be grown in culture from clinical specimens, laboratory diagnosis of PcP has relied mainly upon microscopic visualization with conventional cytochemical or immunofluorescence staining of organisms in respiratory samples. These methods are useful when the organism burden is relatively high but they are insufficient for reliable detection when there is a small parasite load [18]. Although some investigators have detected Pneumocystis carriage by using traditional staining methods, these methods are generally not adequate for detection of Pneumocystis colonization, and researchers have turned to more sensitive molecular techniques [6,39]. Pneumocystis were first detected without the need to visualize the organisms through microscopic examination by the application of polymerase chain reaction (PCR) methods [51]. Nested PCR protocols soon supplanted standard singlecycle amplification owing to their increased sensitivity. More recently, real-time PCR has allowed levels of detection similar to the nested procedures, but is advantageous as it is performed in a one-step process [2,16]. Several straintyping methods of amplified PCR products have allowed insight into epidemiology and transmission of P. jirovecii [4]. These sensitive techniques have enable detection of very low levels of P. jirovecii, not detectable by conventional histochemical 272 E.J. Calderón staining, in respiratory samples from individuals in whom it was not expected. It is thought that detection of P. jirovecii or its DNA in respiratory samples from individuals without signs or symptoms of pneumonia represents colonization with the organism, and accumulating evidence suggests that these groups of subjects may be important in the person to person transmission of P. jirovecii. Furthermore, they may be a major reservoir for future Pneumocystis infection in other susceptible individuals [29,33]. Pneumocystis colonization in adult human HIV-positive individuals are the most studied population of Pneumocystis colonization, although estimates of the colonization rate vary considerably between reports from 10 to 68.8% (Table 1) [11,14,19,21,26,34,50]. The initial observations of a carrier state were obtained when PCR-based assays were evaluated for the diagnosis of PcP in HIV-positive patients. As there was an absence of a fulminant infection, but the presence of P. jirovecii was shown by PCR-based analyses, multiple laboratories independently arrived at the conclusion that this large population might serve as carriers [33]. In an interesting study, the length of carriage following an episode of AIDS-related PcP ranged from 2 week to 16 months. Importantly, two individuals were noted to have a change in genotype, which suggests that exogenous reexposure, as opposed to latent infection, is the source of these organisms [50]. In a group of patients evaluated for PcP at San Francisco General Hospital, 68.8% of patients without PcP were colonized with P. jirovecii. No statistically significant differences were noted in demographic factors, CD4+ T cells, HIV RNA level, history of PcP, or use of PcP prophylaxis between carriers and non-carriers [14]. In a multicenter AIDS cohort study, colonization was detected in 46% of autopsy specimens and only smoking was associated with an increased risk of Pneumocystis colonization [26]. Pneumocystis colonization also occurs in non-HIV immunosuppressed patients [39]. Many non-HIV-positive people with impaired immunity, such as organ transplant recipients, patients with malignancies or those with connective tissue diseases, can develop PcP [16]. In the same way, these individuals are at risk of Pneumocystis colonization (Table 1) [13,20,25,31]. More subtle changes in immune function, such as those