Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
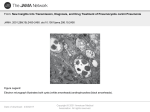
82 Central Nervous System Pneumocystosis in a Patient with AIDS John A. Bartlett and Christine Hulette From the Department of Medicine and the Department of Pathology, Duke University Medical Center, Durham, North Carolina Extrapulmonary involvement with Pneumocystis carinii has been described in 0.5% – 2.5% of persons with AIDS. One hundred nine patients with AIDS and confirmed extrapulmonary pneumocystosis were identified, and seven of these patients (including our patient) had central nervous system (CNS) pneumocystosis. Of these seven patients, six had prior AIDS-related complications, and three had previous P. carinii pneumonia. Six patients had CNS symptoms, one of whom underwent a focal neurological examination. No cases were diagnosed before death. The involved sites were the cerebral cortex (2 patients), meninges (2), pituitary gland (1), putamen (1), and nonspecified locations (3). In two patients, organisms were seen around blood vessels, and in five patients there was concurrent neuropathology. In summary, CNS involvement with P. carinii usually occurs as a late complication of AIDS and probably represents hematogenous dissemination. Infection with Pneumocystis carinii remains a common complication in patients with AIDS. P. carinii pneumonia (PCP) continues to be the initial AIDS-related manifestation in 25% of patients and occurs in ú50% of patients before they die [1]. P. carinii infections may extend beyond the lungs, and extrapulmonary pneumocystosis has been described in 0.5% – 2.5% of persons with AIDS [2, 3]. We recently cared for a woman with AIDS in whom clinically unsuspected CNS pneumocystosis was discovered at autopsy. We report her case and review the literature on extrapulmonary pneumocystosis with an emphasis on CNS involvement. Case Report In March 1991, a 41-year-old woman was admitted to Duke University Medical Center (Durham, NC) because of profound headache and cough. Culture of her CSF yielded Cryptococcus neoformans, and she was then discovered to be HIV-seropositive (initial absolute CD4/ lymphocyte count, 51/mm3). An MRI revealed an increased signal in the region of her left basal ganglia and in her white matter, which was believed to be due to HIV encephalitis or cryptococcal infection. She was treated with amphotericin B and flucytosine followed by oral fluconazole; she also received trimethoprimsulfamethoxazole (TMP-SMZ) as prophylaxis for PCP. She soon developed a diffuse erythematous rash that resolved after discontinuation of TMP-SMZ therapy; she began monthly treatment with aerosolized pentamidine (300 mg). In May 1992, following introduction of contrast medium, a CT scan of the head showed a new area of hypodensity without enhancement Received 7 December 1995; revised 15 January 1997. Reprints or correspondence: Dr. John A. Bartlett, Box 3238, Duke University Medical Center, Durham, North Carolina 27710. Clinical Infectious Diseases 1997;25:82–5 q 1997 by The University of Chicago. All rights reserved. 1058–4838/97/2501–0011$03.00 / 9c33$$jy49 06-10-97 09:50:19 in the left caudate nucleus and anterior limb of the internal capsule, which was believed to be compatible with encephalomalacia due to her past inflammatory process or ischemic changes. In July 1992, she was admitted to our center because of proven PCP, and therapy with TMP-SMZ was started again. She developed a recurrent rash and then received a 3-week course of treatment with dapsone and trimethoprim. She resumed monthly therapy with aerosolized pentamidine. In August 1993, she developed disseminated Mycobacterium avium complex infection, and in March 1994, she developed cytomegalovirus retinitis. In April 1994, she complained of cough, and a chest roentgenogram revealed a right-upper-lobe infiltrate. She was treated empirically for recurrent PCP with oral atovaquone for 6 weeks, and her clinical condition improved. During the summer of 1994, her clinical condition deteriorated, and she received palliative care. She died on 23 September 1994, and an autopsy was performed. Autopsy results. The general autopsy revealed severe necrotizing pneumonia with multiple abscesses and extensive vascular invasion by Aspergillus species. There were multiple septic infarcts containing Aspergillus in both kidneys. Examination of the eyes showed cytomegalovirus retinitis bilaterally with retinal degeneration. No Pneumocystis organisms were identified outside of the CNS, despite Grocott-Gomori methenamine – silver