Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
West Nile fever wikipedia , lookup
Plague (disease) wikipedia , lookup
Chagas disease wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
African trypanosomiasis wikipedia , lookup
United States biological defense program wikipedia , lookup
Yellow fever wikipedia , lookup
Schistosomiasis wikipedia , lookup
Leishmaniasis wikipedia , lookup
Typhoid fever wikipedia , lookup
Orthohantavirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Marburg virus disease wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Yellow fever in Buenos Aires wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Anthrax vaccine adsorbed wikipedia , lookup
Biological warfare wikipedia , lookup
Leptospirosis wikipedia , lookup
History of biological warfare wikipedia , lookup
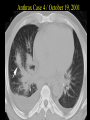
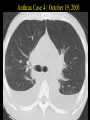
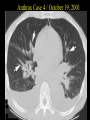
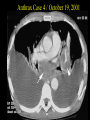
Biological warfare Renaat A. A. M. Peleman, MD, PhD Dept Internal Med, Div Infect Dis University Hospital Ghent Index of Suspicion • Are there an unusual number of patients presenting with similar symptoms? • Is there an unusual presentation of symptoms? • Many cases of unexplained diseases or deaths • Patients presenting with similar set of exposures? • Diseases normally transmitted by vector not present in area • Is this an unexplained case of a previously healthy individual with an apparently infectious disease? • Disease outbreak with zoonotic impact Biological Agents of Highest Concern • • • • • • • Variola major (Smallpox) Bacillus anthracis (Anthrax) Yersinia pestis (Plague) Francisella tularensis (Tularemia) Coxiella burnetii ( Q Fever) Botulinum toxin (Botulism) Filoviruses and Arenaviruses (Viral hemorrhagic fevers) • Report ALL suspected or confirmed illness due to these agents to health authorities immediately Why These Agents? • • • • • Infectious via aerosol Organisms fairly stable in aerosol Susceptible civilian populations High morbidity and mortality Person-to-person transmission (smallpox, plague, VHF) • Difficult to diagnose and/or treat • Previous development for BW Nominal lethality/1,000 kgs of different biological weapens The bioterrorism pathways matrix • Motivation – Number of casualties – Level of panic • Capabilities – Group size – Technical proficiency – Financial resources • Agents – Availability – Ease of growth – Morbidity & mortality • Dissemination – Ease of dissemination – Efficacy of dissemination technique • Target – Number exposed at target – Target vulnerability Covert vs. Overt Event Recognition Response Treatment Responders Overt Covert Early Delayed Early Delayed Early Delayed Traditional First Responders Health Care Workers Diagnostic matrix: chemical and biological casualties Inhalational Anthrax, Plague, Tularemia: Differential Diagnoses • Community acquired pneumonia (CAP) – S. pneumoniae, H. influenzae, Klebsiella spp • Pneumonic Anthrax, Tularemia, Plague, Melioidosis • Brucellosis, Q Fever, Histoplasmosis • Severe atypical CAP (Legionella, Mycoplasma) • Hantavirus pulmonary syndrome (HPS) inhaled BWF bacteria • Treatment – – – – Fluoroquinolones (all) Vibramycin Penicillin Aminoglycosides • Prophylaxis – Fluoroquinolones (all) – Vibramycin Anthrax Disease Complex Summary Inhalational Tracheobronchial Lymphadenitis 1-6 days Hemorrhagic Meningitis 50% Cutaneous ABRUPT ONSET Mediastinitis, cyanosis, stridor, pulmonary edema Papule vesicle edema + eschar 24 - 36 hours GI Toxic shock and Death 20% Resolve Bacteria Bacillus anthracis • • • • Disease: anthrax Incubation: 1 – 60 days Length of illness:1 to 2 days Mortality rate: extremely high, death typically occurs within 24 – 36 hours after onset of severe