associated with pregnancy or chronic lung diseases (Table 2), have been related with Pneumocystis colonization as well [6,7,36,47,48]. There are some studies that have detected transient Pneumocystis colonization in healthy subjects, as such health care workers in contact with PcP patients [23,44]. There is also a study demonstrated the presence of Pneumocystis DNA among 20% adults that were otherwise healthy, although these data require independent verification [22]. Pneumocystis colonization in children Primary exposure to P. jirovecii is common among infants, as is demonstrated by the increase in anti-Pneumocystis anti- Table 1 Pneumocystis colonization in adults with immunosuppression. Colonisation par Pneumocystis chez des adultes immunodéprimés. Author, year [Reference] Subjects Sample no. Leigh et al., 1993 [19] 70 Rabodonirina et al., 1997 [34] 80 Nevez et al., 1999 [31] 69 Matos et al., 2001 [21] 52 Helweg-Larsen et al., 2002 [13] 20 Huang et al., 2003 [14] 32 Wakefield et al., 2003 [50] Maskell et al., 2003 [20] 16 18 Morris et al., 2004 [26] 91 Davis et al., 2008 [11] 172 Mori et al., 2008 [25] 55 Induced sputum/BAL Diagnostic method PCR Population HIV Infected at different levels of CD4 BAL Nested PCR HIV infected with respiratory symptoms BAL Heminested PCR Various causes of immunosuppression Induced sputum/ Nested PCR HIV infected with Oropharyngeal washes respiratory symptoms BAL, tracheal aspirate, Nested PCR Patients with suspected sputum pneumonia and receiving corticosteroids Induced sputum/BAL Nested PCR HIV infected with respiratory symptoms BAL Nested PCR HIV infected BAL Nested PCR Receiving prednisolone (> 20 mg/day) Autopsy lung Nested PCR HIV-infected men dying of non-PcP Induced sputum/BAL Nested PCR HIV infected with non-Pneumocystis pneumonia Induced sputum/BAL PCR Patients with rheunatoid arthritis receiving methotrexate, prednisolone or tacrolimus BAL: bronchoalveolar lavage; Modified of Morris A, et al. JID 2008;197:10—7 [29]. Colonization (%) 10—40 25 14 28.8 60 68.8 43.8 44 46.2 68 10.9 Epidemiology of Pneumocystis infection in Human 273 Table 2 Pneumocystis colonization in subjects with different chronic pulmonary diseases from same geographical area. Colonisation par Pneumocystis chez des patients porteurs d’affections pulmonaires chroniques. Author, year [Reference] Subjects Sample no. Calderon et al., 1996 [6] 50 Calderon et al., 51 2007 [7] Vidal et al., 2006 [48] 37 Vidal et al., 2006 [48] 16 Respaldiza et al., 88 2005 [36] Diagnostic method Sputum Disease Microscopic demonstration Chronic bronchitis with conventional and immunofluorescence staining Sputum Nested PCR Chronic obstructive pulmonary disease Bronchoalveolar lavage Nested PCR Idiopathic interstitial pneumonias Bronchoalveolar lavage Nested PCR Sarcoidosis Sputum or Oropharyngeal Nested PCR Cystic fibrosis washes body titers during the first few years of life. Among healthy, immunocompetent infants in Chile, the seroconversion rate reached 85% by 20 months of age and Pneumocytis DNA was found in 32% of infants studied [42]. In a study carried out among Spanish children, the overall seroprevalence of antiPneumocystis antibody was 73%. Furthermore, there was evidence of an age related increase in seroprevalence, from 52% at age 6 years to 66% at 10 years and to 80% at age 13 years [35]. These findings suggest the continuous exposition to the pathogen during the first and the second infancy and it is concordant with an airborne transmission. In this sense, the first molecular evidence of P. jirovecii transmission from colonized immunocompetent grandparents to their infant granddaughter has been recently provided [37]. Pneumocystis primary infection has been presumed to be an asymptomatic