Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
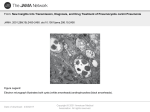
Pneumocystis Jiroveci: Imaging Findings on HRCT
Poster No.:
C-2491
Congress:
ECR 2015
Type:
Educational Exhibit
Authors:
R. E. Correa Soto , J. M. Fernandez Garcia-Hierro , M. J. Martín
1
1
2
1
1
Sánchez , H. Y. saenz , A. Costales Sanchez , D. Palominos
3 1
2
Pose ; SALAMANCA/ES, Carbajosa de la Sagrada/ES,
3
Barcelona/ES
Keywords:
Thorax, Lung, Respiratory system, CT-High Resolution, Education,
Image compression, Infection
DOI:
10.1594/ecr2015/C-2491
Any information contained in this pdf file is automatically generated from digital material
submitted to EPOS by third parties in the form of scientific presentations. References
to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in
any way constitute or imply ECR's endorsement, sponsorship or recommendation of the
third party, information, product or service. ECR is not responsible for the content of
these pages and does not make any representations regarding the content or accuracy
of material in this file.
As per copyright regulations, any unauthorised use of the material or parts thereof as
well as commercial reproduction or multiple distribution by any traditional or electronically
based reproduction/publication method ist strictly prohibited.
You agree to defend, indemnify, and hold ECR harmless from and against any and all
claims, damages, costs, and expenses, including attorneys' fees, arising from or related
to your use of these pages.
Please note: Links to movies, ppt slideshows and any other multimedia files are not
available in the pdf version of presentations.
www.myESR.org
Page 1 of 16
Learning objectives
•
Explain the pathophysiology and clinical manifestations of Pneumocystis
Jiroveci pneumonia (PCP).
•
Describe the radiographic findings of PCP on HRCT.
•
Review the differential diagnosis with other entities that show similar
findings.
Background
Epidemiology:
Pneumocystis jirovecii, previously known as P. Carinii, is a yeast-like fungus of the
genus Pneumocystis. It is the causative organism of Pneumocystis pneumonia, entity
that persists as one of the most prevalent opportunistic infections in immunocompromised
patients. The organism can be found in normal lungs and it is airborne transmitted.
Even with highly active antiretroviral therapy (HAART), PCP remains the most prevalent
opportunistic infection in AIDS.
3
HIV-infected patients with a low CD4 count (<200 cells /mm ) are at the highest risk
of PCP. Others at substantial risk include transplant recipients, patients with cancer
and those under chemotherapy, radiotherapy, glucocorticoids or immunosuppressive
treatments. Recently it has also been reported PCP infections in patients with moderate
immunocompromise, such as those with chronic lung disease. The incidence of PCP is
increasing as the number of people receiving immunosuppressive medications continues
to grow.
Clinical manifestations:
The most common symptoms include progressive dyspnea, nonproductive cough and
low fever. Often it is subacute, gradually worsening over 2-6 weeks. Acute dyspnea with
chest pain may indicate a pneumothorax, entity that must be discarded due to its potential
gravity. It must be considered that PCP in non-HIV patients produces a much more severe
inflammatory response manifested as a fulminant respiratory failure with fever and cough.
Also PCP in non-HIV patients is more difficult to diagnose.
Physical examination shows tachypnea, tachycardia and a normal auscultation but
sometimes it is anodyne.
Page 2 of 16
Diagnosis:
White blood cell count usually not elevated and 90% have elevated LDH. HRCT is the
imaging modality of choice for its study. For the definite diagnosis the procedure of choice
is bronchoscopy with bronchoalveolar lavage (BAL), which has a sensitivity of 90-98%.
Treatment:
Appropriately treated PCP has very good prognosis. Trimethoprim-sulfamethoxazole or
intravenous (IV) pentamidine is effective in most cases with clinical improvement in 80%
of cases (mean: 5 days) after initiation of treatment. One must consider that radiographic
improvement lags by 5 days. In patients with PCP & severe hypoxia, early adjunctive
treatment with corticosteroids has significantly decreased rate of respiratory failure.
Top Differential Diagnoses:
•
•
•
•
•
Hypersensitivitypneumonitis
Lymphocytic interstitial pneumonia
Diffuse alveolar hemorrhage
Cytomegalovirus pneumonia
Pulmonary alveolar proteinosis
Findings and procedure details
We reviewed microbiologically confirmed PCP affected patients diagnosed in our hospital
between July 2009 to July 2014.
The most common HRCT findings were the presence of bilateral ground-glass opacities
distributed in a diffuse/patchy pattern predominantly in central and perihilar areas
with sparing of peripheral subpleural lung. PCP may also present with upper lobes
predominance, as thick or thin-walled cysts and as pneumothorax secondary to cyst
rupture.
