Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
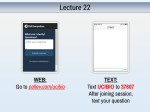
DTD 5 Cancer Detection and Prevention xxx (2004) xxx–xxx www.elsevier.com/locate/cdp Soluble Fas and Fas ligand provide new information on metastasis and response to chemotherapy in SCLC patients Makoto Shimizu MDa, Masashi Kondo MDa, Yasushi Ito MDa, Hiroaki Kume MDa, Ryujiro Suzuki MDa, Kenichi Yamaki MDb,* a Department of Respiratory Medicine, Nagoya University School of Medicine 65, Tsurumai-cho, Showa-ku, Nagoya, Aichi 466-8560, Japan b Kariya Nursing College, Kariya Medical Corporation, 1, 1, 72, Araihata, Hajodo-cho, Kariya, Aichi 448-0804, Japan Accepted 15 September 2004 Abstract Background : The Fas/Fas ligand (FasL) system is a major regulator of apoptosis. Chemotherapeutic drugs have been shown to induce Fas expression on the surface of lung cancer cells, and cancer cell apoptosis. However, this mechanism is not considered to be associated with Fas expressed on lung cancer cells. Soluble Fas and FasL concentrations are reportedly elevated in the peripheral blood of patients with lung cancer, but the roles of circulating soluble Fas and FasL in that disease have not been clarified. Materials and methods : We measured the circulating soluble Fas and FasL levels in 21 patients with small cell lung cancer (SCLC), and 12 healthy matched controls, in order to examine whether such ligands could provide any important information and/or reveal any new clinical features of SCLC. Results : In the CR patients, the neuronal specific enolase (NSE), soluble Fas and soluble FasL concentrations were 21.26 3.65 ng/ml, 3.58 0.19 ng/ml and 0.50 0.15 ng/ml, while in the partial response (PR)/no change (NC)/progressive disease (PD) group of patients they were 33.96 7.86 ng/ml, 5.29 0.29 ng/ml and 0.59 0.07 ng/ml, respectively. The NSE, soluble Fas and soluble FasL concentrations were all elevated in the PR/NC/PD patients, however, significant differences were only seen in Fas concentration between CR and PR/NC/PD patients and CR patients and the controls (p < 0.001). Conclusions : Serum soluble Fas and FasL play important roles in the proliferation and metastasis of SCLC, as well as in the cytotoxic reaction and apoptosis induced by anticancer drugs in SCLC. Further study of the mechanisms and participation of circulating soluble Fas and FasL is necessary to develop treatment strategies for SCLC. # 2004 International Society for Preventive Oncology. Published by Elsevier Ltd. All rights reserved. Keywords: Fas; Fas ligand; SCLC; Chemotherapy 1. Introduction The Fas/Fas ligand (FasL) system is a major regulator of apoptosis. Fas is expressed on the surface of cell membranes in a variety of normal tissue cells and malignant cells including lung cancer cells [1,2], and FasL is expressed on the cell membrane surface of activated T lymphocytes and lung cancer cells [3,4]. Since FasL expressed on T lymphocytes can induce apoptosis in Fas-expressing lung * Corresponding author. Tel.: +81 566 27 5404; fax: +81 566 27 5407. E-mail address: [email protected] (K. Yamaki). cancer cells, the Fas/FasL system plays an important role in the cell-mediated cytotoxic reaction against lung cancer. On the other hand, malignant cells can escape the immune system by the downregulation of the FasL and the killing of lymphocytes through the expression of FasL [5,6]. Thus, the balance of Fas/FasL interaction between the host immune system and malignant cells may play an important role in cancer progression, lymph node involvement, metastasis and cancer cell death. Commonly used chemotherapeutic drugs have been shown to induce Fas expression on lung cancer cells and apoptosis of lung cancer cells [7]. The mechanism of apoptosis induced by drugs has not been clarified, but is 0361-090X/$30.00 # 2004 International Society for Preventive Oncology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.cdp.2004.09.001 DTD 5 2 M. Shimizu et al. / Cancer Detection and Prevention xxx (2004) xxx–xxx not considered to be associated with the Fas expressed on lung cancer cells [8,9]. Unlike membrane-bound Fas and FasL in lung cancer cell lines, the role of soluble