or mild nonspecific disease, however recent reports indicate that it can present clinically as a self-limiting upper or lower acute respiratory tract infection [17,40,42]. In a study carried out in Santiago de Chile, Pneumocystis DNA was detected by nested PCR in specimens from 45 (51.7%) of 87 infants who died unexpectedly in the community, but only 15% had pneumonia [46]. The significance of these findings is unclear. Some studies have suggested a likely association between primary Pneumocytis infection and sudden infant death syndrome but now, this association is not clear [43,45]. The early age of acquisition of Pneumocystis infection in different mammals, including humans, led scientists to think that vertical transmission could be as an additional route of transmission of Pneumocystis. In humans, transplacental transmission was first suggested by a few reports of PcP in neonates published before the AIDS epidemic [3,32]. A few years ago, a controversial case of vertical transmission of P. jirovecii was reported: an infection in the lungs of a fetus of an HIV-positive mother with PcP [30]. However, the study did not identify the organisms as Pneumocystis, and a subsequent fluorescein-labeled monoclonal antibody test yielded negative results [15]. Therefore, vertical transmission of P. jirovecii in humans has remained controversial. Only recently, the first molecular evidence of P. jirovecii transplacental transmission in humans has been provided [24]. In this study, tissues from human fetuses and placentas from nonimmunodepressed women, who had a miscarriage, were evaluated using the exquisitely sensitive detections method Colonization (%) 10 55 37.8 18.8 28.8 of PCR targeting the mtLSU and DHPS genes. P. jirovecii DNA was identified in 35% of foetal tissues and 5% of placenta samples, showing that transplacental transmission can occur in humans and that it is not a rare event [24]. Conclusions Although still impaired by the lack of a reliable and reproducible continuous in vitro cultivation system, research into the natural history of P. jirovecii has advanced owing to the expansion of molecular-based techniques [33]. Even though early studies described the identification of Pneumocystis DNA from the air surrounding apple orchards and the surface of pond water, no Pneumocystis forms were identified in environmental samples using microscopy, and it is uncertain whether there is an ecological niche for Pneumocystis outside the mammalian hosts [9,12,49]. Animal sources for P. jirovecii can be excluded because the Pneumocystis organisms that infect mammalian species are characterized by strong, close host species specificity [1]. So far, human is the only known reservoir host for P. jirovecii [29]. Highly sensitive PCR-technologies have allowed the detection of low numbers of Pneumocystis organisms in respiratory samples from colonized individuals who do not have PcP. Studies have shown that individuals who have underlying HIV-infection or other cause of immunosuppression and those who are not immunosuppressed but have chronic lung disease may often be colonized by P. jirovecii [29]. These groups at risk for carriage probably represent a major species-specific reservoir of infection, although transient Pneumocystis colonization has been also identified in healthy subjects that could behave as a sort of dynamic reservoir for future Pneumocystis infection in other susceptible individuals [22,23,44]. Recent demonstration of P. jirovecii transplacental transmission may explain the accumulating evidence that the primary infection is widely acquired very early in the life and support the view that human infants are a major natural reservoir for P. jirovecii, since they can remain colonized as their immune response matures [5,24]. The accumulating evidence suggests that P. jirovecii is a highly infectious organism with low virulence that takes advantage of hosts as temporary reservoirs of infection. 