symptoms • Effective dosage: 8.000-50.000 spores • casualties/50 kg/city/5*106: 250.000 • MMWR-Weekly, November 02, 2001 / 50(43);941-8 • MMWR-Weekly, November 02, 2001 / 50(43);941-8 Chest Radiograph Inhalation Anthrax Note: • widened mediastinum • diminished air space Inhalational anthrax: evolution Anthrax Case 3 / October, 2001 Anthrax Case 3/ October, 2001 Anthrax Case 4 / October 19, 2001 Anthrax Case 4 / October 19, 2001 Anthrax Case 4 / October 19, 2001 Anthrax Case 4 / October 19, 2001 Anthrax Case 4 / October 19, 2001 Specimen Collection: B. anthracis Site Cutaneous Anthrax Specimen Comments Vesicular stage Collect fluid from a previously unopened vesicle with dry sterile Eschar stage Feces Roll swabs beneath the edge of the eschar without removing Provides minimal recovery of agent Nasal swab Useful in later stages of disease. Collect prior to antibiotic use, if possible. Collect only within 24 h of exposure Gastrointestinal Anthrax Blood cultures Inhalation Anthrax Sputum Collect if respiratory symptoms occur and sputum is being produced. Provides minimal recovery of agent. Blood cultures Cultures collected 2-8 days post-exposure may yield the organism. Collect prior to antibiotic use. Cutaneous Anthrax •black eschar (anthracis, Greek for “coal”) • typical red areola Arm Neck Cutaneous anthrax, stemming from wear of infected wool scarf Hemorrhagic Meningitis Human autopsy, 1979, Sverdlovsk, hemorrhagic meningitis 2° to inhalation anthrax Plague Disease Complex Fever/rigors Inhalational Pharyngitis 2 -3 Sudden days onset Fever, URI syndrome APTT ecchymosis DIC Tender bubo 1 - 10 cm 9% 24 hrs Liver enzymes Fulminant Pneumonia 6% late meningitis Erythema Stridor, cyanosis, productive cough, bilateral infiltrates Leukemoid reaction Gram - ve rods in sputum 2 - 10 days Systemic Toxicity Respiratory failure & circulatory collapse Pneumonic Plague: Prevention of Secondary Infection • Secondary transmission is possible and likely Standard, contact, and droplet precautions for at least 48 hrs until sputum cultures are negative or pneumonic plague is excluded Plague: Specimen Collection Site Bubonic Plague Pneumonic Plague Specimen Lymph node aspirate Comments After applying a local anesthetic, obtain specimen by injecting 1 ml of sterile saline into lymph node and aspirating immediately Blood cultures Collect at least three cultures 15 – 20 minutes apart to detect bacteremia Minimal recovery from sputum. Bronchial or tracheal aspirate preferred because of fewer contaminating organisms Sputum, bronchial or tracheal Blood cultures Nasal swab Lymphoid tissue Postmortem Examinations Bone marrow Lung tissue Collect only within 24 h of exposure Clinical clues Anthrax Plague Brucella Incubation 1 – 60 d 2 – 10 d 5–6d Duration of 1 – 2 d illness 1–2d Variabel Major S&S High fever, diff breathing pneumonia & death in 2 – 3 d High T°, tender LN, pneumonia Flu-like, aching joints, myalgia Minor S&S T° & fatigue GI symptoms, GI symptoms skin lesions Specific Gram-neg pneumonia + hemoptysis Widened mediastinum Low WBC and platelets Plague: Differential Diagnosis • Bubonic – Staph/streptococcal adenitis – Glandular tularemia – Cat scratch disease • Septicemic – – – – Other gram-negative sepsis Meningococcemia RMSF TTP • Pneumonic – Bioterrorism threats • Anthrax • Tularemia • Melioidosis – Other pneumonias (CAP, influenza, HPS) – Hemorrhagic leptospirosis Tularemia Disease Complex Summary Inhalational Papule®ulcer Conjunctiva cutaneous lesions Oropharyngeal pseudomembrane 2 - 10 days 50% Secondary pleuropulmonary Abrupt onset Fever, chills headaches 7 - 10 days Primary pulmonary + 2 wks duration Alveolar septa Necrosis & cavitation Rhabdomyolysis Infiltrates, rales Lower nephrotic syndrome Mild liver enzyme Specimen