Fas and FasL in the proliferation and death of lung cancer cells has yet to be clarified. Soluble Fas and FasL levels rise in the peripheral blood of lung cancer patients, yet the significance of circulating soluble Fas and FasL has not been examined. In the present study, we measured the concentrations of circulating soluble Fas and FasL in patients with small cell lung cancer (SCLC), as they have higher sensitivity to chemotherapeutic agents than non-small cell lung cancer (NSCLC) patients, in order to examine whether soluble Fas and FasL participate in any as yet unidentified clinical features of SCLC. 2. Patients and methods 2.1. Patients Twenty-one patients (15 males, 6 females; mean age, 65.7 years; range, 47–81 years; Table 1) diagnosed with SCLC by transbronchial lung biopsy and treated at the Second Department of Internal Medicine of Nagoya University Hospital from 1998 to 2000 were included in this study. Blood samples were obtained prior to chemotherapy in order to measure soluble Fas and soluble FasL concentrations. All patients were evaluated according to the simple two-stage system developed by the Veteran’s Administration Lung Cancer Study Group [10]. Distant organ metastasis was found in 12 of the 21 patients. Limited disease (LD) stage SCLC describes a tumor confined to the hemithorax of origin, the mediastium, and the supraclavicular lymph node, which can be encompassed within tolerable radiation therapy. Extensive disease (ED) stage SCLC indicates a tumor that is too widespread to be included within the LD stage definition. Blood samples were also obtained from 12 age-matched healthy controls (eight males, four females; mean age, 63.8 years, range, 50–78 years). Blood serum was stored at 80 8C immediately after separation by centrifugation at 4 8C until the assay. 2.2. Therapy and response to therapy The patients in the ED stage received intensive weekly anticancer chemotherapy (vincristine, doxorubicin, etoposide and carboplatin), while patients in the LD stage were treated with the same intensive weekly anticancer chemotherapy as those in the ED stage plus sandwich thoracic irradiation. The response to therapy was documented at 4 weeks following the completion of therapy. Complete response (CR) was defined as the absence of detectable disease, partial response (PR) indicated a reduction in tumor size of more than 50%, no change (NC) indicated a tumor reduction of less than 50% or an enlargement of less than 25%, and progressive disease (PD) indicated a tumor enlargement greater than 25% or additional tumor involvement. Two independent observers evaluated the radiological findings based on X-ray, computed tomography or magnetic resonance imaging films. Prophylactic cranial irradiation was applied only to patients who achieved CR, as proved by negative histology of a transbronchial biopsy after chemotherapy. 2.3. Measurement of soluble Fas and FasL Table 1 Characteristics of the 21 small cell lung cancer patients Patient Age Sex Smoker Stage Distant metastasis Response to chemotherapy 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 58 60 65 71 69 46 51 63 73 68 72 55 64 65 67 69 70 70 71 81 71 M M M F F F M M M M M F F F M M M M M M M Yes Yes Yes Yes Yes No Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes LD LD LD LD LD ED ED LD LD ED ED ED ED ED ED ED ED ED ED LD ED No No No No Yes Yes Yes No No No No Yes Yes Yes Yes Yes Yes Yes Yes No Yes CR CR CR CR CR CR CR PR PR PR PR PR PR PR PR PR PR PR PR PD PD Soluble Fas and FasL in blood serum were measured using a soluble Fas ELISA Kit and soluble FasL ELISA Kit (Medical & Biological Laboratories Co. Ltd., Nagoya, Japan) according to the manufacturer’s instructions. Blood samples (0.1 ml) were poured into antibody-coated microwells using multichannel pipettes, then incubated for 60 min at room temperature. After washing four times, 0.1 ml of peroxidase-conjugated monoclonal antibody solution was added to each well and incubated for 60 min at room temperature with shaking. After washing, the peroxidase substrate reagent (0.1 ml) was added to each well. Stop solution (0.1 ml) was then added to the wells after 30 min shaking at room temperature. The absorbance of each well was measured at a wavelength of 450 nm and the reference at 620 nm using a microplate reader MPQ A4i (Tosoh, Tokyo, Japan). 