nitrate staining of samples from all major organs. The fresh brain weighed 918 g. The meninges over the superior parietal lobe were cloudy. The brain was sectioned in 1cm slices in a coronal fashion. There was a 0.9-cm cystic defect in the anterior limb of the left internal capsule, and no other gross lesions were found. Examination of the cyst showed subacute infarction characterized by a macrophage infiltrate with adjacent severe gliosis and edema. Grocott-Gomori methenamine – silver nitrate staining of the perivascular space of a juxtaposed blood vessel demonstrated Pneumocystis organisms. In the adjacent putamen, areas of vacuolation with a bubbly appearing neuropil that was most pronounced around blood vessels were seen in virtually every cida UC: CID CID 1997;25 (July) CNS Pneumocystosis and AIDS 83 Figure 1. Photomicrograph revealing focal edema and vacuolation ( arrows ) of the neuropil in the basal ganglia of a patient with AIDS and CNS pneumocystosis. Note the small cystlike spaces in the vicinity (hematoxylin-eosin/luxol fast blue stain; original magnification 1 130). section (figure 1). Grocott-Gomori methenamine – silver nitrate staining of the vacuolated space demonstrated many Pneumocystis organisms (figure 2). Pneumocystis organisms were also seen in the meninges and adjacent to an area of acute hemorrhage in the caudate nucleus. Multiple areas of ischemic damage characterized by tissue edema, reactive astrocytosis, and a scanty macrophage infiltrate were associated with perivascular accumulations of Pneumocystis organisms. In addition, pallor of cerebral myelin and severe myelopathy of the posterior white columns (findings consistent with HIV encephalopathy and my- elopathy) were found. Pneumocystis organisms were not seen in the cerebral myelin or the posterior white columns. Literature Review A search of the English-language literature from 1981 to 1995 was performed to identify reports or reviews of cases of histologically confirmed extrapulmonary pneumocystosis. These cases were reviewed for the sites of P. carinii infection, and the cases of patients with CNS pneumocystosis were reviewed in greater detail. Results Figure 2. Photomicrograph of the same area in figure 1 at a higher magnification; characteristic boat-shaped Pneumocystis organisms are demonstrated ( arrow ) (Grocott-Gomori methenamine – silver nitrate stain; original magnification, 1 680). / 9c33$$jy49 06-10-97 09:50:19 One hundred eight cases of extrapulmonary pneumocystosis were reported in the literature. The sites of documented extrapulmonary pneumocystosis included the liver (41% of cases), spleen (34%), lymph nodes (28%), thyroid gland (23%), kidneys (19%), bone marrow (18%), adrenal glands (15%), eyes (11%), and others. Nervous system localization was documented in seven cases (6%), including CNS pneumocystosis in six cases and involvement of ganglia in the sympathetic nervous system in one case. The six patients with CNS involvement [3 – 8] and our patient are described in table 1. Of these seven patients, six had a history of at least one AIDS-related clinical complication, and five had at least two prior AIDS-related clinical complications. Three patients had a history of PCP. Five patients (71%) were receiving aerosolized pentamidine prophylaxis, and two (29%) were not receiving any prophylaxis. cida UC: CID 84 Bartlett and Hulette CID 1997;25 (July) Table 1. Summary of data on CNS pneumocystosis in seven patients. [Reference], age (y)/sex AIDS-related complication(s) Risk behavior [4], 40/M Homosexual KS, cryptococcosis, CMV retinitis, Staphylococcus aureus sepsis, recurrent bacterial respiratory tract infections Four prior episodes of PCP [5], 26/M Transfusion [3], 33/M Homosexual [6], 41/M Homosexual KS, candidal esophagitis, CMV retinitis, MAC infection, three prior episodes of PCP Cryptococcosis [7], 30/M IDU None [8], 32/M Homosexual [PR], 45/F HSP Cryptococcosis, CMV retinitis Cryptococcosis, Mycobacterium kansasii and MAC infections, CMV retinitis, aspergillus pneumonia, two prior episodes of PCP Extra-CNS isolation of Pneumocystis CNS localization of Pneumocystis Concurrent neuropathology Symptoms Clinical course Progressive confusion and withdrawal, severe dyspnea, decreased urinary output Cerebral atrophy by head CT, no aggressive measures, death Lungs, widely disseminated Virchow-Robin spaces, surrounding rare cortical arterioles HIV encephalopathy Dry gangrene of toes, no neurological symptoms Lethargy, substernal chest pain Sudden death Lungs, widely disseminated Not specified None