Collection: F. tularensis Specimen Serum for serology Nasal swab Comments Collect an acute phase sample as soon as possible after onset of disease. Collect convalescent phase sample 21-28 days after the acute sample. (1ml min.) Collect only within 24 h of exposure Blood Sputum Collect or induce specimen from symptomatic patients. Bronchial or tracheal wash may produce better yield. Ulcer Collect swab specimen from ulcer on skin or throat Eye Collect swab specimen if eyes affected Q Fever – Clinical Course Summary CNS symptoms and neck stiffness Meningitis Inhalation Osteomyelitis Sudden onset Fever (100 - 104º 3 - 6 days), malaise, anorexia + headache 2 - 14 day course Mild LFT Mild primary atypical pneumonia “ground glass” Late complications Chronic infective endocarditis (aortic valve) Q fever: Clinical Features AT PRESENTATION 3 DAYS LATER Specimen Collection: Q. Fever Specimen Serum for serology Comments Collect an acute phase sample as soon as possible after onset of disease. Collect convalescent phase sample 10-14 days after the acute sample. (10 -12 ml, 2.5ml minimum) Clinical clues Tularemia Q-fever Incubation 1 – 10 d 2 – 14 d Duration of illness 1 – 3 wks 2 – 14 d Major S&S T°, headache, Flu-like Minor S&S weightloss Specific irritating cough Elevated LFT Influenza Cough, T°, Catarrh, loss of appetite Weariness Aching limbs Rickettsiae Coxiella burnetti • Symptoms: acute non-differentiated febrile illness with cough, aches, fever, chest pain, pneumonia • Leukocytosis in 30%, elevated LFT • Prophylaxis: – Vaccine available – Chemoprophylaxis:Doxycycline 100 mg bid for at least 7 days but start only 8 – 12 days post exposure. If started too early, prophylaxis prolongs the disease • Treatment: Doxycycline 100 mg bid for 5 - 7 days Smallpox - Clinical Course Summary Exanthema on Macules papules face, arms, hands pustular vesicles Inhalational 8 - 10 days Replication in regional node of airways 12 day incubation 2 - 3 days Flat Smallpox variants Hemorrhagic Smallpox rapid death before typical lesions Viremia Acute malaise, fever, rigors, headache + mental status changes Scabs separate + pt non-infective Smallpox: Clinical Features USAMRICD Smallpox: Clinical Features USAMRICD Smallpox vs. Chickenpox Incubation Prodrome Distribution Progression Scab formation Scab separation Variola Varicella 7-17 days 2- 4 days centrifugal synchronous 10-14 d p rash 14-28 d p rash 14-21 days minimal/none centripetal asynchronous 4-7 d p rash <14 d p rash Smallpox: Medical Management • Strict airborne precautions and contact isolation of patient – Patient infectious until all scabs have separated • Notify public health authorities immediately for suspected case • Identification of contacts within 17 days of the onset of case’s symptoms Specimen Collection: Smallpox Specimen Comments Do not collect or ship any specimens without consultation from MDCH or CDC Vesicles Vesicle fluid may be placed as a drop on a clean microscope slide. Store each slide in a separate slide holder. As an alternative, collect fluid from separate lesions onto separate swabs. Include cellular material from base of lesion. Store at 4°C for for not more than 6 h. For longer periods store at –20 to –70 °C. Scabs Aseptically collect material or scrapings and place into a sterile, leakproof, freezable container. Store at 4°C for not more than 6 h. For longer periods store at –20 to –70°C. Biopsy Place tissue into a sterile, leakproof, freezable container. Store at 4°C for not more than 6 h. For longer periods store at –20 to –70°C. Formalin fixed tissue acceptable for histopathology. Autopsy Specimens Place into sterile, freezable, leakproof container. Store frozen at –20 to –70°C. VEE – Clinical Course Summary ?? Inhalational Mosquito born 1 to 5 day incubation