Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
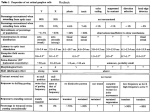
(Acta Anaesth. Belg., 2016, 67, 1-5) Stellate ganglion blockade-techniques and modalities A. Ghai (*), T. Kaushik (*), R. Wadhera (**) and S. Wadhera Abstract : Stellate ganglion block (SGB) is utilized in the diagnosis and management of various vascular disorders and sympathetically mediated pain in upper extremity, head and neck. The stellate ganglion lies medial to the scalene muscles, lateral to longus coli muscle, esophagus, trachea and recurrent laryngeal nerve, anterior to C7 transverse process and prevertebral fascia, superior to the subclavian artery and posterior to vertebral vessels. Consequently, inadvertent placement of the needle tip into these soft tissues and vessels occur with blind technique. Henceforth, various interventional modalities are being used for SGB, these have been reviewed in this paper. Various techniques of SGB have been described, and vary from the use of standard blind technique to the use of fluoroscopy, computerized tomography, magnetic resonance imaging, and radio nucleotide tracers. However, these techniques may not be practical in a clinical setting, insofar as they are time consuming, costly, and may involve radiation exposure. The use of fluoroscopy does not visualize the blood vessels close to the stellate ganglion. Ultrasounds are the alternative. They help in visualization of soft tissues to prevent complications and help in deposition of drug subfascially, under direct visual control. Key words : Stellate ganglion ; Stellate ganglion block ; blind technique ; fluoroscopy ; sonographic guidance. Introduction The stellate ganglion block (SGB) has been used to treat vascular insufficiency, vasospasm, hyper hidrosis, and a variety of pain syndromes, including complex regional pain syndrome, type I and II, phantom limb pain, postherpetic neuralgia, herpes zoster, pain from cen tral nervous system lesions, atypical facial pain, and intractable angina pectoris. First implemented by Leriche and further refined by Findley and Patzer (1), the most common technique is blind paratracheal approach. However, various complications like subarachnoid or epidural injection, recurrent laryngeal nerve palsy, seizures, and blindness have led to the emergence of interventional radiology, including fluoroscopy, computerized tomography (CT scan), magnetic resonance imaging (MRI) and ultrasound guided techniques (2-4). The stellate ganglion is located immediately below the prevertebral fascia covering the longus coli muscle, separated by loose areolar tissue from posterior osseous structures. The vertebral artery is located anterior to the stellate ganglion, usually runs ventrally to the seventh cervical transverse process, and usually enters the foramen transversum of the C6 vertebra (Fig. 1). In 10% of individuals, it enters the foramen transversum at the C5 level or higher, and is more tortuous on the left side. This can lead to vertebral artery injury during SGB. The inferior thyroid artery runs ventrally to C6 and C7, lying anterior to the vertebral artery. The close proximity of stellate ganglion may lead to retropharyngeal hematoma, and accidental intravascular injections, eventually leading to cardiac arrest (5). The preganglionic fibers of the head and neck continue to travel cephalic to the superior and middle cervical ganglion through the cervical sympathetic trunk, which is located anterior to the prevertebral fascia (6). Hence, all sympathetic fibers to the head and neck either synapse at the level of the sympathetic ganglion, or pass through it to the more cephalic ganglion. SGB provides complete blockade of head and neck sympathetic structures (7-10). Approaches and imaging modalities Classic blind approach Technique The patient is placed in the supine position, with head extended. The landmark is the anterior Anju Ghai ; Teshi Kaushik ; Raman Wadhera ; Sarthak Wadhera. (*) Departments of Anesthesia and Critical Care, (**) Dept. of ENT Pt. BD Sharma, PGIMS, Rohtak, Haryana, India. Correspondence address : R. Wadhera, House no. 6/8 FM, Medical campus, PGIMS, Rohtak, Haryana, India. Tel. : 09416974794, 01262- 212860. E-mail : [email protected] © Acta Anæsthesiologica Belgica, 2016, 67, n° 1 ghai-kaushik-.indd 1 18/04/16 14:06 2 a. ghai et al. recurrent laryngeal nerve is also possible (2), as well as esophageal injury (12). Fluoroscopy-guided stellate ganglion block This technique aims at guiding the needle towards the Chassaignac’s tubercle. However, there is a large variability in size and location of it (13). Epidural and intrathecal injections can be ruled out using the spread of contrast in fluoroscopy. The needle can be accurately directed to the landmark, using oblique approach (14). Technique Fig. 1. — Anatomy of