2.4. Statistical analysis Statistical analysis was performed using Fisher’s PLSD and Scheffe method of Post Hoc Test (StatView 5.0). DTD 5 M. Shimizu et al. / Cancer Detection and Prevention xxx (2004) xxx–xxx Differences with a p-value less than 0.05 were considered significant. Data represent the mean S.E. 3. Results The serum soluble Fas and FasL concentrations of the 21 SCLC patients were 4.72 0.27 ng/ml and 0.56 0.06 ng/ ml (mean S.E.), respectively, and were significantly higher than those of the 12 controls, at 1.98 0.12 ng/ml and 0.27 0.09 ng/ml, respectively (p < 0.001). The neuronal specific enolase (NSE) concentration of the SCLC patients (29.70 25.00 ng/ml) was significantly higher than that of the controls (<10 ng/ml) (p < 0.001) (Table 2). The NSE concentration of the LD and ED patients was 16.19 3.01 ng/ml (n = 8) and 38.05 7.87 ng/ml (n = 13), respectively. The NSE concentration of the ED patients, but not the LD patients, was significantly higher than those of the LD patients and controls. The NSE concentration of patients with distant metastasis (38.02 8.62 ng/ml, n = 12) was significantly higher than that of patients without distant metastasis (8.66 3.37 ng/ ml, n = 9). In SCLC patients without distant metastasis, the NSE concentration was higher than that in the controls, but the difference did not reach statistical significance. Thus, elevation of NSE concentration in serum appears to indicate the spread of SCLC. The soluble Fas concentration of the LD and ED patients was 4.05 0.33 ng/ml (n = 8) and 5.14 0.34 ng/ml (n = 13), respectively. Each was significantly higher than in the controls, and the soluble Fas concentration of ED patients was significantly higher than that of the LD patients, while the soluble Fas concentration of ED patients was the highest of all groups. Therefore, elevation of soluble Fas in blood may indicate progressive proliferation and metastasis of SCLC. The soluble Fas concentration of patients with distant metastasis (5.12 0.39 ng/ml, n = 12) was significantly higher than that of patients without distant metastasis (4.19 0.29 mg/ml, n = 9), and the latter was significantly higher than that of the controls value. Thus, elevation of 3 soluble Fas concentration in serum may indicate a progressive invasion of SCLC, suggesting that soluble Fas may be a valuable marker for SCLC, in addition to NSE, the usual marker of SCLC (Fig. 1). The soluble FasL concentration of the LD and ED patients was 0.44 0.14 ng/ml (n = 8) and 0.64 0.05 ng/ ml (n = 13), respectively, and a significant difference was recognized between the ED patients and controls value but not between LD and ED patients. The soluble FasL concentration of patients with and without distant metastasis were 0.70 0.03 ng/ml (n = 13) and 0.38 0.12 mg/ml (n = 8), respectively. The former was significantly higher than both the latter and that of the controls value, but there was no significant difference between the latter and the controls. The soluble FasL concentration of patients with ED or distant metastasis was higher than in the controls. These data suggest that elevation of soluble FasL concentration in SCLC may indicate an extensive invasion by cancer cells. Elevation of NSE or soluble FasL concentration may indicate the ED stage or distant metastasis of SCLC. In addition, elevation of soluble Fas concentration was detected even in the LD stage and in patients with no distant metastasis of SCLC. These results suggest that serum soluble Fas may be one of the most sensitive markers of SCLC. Complete response was achieved in 7 (33.3%), PR in 12 (57.2%), NC in 0 (0%), and PD in 2 (9.5%) of the 21 SCLC patients. In CR patients, NSE, soluble Fas and soluble FasL concentrations were 21.26 3.65 ng/ml, 3.58 0.19 ng/ml and 0.50 0.15 ng/ml, respectively, while they were 33.96 7.86 ng/ml, 5.29 0.29 ng/ml and 0.59 0.07 ng/ ml, respectively, in the PR/NC/PD group of patients. Elevation of NSE, soluble Fas and soluble FasL concentrations were detected in the