274 Probably, any person may be colonized by Pneumocystis at some stage in his life [10]. P. jirovecii is a highly adapted parasite that most likely circulates by active airborne horizontal and vertical (transplacental or aerial) transmission mechanisms among human populations developing mostly mild, though frequent, parasitism in the host lungs [1,12]. The length of carriage and the possible detrimental effect of colonization in some populations as individuals with chronic lung diseases or infants remains to be defined. There is growing evidence that P. jirovecii colonization is an important part of the organism’s life cycle and could have significant clinical consequences. Further investigation is needed to throw light on the role of Pneumocystis colonization in development and transmission of PcP and in other human diseases. Acknowledgments I am indebted to Dr. Eduardo Dei-Cas for his assistance during the preparation of the manuscript. This work was developed in the framework of the project ‘‘Pneumocystis Pathogenomics: Unravelling the Colonization-to-Disease Shift’’ into a Coordination Action supported by the European Commission (ERA-NET PathoGenoMics) and the Spanish Ministry of Science and Innovation (FISPI080983). References [1] Aliouat-Denis CM, Chabé M, Demanche C, Aliouat el M, Viscogliosi E, Guillot J, et al. Pneumocystis species, co-evolution and pathogenic power. Infect Genet Evol 2008;8:708—26. [2] Arcenas RC, Uhl JR, Buckwalter SP, Limper AH, Crino D, Roberts GD, et al. A real-time polymerase chain reaction assay for detection of Pneumocystis from bronchoalveolar lavage fluid. Diagn Microbiol Infect Dis 2006;54:169—75. [3] Bazaz GR, Manfredi OL, Howard RG, Claps AA. Pneumocystis carinii pneumonia in three full-term siblings. J Pediatr 1970; 76:767—9. [4] Beard CB, Roux P, Nevez G, Hauser PM, Kovacs JA, Unnasch TR, et al. Strain typing methods and molecular epidemiology of Pneumocystis pneumonia. Emerg Infect Dis 2004;10: 1729—35. [5] Beard CB, Fox MR, Lawrence GG, Guarner J, Hanzlick RL, Huang L, et al. Genetic differences in Pneumocystis isolates recovered from immunocompetent infants and from adults with AIDS: Epidemiological Implications. J Infect Dis 2005;192:1815—8. [6] Calderón EJ, Regordan C, Medrano FJ, Ollero M, Varela JM. Pneumocystis carinii infection in patients with chronic bronchial disease. Lancet 1996;347:977. [7] Calderon EJ, Rivero L, Respaldiza N, Morilla R, Montes-Cano MA, Friaza V, et al. Systemic inflammation in patients with chronic obstructive pulmonary disease who are colonized by Pneumocystis jirovecii. Clin Infec Dis 2007;45:e17—9. [8] Calderon-Sandubete EJ, Varela-Aguilar JM, Medrano-Ortega FJ, Nieto-Guerrero V, Respaldiza-Salas N, de la Horra-Padilla C, et al. Historical perspective on Pneumocystis carinii infection. Protist 2002;153:303—10. [9] Casanova-Cardiel L, Leibowitz MJ. Presence of Pneumocystis carinii DNA in pond water. J Eukaryot Microbiol 1997; 44(Suppl.):28. [10] Cushion MT. Pneumocystis: unraveling the cloak of obscurity. Trends Microbiol 2004;12:243—9. E.J. Calderón [11] Davis JL, Welsh DA, Beard CB, Jones JL, Lawrence GG, Fox MR, et al. Pneumocystis colonisation is common among hospitalised HIV infected patients with non-Pneumocystis pneumonia. Thorax 2008;63:329—34. [12] Dei-Cas E. Pneumocystis infections: the iceberg? Med Mycol 2000;38(Suppl. 