stellate ganglion tubercle of C6, which lies against the cricoid cartilage. The sternocleidomastoid muscle is retracted laterally, pulling the internal carotid artery away. The needle is then inserted perpendicularly between the cricoid cartilage and the operator fingers, and passed until contact is made with the C6 tubercle. The needle is withdrawn a few millimeters away from the periosteum of C6 transverse process and, after a negative aspiration test for blood and cerebrospinal fluid (CSF) detection, 1 ml of the local anesthetic solution is injected. Disadvantages The C6 landmark is in close proximity to the middle cervical ganglion instead of the stellate ganglion, and the cervical sympathetic ganglion is primarily blocked when the injected solution spreads to the T1 level (2). The width of the C6 tubercle can be as small as 6 mm, and can be missed during blind needle advancement. A small deviation of the needle may puncture the vertebral artery. If the needle is directed to the posterior tubercle, the drug can spread around the spinal nerve roots. The final position of the needle and the spread of local anesthetic (LA) agents is unpredictable (10, 11). There is also a risk of thyroid gland hematoma. Intravascular injections and vascular injury have been reported despite a negative aspiration test, leading to life threatening complications like retropharyngeal hematoma, cardiac arrest, and convulsions (5). A paralysis of the The patient is positioned in a similar way as for the blind technique. The fluoroscopy beam is directed in anteroposterior direction, with caudo cranial angulations of the C arm. The needle is directed towards the C6 anterior tubercle, and advanced under real time imaging to contact the bony target. The stylet is then removed, and the needle is connected to a three-way extension set to allow a 1-2 ml radio opaque contrast injection. After a negative aspiration test, a test dose of local anesthetic agent is given, followed by the injection of the therapeutic dose. Flow of contrast to the head of first rib can be observed by increasing the amount of contrast injection, which pushes the contrast up and down. A modified fluoroscopy-guided technique is performed with the patient in the supine position, with the neck slightly extended and the head rotated slightly to the opposite side. The skin temperatures are recorded at the distal portion of both upper extremities, in mirror-image locations. The fluoroscopy beam is directed in an anteroposterior direction, until the C5-C6 disc is well visualized. This usually requires caudocranial angulations of the C-arm. The C-arm is then rotated obliquely, on the side of the block. The rotation must occur to allow adequate visualization of the neural foramina. A skin wheal is raised at the surface point of the junction of the uncinate process and the vertebral body, as seen on the fluoroscope. Under real-time imaging, a single pass is made with a 25-gauge spinal needle to contact bone at this point. The stylet is removed, and 2 ml of radioopaque contrast is injected to visualize the longus coli muscle. A 0.5 mL test dose is injected.. This approach provides better upper extremity blockade and less chances of vertebral artery puncture due to oblique rather than perpendicular view (13). © Acta Anæsthesiologica Belgica, 2016, 67, n° 1 ghai-kaushik-.indd 2 18/04/16 14:06 stellate ganglion blockade3 Advantages With this technique, the intravascular injection is prevented by the prior administration of dye, identification of bony anatomy is possible, and the spread of drug is visualized. Disadvantages The anterior tubercle is only a surrogate marker of the location of the stellate ganglion. This location is defined by the fascia plane of the pre-vertebral fascia, which can’t be visualized using fluoroscopy. Soft tissue structures surrounding the stellate ganglion are poorly visualized, including the longus coli muscle, the thyroid gland, and the esophagus, leading to increased risk of injury (15). The precise needle placement into the subfascial plane of the longus coli is not possible (16). The contrast agent may show aberrant and inconsistent spread (16). The fluoroscopic technique helps to avoid inadvertent intravascular injection of local anesthetic agent, but the injection can be identified only after artery is punctured. Therefore, vascular injury is possible (15). CT/ MRI guided block The spread of local anesthetic agent after C6 stellate ganglion block has been defined using computerized axial tomography (CAT) in 10 patients. Radiocontrast and local anesthetic mixture were given in 5 ml increments up to a 20 ml total volume for C6 stellate ganglion nerve blocks in eight patients and C7 in two patients. CAT scanning was performed at baseline and after 5, 10, 15, and 20 ml administration. Cervical