PR/NC/PD patients, however, only Fas concentration was significantly different between the CR and PR/NC/PD patients. NSE, soluble Fas and soluble FasL concentrations were elevated in both CR patients and the controls, however only soluble Fas concentration significantly differed between the CR patients and controls. Table 2 Concentrations of soluble Fas, soluble Fas ligand and NSE in the 21 small cell lung cancer patients before chemotherapy Soluble Fas Small cell lung cancer Limited disease Extensive disease Distant metastasis ( ) Distant metastasis (+) CR PR/NC/PD Controls n = 21 n=8 n = 13 n = 10 n = 11 n=7 n = 14 n = 12 Data represent mean S.E. a Significant increase compared with controls (p < 0.001). b Significant increase compared with the former (p < 0.001). a 4.72 0.27 4.05 0.33a 5.14 0.34a,b 4.13 0.27a 5.26 0.40a,b 3.58 0.19a 5.29 0.29a,b 1.98 0.12 Soluble FasL a 0.56 0.06 0.44 0.14 0.64 0.05a 0.42 0.12 0.70 0.03a 0.50 0.15a 0.59 0.07a 0.27 0.09 NSE 29.72 5.44a 16.19 3.01 38.05 7.87a,b 17.53 3.22 40.81 8.92a,b 21.26 3.65 33.96 7.86a <10.00 DTD 5 4 M. Shimizu et al. / Cancer Detection and Prevention xxx (2004) xxx–xxx Fig. 1. Soluble Fas concentration of the ED patients was significantly higher than that of the LD patients and controls (p < 0.001) (a). The soluble Fas concentration of patients with distant metastasis was higher than that of patients without distant metastasis (p < 0.001) (b). In addition, the soluble Fas levels in patients achieving CR were significantly lower than in patients with PR/NC/PD (p < 0.001) (c). Data represent means S.D. Serum elevation of soluble Fas may indicate lymph node involvement and/or distant metastasis of SCLC. 4. Discussion The Fas/FasL system is a major regulator of apoptosis. Fas is expressed on the surface of cell membranes in a variety of normal lung cells and lung cancer cells [1,2], and Fas mRNA is expressed in non-small cell lung cancer cells [11]. Serum soluble Fas is produced from the cell surface of malignant cells in a form lacking the 21 amino acid residues containing the transmembrane domain by alternative splicing. Soluble Fas is supposed to act as a FasL inhibitor to bind Fas and prevent Fas-mediated apoptosis. Circulating soluble Fas has been reported to increase in hepatocellular carcinoma [12], hematopoietic malignancies [13], renal cell carcinoma [14], breast cancer [15] and bladder cancer [16]. We demonstrated in the present study that serum soluble Fas levels are higher in SCLC patients with distant metastasis or in ED patients than in patients without distant metastasis or LD patients. Although the concentrations of serum soluble Fas or FasL did not parallel the levels of Fas or FasL expression on the surface of cancer cells, their expression on lung cancer cell membranes will reflect the circulating soluble Fas and FasL. Thus, measurement of the serum soluble Fas and FasL concentrations is important to understand the tumorigenesis of SCLC. Higher expression of Fas correlates with a lower incidence of lymph node involvement in NSCLC [17]. The expression of Fas on the membrane of cancer cells or mRNA in cancer cells was not determined in the 21 SCLC samples examined in the present study. However, most patients with a higher level of soluble Fas were ED cases and/or distant metastasis cases. Although the highly metastatic potential of lung cancer may not be induced by an alteration in the expression of a single gene, the soluble Fas level may be an important marker of metastasis of SCLC. In addition to Fas, FasL also exists in soluble form released from cell surfaces after cleavage by metalloproteinases [18,19]. FasL is a type II transmembrane protein that is a member of the tumor necrosis factor family of cytokines [20,21], expressed in T-cells, NK cells and a wide variety of tumors, many of which also express Fas [3,4], and induce apoptosis in Fas-expressing cells. High levels of soluble FasL have been observed in some hemopoietic malignancies [22], hepatocellular malignancy [23], colon cancer [24], esophageal cancer [25], and pancreatic cancers [3,4]. The cytotoxic potential of soluble FasL is significantly less than that of membrane-bound