1):23—32. [13] Helweg-Larsen J, Jensen JS, Dohn B, Benfield TL, Lundgren B. Detection of Pneumocystis DNA in samples from patients suspected of bacterial pneumonia-a case-control study. BMC Infect Dis 2002;2:28. [14] Huang L, Crothers K, Morris A, Groner G, Fox M, Turner JR, et al. Pneumocystis colonization in HIV-infected patients. J Eukaryot Microbiol 2003;50(Suppl):616—7. [15] Hughes WT. Pneumocystis in infants and children. N Engl J Med 1995;333:320—1. [16] Krajicek BJ, Thomas CF, Limper AH. Pneumocystis pneumonia: current concepts in pathogenesis, diagnosis and treatment. Clin Chest Med 2009;30:265—78. [17] Larsen HH, von Linstow ML, Lundgren B, Høgh B, Westh H, Lundgren JD. Primary pneumocystis infection in infants hospitalized with acute respiratory tract infection. Emerg Infect Dis 2007;13:66—72. [18] Leibovitz E, Pollack H, Moore T, Papellas J, Gallo L, Krasinski K, et al. Comparison of PCR and standard cytological staining for detection of Pneumocystis carinii from respiratory specimens from patients with or at high risk for infection by human immunodeficiency virus. J Clin Microbiol 1995;33:3004—7. [19] Leigh TR, Kangro HO, Gazzard BG, Jeffries DJ, Collins JV. DNA amplification by the polymerase chain reaction to detect subclinical Pneumocystis carinii colonization in HIV-positive and HIV- negative male homosexuals with and without respiratory symptoms. Respir Med 1993;87:525—9. [20] Maskell NA, Waine DJ, Lindley A, Pepperell JC, Wakefield AE, Miller RF, et al. Asymptomatic carriage of Pneumocystis jirovecii in subjects undergoing bronchoscopy: a prospective study. Thorax 2003;58:594—7. [21] Matos O, Costa MC, Lundgren B, Caldeira L, Aguiar P, Antunes F. Effect of oral washes on the diagnosis of Pneumocystis carinii pneumonia with a low parasite burden and on detection of organisms in subclinical infections. Eur J Clin Microbiol Infect Dis 2001;20:573—5. [22] Medrano FJ, Montes-Cano M, Conde M, de la Horra C, Respaldiza N, Gasch A, et al. Pneumocystis jirovecii in general population. Emerg Infect Dis 2005;11:245—50. [23] Miller RF, Ambrose HE, Wakefield AE. Pneumocystis carinii f. sp. hominis DNA in immunocompetent health care workers in contact with patients with P. carinii pneumonia. J Clin Microbiol 2001;39:3877—82. [24] Montes-Cano MA, Chabe M, Fontillon-Alberdi M, de La Horra C, Respaldiza N, Medrano FJ, et al. Vertical transmission of Pneumocystis jirovecii in humans. Emerg Infect Dis 2009; 15:125—7. [25] Mori S, Cho I, Ichiyasu H, Sugimoto M. Asymptomatic carriage of Pneumocystis jirovecii in elderly patients with rheumatoid arthritis in Japan: a possible association between colonization and development of Pneumocystis jirovecii pneumonia during low-dose MTX therapy. Mod Rheumatol 2008;18:240—6. [26] Morris A, Kingsley LA, Groner G, Lebedeva IP, Beard CB, Norris KA. Prevalence and clinical predictors of Pneumocystis colonization among HIV-infected men. AIDS 2004;18:793—8. [27] Morris A, Lundgren JD, Masur H, Walzer PD, Hanson DL, et al. Current epidemiology of Pneumocystis Pneumonia. Emerg Infect Dis 2004;10:1713—20. [28] Morris A, Sciurba FC, Norris KA. Pneumocystis: a novel pathogen in chronic obstructive pulmonary disease? COPD 2008;5:43—51. [29] Morris A, Wei K, Afshar K, Huang L. Epidemiology and clinical significance of Pneumocystis colonization. J Infect Dis 2008; 197:10—7. Epidemiology of Pneumocystis infection in Human [30] Mortier E, Pouchot J, Bossi P, Molinie V. Maternal-fetal transmission of Pneumocystis carinii in human immunodeficiency virus infection. N Engl J Med 1995;332:825. [31] Nevez G, Raccurt C, Vincent P, Jounieaux V, Dei-Cas E. Pulmonary colonization with Pneumocystis carinii in human immunodeficiency virus-negative patients: assessing risk with blood CD4+ T cell counts. Clin Infect Dis 1999;29:1331—2. [32] Pavlica F. The first observation of congenital pneumocystic pneumonia in a fully developed stillborn