level and pattern of spread was recorded after each increment. One half of the injections were beneath the pre-vertebral fascia. Injections on top of the fascia spread more diffusely around C6. All injections of high volume reached the medial aspect of T1 around the head, not neck, of the first rib (16). Advantages Although fluoroscopic guidance has helped reducing the complication rate of stellate ganglion blocks, some complications such as lesions to the lung or pleura may occur, particularly when a C7 approach is performed. Moreover, the accuracy of needle placement allowed by the use of CT guidance, which is highly superior to that of fluoroscopic guidance, explains the low complication rate (1.7%) with that technique (17). Disadvantages The use of MRI and CT can be expensive, time-consuming, and impractical for most pain physicians. Another point to consider is that different blocks in the same patient can produce variable spread and may consequently explain the inconsistent outcomes seen with a “blind” technique (18). Studies using MRI (8) or CT (16) have failed demonstrating any evidence of spread to the stellate ganglion itself, although in the CT study, the stellate ganglion could not actually be visualized. However, an ultrasound imaging study showed spread from C4 to C7 while using 5 ml of local anesthetic mixture. In that study, the authors considered to be an effective clinical stellate ganglion block in 23 out of 24 cases (19). Ultrasound guided stellate ganglion block The success or failure of either blind or fluoroscopic-guided injection depends on the thickness of the longus coli muscle, and on the anatomic location of the cervical sympathetic trunk. The endpoint for injection in the ultrasound-guided technique is the pre-vertebral fascia, and not a contact with bone as with the fluoroscopy and blind techniques. Technique The patient is positioned in the supine or lateral position. A high frequency linear transducer (613 MHz) is placed at the level of C6 or C7 to enable cross sectional visualization of anatomic structures – the transverse process and anterior tubercle of C6, the longus coli muscle, the pre-vertebral fascia covering the muscle, the carotid artery, and the thyroid gland. The transducer is gently pressed between the carotid artery and the trachea, in a para-tracheal approach, to retract the carotid artery laterally and to position the transducer close to the longus coli. A 1.0 inch, 25 G needle is inserted para-tracheally, with the needle staying out-of -plane to the ultrasound beam towards the middle of the longus coli. A pre-scan is important to determine the path of needle insertion, as the esophagus, the inferior thyroid artery, and, in some cases, the vertebral artery may obviate the needle insertion path between the carotid artery and the trachea. In this situation, the needle is inserted lateral to the carotid artery (Fig. 2). When advancing the needle from the lateral © Acta Anæsthesiologica Belgica, 2016, 67, n° 1 ghai-kaushik-.indd 3 18/04/16 14:06 4 a. ghai Fig. 2. — Colour doppler mode used before needling to identify major vessels. [A] Thyroid gland. [B] Carotid artery [C] Internal Jugular vein. [D] Vertebral artery [E] Transverse process of C7. aspect, the best interval is between the carotid artery and the tip of the anterior tubercle, with needle staying in plane of the ultrasound beam. This needle path avoids hitting the cervical nerve root. This pathway is intramuscular, with needle passing through the sternocleidomastoid and anterior scalene muscle. With this approach, the internal jugular vein can be visualized by decreasing the probe pressure. Avoiding jugular vein puncture is obtained by pushing it away with the needle (Fig. 3). The tip of the needle is directed to the pre- vertebral fascia, superficial to the longus coli. A total of 5 ml of local anesthetic mixture is injected. The visualization of the spread under real time scanning is important, insofar as the absence of spread indicates intravascular injection (20). et al. Fig. 3. — Needle path in real time imaging [A] carotid artery [B] Internal jugular vein [C] Needle piercing the fascia covering longus colli. [D] Transverse process of C7 [E] longus colli. blockade to the head and neck as compared to sympathetic blockade at the C7 level (2, 14). This is because of the presence of Kuntz’s nerves. The caudal spread of the solution to the T2 to T3 level is required to block the sympathetic outflow to the upper extremity. Methylene blue dye has been visualized at the stellate ganglion level in only 46% of cases when the C6 level is targeted, while at C7 the dye was seen in 63% of cases (22). Therefore, the C7 level may be more appropriate for upper limb sympathetic blockade. Advantages Conclusion This technique improves the safety of