FasL. However, soluble FasL retains the capacity to induce apoptosis [26,27]. The soluble Fas and FasL system at the interface of tumor cells and the immune system is more complex than expected. The aberrant expression of FasL is a common feature of malignant cells and can result in tissue invasion, metastatic spread, and immune escape [28]. Invading and metastatic tumor cells typically secrete matrix metalloproteinases and induce matrix metalloproteinase production by surrounding stromal cells that may overwhelm the local tissue capacity to maintain their proteolytic activity in check. Synthetic metalloproteinase inhibitors have been able to prevent tumor cell-induced remodeling of extracellular matrix and DTD 5 M. Shimizu et al. / Cancer Detection and Prevention xxx (2004) xxx–xxx angiogenesis and to provide potentially useful reagents for the control of cancer spread. FasL highly expressed on SCLC cells and circulating soluble Fas may counteract the host’s anticancer immunity in their vicinity thereby enhancing immune escape of cancer cells, cancer cell growth and metastases in patients [5,6]. The expression of FasL is downregulated in highly metastatic subpopulations of NSCLC [29]. We demonstrated that the serum soluble FasL concentration is elevated in SCLC patients, as is soluble Fas, suggesting that soluble FasL plays an important role in tumorigenesis and anticancer cytotoxic activity, similar to soluble Fas. A role for the Fas/FasL signaling system in apoptosis induced by chemotherapy has been proposed for some cell types of lung cancer [30]. The expression of Fas and FasL on the surface of NSCLC cells is upregulated after exposure to anticancer agents, and apoptosis is induced in some cell lines upon exposure to the Fas agonistic monoclonal antibody. However, the drug response to doxorubicin has been demonstrated to be associated with Fas expression in 94 NSCLC cells lines [7], and sensitivity to chemotherapy has not been shown to correlate with Fas-mediated apoptosis [8,9]. Therefore, chemotherapy-induced apoptosis is expected to occur in the absence of Fas and FasL interaction. However, soluble Fas may play a key role in the development of SCLC, and may act as an inhibitor and blocker of the chemotherapy-induced apoptosis of SCLC cells. In the present study, the concentrations of serum soluble Fas were statistically lower in CR patients than in the other patients, although the difference between them was not particularly great. In six of the seven (85.7%) CR patients, the soluble Fas concentration was lower than 4.20 ng/ml, which was the mean minus one S.D. of the soluble Fas concentration of the PR/NC/PD patients, and in only 1 of 14 (7.1%) of the other patients was the soluble Fas concentration lower than 4.20 ng/ml. Therefore, serum soluble Fas may predict the responsiveness to chemotherapy in SCLC patients. However, the concentration at which Fas becomes serum soluble must be determined using a large SCLC patient cohort and the standard assay. Furthermore, the response will be predicted more accurately by a analysis of a combination of soluble Fas and other tumor markers such as NSE and pro GRP. In conclusion, serum soluble Fas and FasL play important roles in the proliferation and metastasis of SCLC, as well as in the cytotoxic reaction and apoptosis induced by anticancer drugs in SCLC. The mechanisms and participation of circulating soluble Fas and FasL require further study in order to develop treatment strategies for SCLC. References [1] Watanabe-Fukunaga R, Brannan CI, Itoh N, et al. The cDNA structure, expression, and chromosomal assignment of the mouse Fas antigen. J Immunol 1992;148:1274–9. 