Page 3 of 16
Best diagnostic clue: Diffuse symmetric ground-glass opacities in hypoxic
immunocompromised patient.
Location:
•
•
Diffuse perihilar involvement with sparing of peripheral subpleural lung
Less commonly upper lobe predominant disease with thin-walled cysts
Morphology: Ground-glass opacities with cysts (30%).
HRCT FINDINGS
Morphology
Ground-glass opacity is dominant finding
•
Superimposed intralobular lines & smooth interlobular septal thickening
("crazy-paving" pattern) less common
Cysts (30%)
•
•
•
•
•
Thin walled, usually with ground-glass opacities.
Typical upper lobe distribution.
Predisposition to pneumothorax.
Resolution over 5 months with successful treatment.
Rarely described in non-AIDS PCP.
Atypical patterns (5-10%)
•
•
•
Multiple small nodules (may cavitate).
Asymmetric ground-glass or consolidation.
Reticular (interlobular & intralobular) opacities rarely dominant finding.
Distribution
HIV(+)
•
•
•
Diffuse symmetric ground-glass opacities.
Sparing of lung periphery (40%).
Mosaic attenuation (30%).
Page 4 of 16
•
Upper lobe distribution may be associated with aerosolized pentamidine
prophylaxis.
Non-HIV
•
Often spares 1 lung zone (upper, middle, lower).
Prior irradiated lung protected: PCP develops only outside radiation ports
Other
Lymphadenopathy uncommon (10%), short axis diameter > 1 cm.
•
More common with other fungal or tuberculous infections.
Pleural effusion rare.
Confident diagnosis in 95% of patients with AIDS.
Images for this section:
Page 5 of 16
Fig. 1: Coronal HRCT of a patient with Pneumocystis Jiroveci pneumonia shows the
presence of bilateral ground-glass opacities, with diffuse and central distribution. Irregular
cavities chambered thick-walled.
Page 6 of 16
Fig. 2: Axial HRCT of a patient with Pneumocystis Jiroveci pneumonia shows the
presence of bilateral ground-glass opacities, with diffuse distribution. Thin-walled cysts.
Page 7 of 16
Fig. 3: Coronal HRCT of a patient with Pneumocystis Jiroveci pneumonia shows
the presence of bilateral ground-glass opacities, with diffuse, central and upper lobes
distribution.
Page 8 of 16
Fig. 4: Axial HRCT of a patient with Pneumocystis Jiroveci pneumonia shows the
presence of bilateral ground-glass opacities, with diffuse distribution.
Page 9 of 16
Fig. 5: Axial HRCT of a patient with Pneumocystis Jiroveci pneumonia shows the
presence of bilateral groundglass opacities, with diffuse distribution. Thinwalled cysts.
Page 10 of 16
Page 11 of 16
Fig. 6: Coronal HRCT of a patient with Pneumocystis Jiroveci pneumonia shows
the presence of bilateral groundglass opacities, with diffuse, central and upper lobes
distribution.
Page 12 of 16
Fig. 7: Sagittal HRCT of a patient with Pneumocystis Jiroveci pneumonia shows the
presence of groundglass opacities, with diffuse distribution. Thinwalled cysts.
Page 13 of 16
Page 14 of 16
Fig. 8: Sagittal HRCT of a patient with Pneumocystis Jiroveci pneumonia shows the
presence of groundglass opacities, with diffuse distribution.
Page 15 of 16
Conclusion
•
PCP remains the most common opportunistic infection in
immunocompromised patients and its diagnosis requires a high clinical
suspicion.
•
It must be considered in those patients with hypoxia, diffuse bilateral groundglass opacities distributed in a diffuse/patchy pattern located predominantly
in central and perihilar areas.
Personal information
References
•
•
•
•
•
Sepkowitz KA et al: Opportunistic infections in patients with and without
Acquired Immunodeficiency Syndrome. Clin Infect Dis. April 15;34(8)
2002;34(8):1098-107.
Hardak E et al: Radiological features of Pneumocystis jirovecii Pneumonia in
immunocompromised patients with and without AIDS. Lung. 188(2):159-63,
2010.
Tasaka S et al: Comparison of clinical and radiological features of
pneumocystis pneumonia between malignancy cases and acquired
immunodeficiency syndrome cases: a multicenter study. Intern Med.
49(4):273-81, 2010.
D'Avignon LC et al: Pneumocystis pneumonia. Semin Respir Crit Care Med.
29(2):132-40, 2008.
Kuhlman JE: Pneumocystic infections: the radiologist's perspective.
Radiology. 198(3):623-35, 1996.
Page 16 of 16