Respiratory insufficiency, DIC, hypotension, death Lungs, widely disseminated Pituitary gland None Headache, nausea, fever, cough Headache, somnolence, disorientation, fever, left-leg paresis Declining mental status, fever Declining mental status, generalized weakness Sudden death None Cryptococcosis Initial improvement then bronchopneumonia, death Progressive respiratory insufficiency, death Progressive clinical deterioration, death Lungs Cerebral cortex and meninges Four abscesses Lungs, widely disseminated None Toxoplasma gondii infection Not specified Cryptococcosis Putamen around blood vessels, meninges over right parietal lobe HIV encephalopathy, meningeal fibrosis NOTE. CMV Å cytomegalovirus; DIC Å disseminated intravascular coagulation; HSP Å heterosexual partner of HIV-infected person; IDU Å injecting drug user; KS Å Kaposi’s sarcoma; MAC Å Mycobacterium avium complex; PR Å present report. Six patients had potential CNS symptoms, including confusion, disorientation, headache, somnolence, and nausea. Three patients had fever. One patient had a left-leg paresis at the time of neurological examination. Two patients underwent CT of the head; it revealed cerebral atrophy in one patient and abnormalities in one 2 years before Pneumocystis was discovered at the corresponding sites. No patients underwent lumbar puncture. CNS pneumocystosis was not suspected in any of the patients before death. At autopsy, five patients (71%) had concurrent PCP, and four (57%) had widely disseminated pneumocystosis. The involved neuroanatomic locations included the cerebral cortex (2 patients), meninges (2), pituitary gland (1), putamen (1), and nonspecified locations (3). In two patients, organisms were seen around blood vessels. In five patients (71%), there was concurrent neuropathology: HIV encephalopathy (2 patients), cryptococcosis (2), toxoplasma abscesses (1), and meningeal fibrosis from treated cryptococcal meningitis (1). Discussion Dissemination of Pneumocystis beyond the lungs may involve local areas such as the chest and distant sites, a pattern / 9c33$$jy49 06-10-97 09:50:19 suggesting both lymphatic and hematogenous spread. Numerous reports have documented the predilection of P. carinii for vascular involvement [2, 5, 8 – 24]. Pneumocystis organisms have been found to cause vasculitis within the vasa vasorum of the aorta and within the lumina of small arterioles. In addition, cocultivation of peripheral blood lymphocytes and PCR amplification of organism-specific nucleic acid have suggested that P. carinii is present in the bloodstream of patients with PCP and disseminated disease [25 – 27]. CNS pneumocystosis has now been described in seven patients. Six patients had a history of previous opportunistic infections, including three with a history of PCP. Potential neurological symptoms were present in six patients, but only one had focal abnormalities at the time of neurological examination. A head CT of one patient revealed cerebral atrophy, and a head CT of our patient showed focal abnormalities 2 years before P. carinii was discovered at the corresponding sites during autopsy. It is possible that our patient had chronic CNS infection with Pneumocystis that was partially controlled but not cured by treatment with dapsone and trimethoprim and with atovaquone. In two patients with CNS pneumocystosis, organisms were identified in perivascular spaces. These observations further support the role of hematogenous dissemination in extrapulmo- cida UC: CID CID 1997;25 (July) CNS Pneumocystosis and AIDS nary pneumocystosis. CNS pneumocytosis was associated with other active neurological infections in five patients and with healed cryptococcal meningitis in one patient. It is possible that these infections may cause alterations in the local vascular architecture and flow, with the subsequent localization of P. carinii in the CNS during the hematogenous phase. Two patients died suddenly, and five patients’ clinical conditions progressively deteriorated before their deaths. CNS pneumocystosis was clinically unsuspected in all patients, and it was discovered only at autopsy. In most patients (four of seven), P. carinii had widely disseminated. The contribution of CNS pneumocystosis to their deaths is uncertain given their comorbid illnesses, and the clinical significance of CNS pneumocystosis remains to be determined. 12. 13. 14. 15. 16. 17. References 1. Hoover DR, Saah AJ, Bacellar H, et al. Clinical manifestations of AIDS in the era of pneumocystis prophylaxis. N Engl J Med 1993; 329: 1922 – 6. 