5 [2] Nagata S. Fas and Fas ligand: a death factor and its receptor. Adv Immunol 1994;57:129–44. [3] Ungefroren H, Voss M, Jansen M, et al. Human pancreatic adenocarcinomas express Fas and Fas ligand yet are resistant to Fas mediated apoptosis. Cancer Res 1998;58:1741–9. [4] von Bernstorff W, Spanjaard RA, Chan AK, et al. Pancreatic cancer cells can evade immune surveillance via nonfunctional Fas (APO-1/ CD95) receptors and aberrant expression of functional Fas ligand. Surgery 1999;125:73–84. [5] Bramhall SR. The matrix metalloproteinases and their inhibitors in pancreatic cancer. From molecular science to a clinical application. Int J Pancreatol 1997;21:1–12. [6] Kohn EC, Liotta LA. Molecular insights into cancer invasion: strategies for prevention and intervention. Cancer Res 1995;55: 1856–62. [7] Volm M, Rittgen W. Cellular predictive factors for the drug response of lung cancer. Anticancer Res 2000;20(5B):3449–58. [8] Ferreira CG, Tolis C, Span SW, et al. Drug-induced apoptosis in lung cancer cells is not mediated by the Fas/FasL (CD95/APO1) signaling pathway. Clin Cancer Res 2000;6:203–12. [9] Ferreira CG, Span SW, Peters GJ, Kruyt FA, Giaccone G. Chemotherapy triggers apoptosis in a caspase-8-dependent and mitochondriacontrolled manner in the non-small cell lung cancer cell line NCIH460. Cancer Res 2000;60:7133–41. [10] Zelen M. Keynote address on biostatistics and data retrieval. Cancer Chemother Rep 1973;4:31–42. [11] Boldrini L, Faviana P, Pistolesi F, et al. Alterations of Fas (APO-1/ CD95) gene and its relationship with p53 in non small cell lung cancer. Oncogene 2001;20(45):6632–7. [12] Jodo S, Kobayashi S, Nakajima Y, et al. Elevated serum levels of soluble Fas/APO-1 (CD95) in patients with hepatocellular carcinoma. Clin Exp Immunol 1998;112:166–71. [13] Midis GP, Shen Y, Owen-Schaub LB. Elevated soluble Fas (sFas) levels in nonhematopoietic human malignancy. Cancer Res 1996;56:3870–4. [14] Kimura M, Tomita Y, Imai T, et al. Significance of serum-soluble CD95 (Fas/APO-1) on prognosis in renal cell cancer patients. Br J Cancer 1999;80:1648–51. [15] Ueno T, Toi M, Tominaga T. Circulating soluble Fas concentration in breast cancer patients. Clin Cancer Res 1999;5:3529–33. [16] Mizutani Y, Yoshida O, Bonavida B. Prognostic significance of soluble Fas in the serum of patients with bladder cancer. J Urol 1998;160: 571–6. [17] Volm M, Koomagi R. The implications of proliferation and apoptosis for lung cancer metastasis. Oncol Rep 1996;6:373–736. [18] Suda T, Takahashi T, Golstein P, Nagata S. Molecular cloning and expression of the Fas ligand, a novel member of the tumor necrosis factor family. Cell 1993;75:1169–78. [19] Tanaka M, Suda T, Takahashi T, Nagata S. Expression of the functional soluble form of human ligand in activated lymphocytes. EMBO J 1995;14:1129–35. [20] Smith CA, Farrah T, Goodwin RG. The TNF receptor surperfamily of cellular and viral proteins: activation, costimulation, and cell death. Cell 1994;76:959–62. [21] Takahashi T, Tanaka M, Inazawa J, Abe T, Suda T, Nagata S. Human Fas ligand: gene structure, chromosomal location and species specificity. Int Immunol 1994;6:1567–74. [22] Tanaka M, Suda T, Haze K, et al. Fas ligand in human serum. Nat Med 1996;2:317–22. [23] Strand S, Hofmann WJ, Hug H, et al. Lymphocyte apoptosis induced by CD95 (APO-1/Fas) ligand-expressing tumor cells—a mechanism of immune evasion? Nat Med 1996;2:1361–6. [24] O’Connell J, O’Sullivan GC, Collins JK, Shanahan F. The Fas counterattack: Fas-mediated T cell killing by colon cancer cells expressing Fas ligand. J Exp Med 1996;184:1075–82. [25] Gratas C, Tohma Y, Barnas C, Taniere P, Hainaut P, Ohgaki H. Upregulation of Fas (APO-1/CD95) ligand and down-regulation of Fas DTD 5 6 M. Shimizu et al. / Cancer Detection and Prevention xxx (2004) xxx–xxx expression in human esophageal cancer. Cancer Res 1998;58: 2057–62. [26] Tanaka M, Itai T, Adachi M, Nagata S. Downregulation of Fas ligand by shedding. Nat Med 1998;4:31–6. [27] Schneider P, Holler N, Bodmer JL, et al. Conversion of membranebound Fas (CD95) ligand to its soluble form is associated with downregulation of its proapoptotic activity and loss of liver toxicity. J Exp Med 1998;187:1205–13. [28] Müschen M, Warskulat U, Beckmann WM. Defining CD95 as a tumor suppressor gene. J Mol Biol 2000;78:312–25. [29] Gemma A, Takenaka K, Hosoya Y, et al. Altered expression of several genes in highly metastatic subpopulations of a human pulmonary adenocarcinoma cell line. Eur J Cancer 2001;37:1554–61. [30] Fulda S, Los M, Freisen C, Debatin KM. Chemosensitivity of solid tumor cells in vitro is related to activation of the CD95 system. Int J Cancer 1998;76:105–14.