child. Ann Paediatr 1962;198:177—84. [33] Peterson JC, Cushion MT. Pneumocystis: not just pneumonia. Curr Opin Microbiol 2005;8:393—8. [34] Rabodonirina M, Raffenot D, Cotte L, Boibieux A, Mayençon M, Bayle G, et al. Rapid detection of Pneumocystis carinii in bronchoalveolar lavage specimens from human immunodeficiency virus-infected patients: use of a simple DNA extraction procedure and nested PCR. J Clin Microbiol 1997;35:2748—51. [35] Respaldiza N, Medrano FJ, Medrano AC, Varela JM, de la Horra C, Montes-Cano M, et al. High seroprevalence of Pneumocystis infection in Spanish children. Clin Microbiol Infect 2004;10: 1029—31. [36] Respaldiza N, Montes-Cano MA, Dapena FJ, de la Horra C, Mateos I, Medrano FJ, et al. Prevalence of colonisation and genotypic characterisation of Pneumocystis jirovecii among cystic fibrosis patients in Spain. Clin Microbiol Infect 2005;11:1012—5. [37] Rivero L, de la Horra C, Montes-Cano MA, Rodríguez-Herrera A, Respaldiza N, Friaza V, et al. Pneumocystis jirovecii transmission from immunocompetent carriers to infant. Emerg Infect Dis 2008;14:1116—8. [38] Stringer JR, Beard CB, Miller RF, Wakefield AE. A new name (Pneumocystis jirovecii) for Pneumocystis from humans. Emerg Infect Dis 2002;8:891—6. [39] Takahashi T, Goto M, Endo T, Nakamura T, Yusa N, Sato N, et al. Pneumocystis carinii carriage in immunocompromised patients with and without human immunodeficiency virus infection. J Med Microbiol 2002;51:611—4. [40] Totet A, Respaldiza N, Pautard JC, Raccurt C, Nevez G. Pneumocystis jiroveci genotypes and primary infection. Clin Infect Dis 2003;36:1340—2. 275 [41] Varela Aguilar JM, Medrano Ortega FJ, Calderón Sandubete E. Pneumocystis jirovecii: un nuevo nombre para un viejo patógeno. Rev Clin Esp 2006;206:278—80. [42] Vargas SL, Hughes WT, Santolaya ME, Ulloa AV, Ponce CA, Cabrera CE, et al. Search for primary infection by Pneumocystis carinii in a cohort of normal, healthy infants. Clin Infect Dis 2001;32:855—61. [43] Vargas SL, Ponce CA, Gálvez P, Ibarra C, Haas EA, Chadwick AE, et al. Pneumocystis is not a direct cause of sudden infant death syndrome. Pediatr Infect Dis J 2007;26:81—3. [44] Vargas SL, Ponce CA, Gigliotti F, Ulloa AV, Prieto S, Muñoz MP, et al. Transmission of Pneumocystis carinii DNA from a patient with P. carinii pneumonia to immunocompetent contact health care workers. J Clin Microbiol 2000;38:1536—8. [45] Vargas SL, Ponce CA, Hughes WT, Wakefield AE, Weitz JC, Donoso S, et al. Association of primary Pneumocystis carinii infection and sudden infant death syndrome. Clin Infect Dis 1999;29:1489—93. [46] Vargas SL, Ponce CA, Luchsinger V, Silva C, Gallo M, López R, et al. Detection of Pneumocystis carinii f. sp. hominis and viruses in presumably immunocompetent infants who died in the hospital or in the community. J Infect Dis 2005;191:122—6. [47] Vargas SL, Ponce CA, Sanchez CA, Ulloa AV, Bustamante R, Juarez G. Pregnancy and asymptomatic carriage of Pneumocystis jirovecii. Emerg Infect Dis 2003;9:605—6. [48] Vidal S, de la Horra C, Martín J, Montes-Cano MA, Rodríguez E, Respaldiza N, et al. Pneumocystis jirovecii colonisation in patients with interstitial lung disease. Clin Microbiol Infect 2006;12:231—5. [49] Wakefield AE. DNA sequences identical to Pneumocystis carinii f. sp. Carinii and Pneumocystis carinii f. sp. hominis in samples of air spora. J Clin Microbiol 1996;34:1754—9. [50] Wakefield AE, Lindley AR, Ambrose HE, Denis CM, Miller RF. Limited asymptomatic carriage of Pneumocystis jirovecii in human immunodeficiency virus-infected patients. J Infect Dis 2003;187:901—8. [51] Wakefield AE, Pixley FJ, Banerji S, Sinclair K, Miller RF, Moxon ER, et al. Detection of Pneumocystis carinii with DNA amplification. Lancet 1990;336:451—3.