Febrile syndrome lasting 3 days 100- 104º fever chills, headache, photophobia, sore throat 20% Children 4% Adult cases Mild CNS symptoms for 3 days liver enzymes Weakness for 1 - 2 weeks Recovery More severe CNS signs 10 - 37% mortality The VHF RNA Viruses Acute onset febrile illness High fever, myalgia, GI disturbances Ebola Major organ Marburg necrosis Severe systemic illness coagulation abnormalities Lassa Oropharyngeal lesions Machupo Hantaan Renal failure Pulmonary Syndrome Four Corners Agent Severe bleeding ecchymosis Congo fever Jaundice Syndrome Yellow fever Dengue (2x) Rift Valley 7 days Rapid progression into shock and death VHF: Patient Isolation • Single room w/ adjoining anteroom (if available) – Handwashing facility with decontamination solution • Negative air pressure • Strict barrier precautions including protective eyewear/faceshield • Disposable equipment /sharps in rigid containers with disinfectant then autoclave or incinerate • All body fluids disinfected Specimen Collection: Viral hemorrhagic fever Site Specimen Comments Do not collect or ship any specimens without consultation from MDCH or CDC Ebola, Marburg, Argentine, Junin, Bolivian hemorrhagic fevers and Lassa fever Serum Collect 10 – 12 ml of serum Clinical clues: viruses Variola Venezuelan Yellow equine enc fever Incubation Approx 12 d 1–5d 3–6d Duration of illness Major S&S severa1 wks 1 – 2 wks 1 – 2 wks Minor S&S Specific Malaise, T°, Sudden T°, chills, Lesions headache+, after 2-3 d musclepain Nausea, sore throat,diarrea Highly contagious T°, myalgia, prostration. Easy bleeding vasculitis Clinical clues: toxins Botulinum Time to effect 12 – 36 hrs Ricin SEB Few hrs 3 – 12 hrs Duration of illness 24 – 72 hrs 3d Up to 4 wks Major S&S Cranial nerve palsy, desc flaccid paralysis Sudden T°, weakness, cough, APE T°, chills, headache, nausea, cough Minor S&S Specific Convulsions, liver failure Latent period of 3 – 12 hrs on exposure Specimen Collection: C. boltulinum Specimen Comments Testing must be arranged with MDCH prior to specimen transport (517/335-8063) Serum Collect 10 ml (3-4 ml minimum) of serum as soon as possible after the onset of symptoms and before administration of antitoxin. Feces 15 – 25 g of stool should be collected. Store and ship at 4°C. DO NOT FREEZE. Do not use preservative. Food sample Requires 0.5 cup of food. Food should be left in original container if possible or placed in a sterile unbreakable container. Place containers in leak-proof plastic bags. Store and transport at 4°C. If product was originally frozen, do not thaw, ship frozen. Wound or tissue Place in an anaerobic collection device. Transport at room temperature. Summary: important differentials Conclusions • The zebra card • • • • • • • • • • Unlikely is not unthinkable Be suspicious Protect thyself Assess the patient Decontaminate as appropriate Diagnose Treat Infection control Alert authorities Spread the gospel Acknowledgements - references • USAMRIID’S Medical Management of Biological Casualties Handbook. US Army Medical Research Institute of Infectious Diseases, Maryland. 4th Ed. Febr.2001. • Bioterrorism Readiness Plan: A Template for Healthcare Facilities. APIC Bioterrorism Task Force, CDC Hospital Infections Program Bioterrorism Working Group. 1999 • Textbook of Military Medicine. Office of the Surgeon General Dept Army, USA • Bioterrorism in the US: Threat, Preparedness and Response. Chemical and Biological Arms Control Institute. November 2000. • Clinical Aspects of Critical Biological Agents. Powerpoint presentation sponsored by the Public Health Consortium Michigan • Armed Forces Institute of Pathology and the American Registry of Pathology, Washington DC and INOVA Fairfax Hospital, Fairfax VA. http://anthrax.radpath.org/index.html