2. Coker RJ, Clark D, Claydon EL, et al. Disseminated Pneumocystis carinii infection in AIDS. J Clin Pathol 1991; 44:820 – 3. 3. Telzak EE, Cote RJ, Gold JWM, Campbell SW, Armstrong D. Extrapulmonary Pneumocystis carinii infections. Rev Infect Dis 1990; 12:380 – 6. 4. Unger PD, Rosenblum M, Krown SE. Disseminated Pneumocystis carinii infection in a patient with acquired immunodeficiency syndrome. Hum Pathol 1988; 19:113 – 6. 5. Davey RT Jr, Margolis D, Kleiner D, Deyton L, Travis W. Digital necrosis and disseminated Pneumocystis carinii infection after aerosolized pentamidine prophylaxis. Ann Intern Med 1989; 111:681 – 2. 6. Northfelt DW, Clement MJ, Safrin S. Extrapulmonary pneumocystosis: clinical features in human immunodeficiency virus infection. Medicine (Baltimore) 1990; 69:392 – 8. 7. Mayayo E, Vidal F, Alvira R, Gonzalez J, Richart C. Cerebral Pneumocystis carinii infection in AIDS [letter]. Lancet 1990; 336:1592. 8. Cohen OJ, Stoeckle MY. Extrapulmonary Pneumocystis carinii infections in the acquired immunodeficiency syndrome. Arch Intern Med 1991; 151:1205 – 14. 9. Afessa B, Green WR, Williams WA, et al. Pneumocystis carinii pneumonia complicated by lymphadenopathy and pneumothorax. Arch Intern Med 1988; 148:2651 – 4. 10. Balachandran I, Jones DB, Humphrey DM. A case of Pneumocystis carinii in pleural fluid with cytologic, histologic and ultrastructural documentation. Acta Cytol 1990; 34:486 – 90. 11. Bargman JM, Wagner C, Cameron R. Renal cortical nephrocalcinosis: a manifestation of extrapulmonary Pneumocystis carinii infection in the / 9c33$$jy49 06-10-97 09:50:19 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 85 acquired immunodeficiency syndrome. Am J Kidney Dis 1991; 17: 712 – 5. Carter TR, Cooper PH, Petri WA Jr, Kim CK, Walzer PD, Guerrant RL. Pneumocystis carinii infection of the small intestine in a patient with acquired immune deficiency syndrome. Am J Clin Pathol 1988; 89: 679 – 83. Scully RE, Mark EJ, McNeely WF, McNeely BU, eds. Case records of the Massachusetts General Hospital: case 9-1989. N Engl J Med 1989; 320:582 – 7. Grimes MM, LaPook JD, Bar MH, Wasserman HS, Dwork A. Disseminated Pneumocystis carinii infection in a patient with acquired immunodeficiency syndrome. Hum Pathol 1987; 18:307 – 8. Liu YC, Tomashefski JF Jr, Tomford JW, Green H. Necrotizing Pneumocystis carinii vasculitis associated with lung necrosis and cavitation in a patient with acquired immunodeficiency syndrome. Arch Pathol Lab Med 1989; 113:494 – 7. Matsuda S, Urata Y, Shiota T, et al. Disseminated infection of Pneumocystis carinii in a patient with the acquired immunodeficiency syndrome. Virchows Arch [A] 1989; 414:523 – 7. Murry CE, Schmidt RA. Tissue invasion by Pneumocystis carinii: a possible cause of cavitary pneumonia and pneumothorax. Hum Pathol 1992; 23:1380 – 7. Radio SJ, Hansen S, Goldsmith J, Linder J. Immunohistochemistry of Pneumocystis carinii infection. Mod Pathol 1990; 3:462 – 9. Ravalli S, Garcia RL, Vincent RA, Shein R. Disseminated Pneumocystis carinii infection in the acquired immunodeficiency syndrome. N Y State J Med 1990; 90:155 – 7. Raviglione MC. Extrapulmonary pneumocystosis: the first 50 cases. Rev Infect Dis 1990; 12:1127 – 38. Sachs JR, Greenfield SM, Sohn M, Turner JL. Disseminated Pneumocystis carinii infection with hepatic involvement in a patient with the acquired immune deficiency syndrome. Am J Gastroenterol 1991; 86:82 – 5. Saldana MJ, Mones JM. Pulmonary pathology in AIDS: atypical Pneumocystis carinii infection and lymphoid interstitial pneumonia. Thorax 1994; 49(suppl):S546 – 55. Travis WD, Pittaluga S, Lipschik GY, et al. Atypical pathologic manifestations of Pneumocystis carinii pneumonia in the acquired immune deficiency syndrome: review of 123 lung biopsies from 76 patients with emphasis on cysts, vascular invasion, vasculitis, and granulomas. Am J Surg Pathol 1990; 14:615 – 25. Witt K, Nielsen TN, Junge J. Dissemination of Pneumocystis carinii in patients with AIDS. Scand J Infect Dis 1991; 23:691 – 5. Atzori C, Lu J-J, Jiang B, et al. Diagnosis of Pneumocystis carinii pneumonia in AIDS patients by using polymerase chain reactions on serum specimens. J Infect Dis 1995; 172:1623 – 6. Contini C, Romani R, Manganaro M, Sorice F, Delia S. Tissue-culture isolation of Pneumocystis carinii from peripheral blood of AIDS patients with PCP [letter]. AIDS 1993; 7:1137 – 8. Lipschik GY, Gill VJ, Lundgren JD, et al. Improved diagnosis of Pneumocystis carinii infection by polymerase chain reaction on induced sputum and blood. Lancet 1992; 340:203 – 6. cida UC: CID