the procedure through the direct visualization of the related soft tissue structures that are not visualized with fluoroscopy. It minimizes the risk of thyroid gland, vessels, including vertebral artery, or esophageal injury (21). A minimal amount of drug is also needed (22). It provides real time needle advancement so that the clinician may visualize the needle entry to the soft tissue target ? and its final placement in the subfascial plane. Ultrasound guidance allows a direct monitoring of the spread of the local anesthetic solution. It results in more caudal spread due to subfascial injection than cephalic spread due to suprafascial injection with fluoroscopy. Studies using MRI or CT have failed to demonstrate any evidence of spread to the stellate ganglion itself, However, the use of ultrasound imaging has shown spread from C4 to C7. The bedside availability of ultrasound, the visualization of soft tissues, and the subfascial drug deposition with realtime imaging place the ultrasound above other imaging modalities. Level of sympathetic blockade Studies have shown that blockade at the C6 level have resulted in more successful sympathetic References 1. Buckley F. P., Morricca G., Murphy T. M., Neurolytic blockade and hypophysectomy. In : Bonica J. J., The management of pain. 2nd ed. Philadelphia : Lea and Febiger, 1990, p. 2012-4. 2. Elias M., Cervical Sympathetic and stellate ganglion bocks, Pain Physician, 3, 294-304, 2000. 3. Hogan Q. H., Erickson S. J., Abram S. E., Computerized tomography (CT) guided Stellate ganglion blockade, Anesthesiology, 83, 424-6, 1992. 4. Slappendel F., Thijssen H., Crul B. J., Merx J. L., The stellate ganglion in magnetic resonance imaging, a © Acta Anæsthesiologica Belgica, 2016, 67, n° 1 ghai-kaushik-.indd 4 18/04/16 14:06 stellate ganglion blockade5 quantification of anatomic varability, Anesthesiology, 83, 424-6, 1995. 5. Higa K., Hirata K., Hirota K., Nithara K., Shono S., Retropharyngeal haematoma after stellate ganglion block, Anesthesiology, 105, 1238-45, 2006. 6. Drake L. D., Vogl W., Michel A. W., Head and Neck. In : Gray’s anatomy for students. New York : Churchill Livingstone, 2005, 933. 7. Raj P. P., Stellate ganglion block. In : Waldman and Wenner, eds. Interventional pain management. Philadelphia : WB Saunders publication, 1996, 269. 8. Hogan Q. H., Erickson S. J., Magnetic resonance imaging of stellate ganglion : Normal appearance, Am. J. Roentgen., 158, 655-9, 1992. 9. Mamquivst E. L., Bengtsson M., Soren J., Efficacy of stellate ganglion block : A clinical study with bupivacaine, Reg. Anesth., 17, 340-7, 1992. 10.Ellis H., Feldman S., Anatomy of Anaesthetists. 3rd ed. Oxford, Blackwell Scientific Publications, 1979, p. 256-62. 11. Feigl G. C., Rosmarin W., Stelzl A., Weninger B., Likar R., Comparison of different injectate volume for stellate ganglion block : an anatomic and radiologic study, Reg. Anesth. Pain Med., 32, 203-8, 2007. 12.Narouze S., Vydyanathan A., Patel N., Ultrasound- guided stellate ganglion block successfully prevented esophageal puncture, Pain Physician, 10, 747-52, 2007. 13.Abdi S., A new and easy way to block stellate ganglion, Pain Physician, 7, 327-31, 2004. 14.Jadon A., Revalidation of a modified and safe approach of stellate ganglion block, Indian J. Anaesthesia, 55, 52-6, 2011. 15.Sibhata Y., Fujiwara Y., Komatsu T., A new approach of ultrasound guided stellate ganglion block, Anesth. Analg., 105, 550-1, 2007. M., Martinez C. R., Computerized axial 16.Christie J. tomography to define the distribution of solution after stellate ganglion nerve block, J. Clin. Anesth., 7 (4), 30611, 1995. 17.Kastler D., Aubry S., Sailley N., Michalakis D., Siliman G., Gory G., Lajoie J. L., Kastler B., CT-guided stellate ganglion blockade vs. radiofrequency neurolysis in the management of refractory type I complex regional pain syndrome of the upper limb, Eur. Radiol., 23, 1316-1322, 2013. 18.Davies R. M., Stellate ganglion block – a new approach, Anaesthesia, 7, 151-153, 1952. 19.Kapral S., Krafft P., Gosch M., et al., Ultrasound imaging for stellate ganglion block : Direct visualization of puncture site and local anesthetic spread, Reg. Anesth., 20, 323328, 1995. 20.Gofeld M., Bhatia A., Abbas S., Ganapathy S., Johnson M., Development and validation of a new technique for ultrasound guided stellate ganglion block, Reg. Anesth. Pain Med., 34, 475-9, 2009. 21.Lee M. H., Kim K. Y., Song J. H., Jung H. J., Lim H. K., Lee D. I, et al., Minimal volume of anaesthetic required for an ultrasound guided stellate ganglion block, Pain Medicine, 13, 1381-8, 2012. 22.Harano K., Difference of spread of injectate solutions after stellate ganglion block to sixth and seventh vertebral levels, Anesthesiolgy, 15, 871-7, 1998. © Acta Anæsthesiologica Belgica, 2016, 67, n° 1 ghai-kaushik-.indd 5 18/04/16 14:06