Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
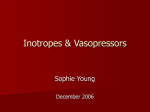
British Journal of Anaesthesia 102 (2): 198–204 (2009) doi:10.1093/bja/aen367 Levosimendan pre-treatment improves outcomes in patients undergoing coronary artery bypass graft surgery† L. Tritapepe1‡, V. De Santis1*, D. Vitale1, F. Guarracino2‡, F. Pellegrini3, P. Pietropaoli1 and M. Singer4‡ 1 Department of Anesthesiology and Intensive Care, ‘Sapienza’ University of Rome, Rome, Italy. Cardiothoracic Department, Cardiothoracic Anesthesia and Intensive Care Unit, University Hospital of Pisa, Pisa, Italy. 3Department of Clinical Pharmacology and Epidemiology, Consorzio Mario Negri Sud, Santa Maria Imbaro, Chieti, Italy. 4Bloomsbury Institute of Intensive Care Medicine, University College London, London, UK 2 *Corresponding author. E-mail: [email protected] Background. The calcium sensitizer levosimendan has anti-ischaemic effects mediated via the opening of sarcolemmal and mitochondrial ATP-sensitive potassium channels. These properties suggest potential application in clinical situations where cardioprotection would be beneficial, such as cardiac surgery. We thus decided to investigate whether pharmacological pre-treatment with levosimendan reduces intensive care unit (ICU) length of stay in patients undergoing elective myocardial revascularization under cardiopulmonary bypass. Methods. One hundred and six patients undergoing elective coronary artery bypass grafting were randomly assigned in a double-blind manner to receive levosimendan or placebo. Levosimendan (24 mg kg21) or placebo was administered as a slow i.v. bolus over a 10 min period before the initiation of bypass. Results. Tracheal intubation time and the length of ICU stay were significantly reduced in the levosimendan group (P,0.01). The number of patients needing inotropic support for .12 h was significantly higher in the control group (18.0% vs 3.8%; P¼0.021). Compared with control patients, levosimendan-treated patients had lower postoperative troponin I concentrations (P,0.0001) and a higher cardiac power index (P,0.0001). Conclusions. Pre-treatment with levosimendan in patients undergoing surgical myocardial revascularization resulted in less myocardial injury, a reduction in tracheal intubation time, less requirement for inotropic support, and a shorter length of ICU stay. Br J Anaesth 2009; 102: 198–204 Keywords: heart, coronary artery bypass; heart, inotropism; heart, ischaemia; surgery, cardiovascular Accepted for publication: November 18, 2008 The myocardium has to endure periods of ischaemia and reperfusion during coronary artery bypass grafting (CABG) surgery. Despite some degree of ischaemic protection afforded by cardioplegia, which establishes electromechanical arrest and reduces myocardial oxygen consumption, myocardial contractile dysfunction is a frequent complication. This often necessitates inotropic and mechanical circulatory support and is associated with an increase in morbidity and mortality.1 2 Levosimendan is a cardiovascular drug licensed for the treatment of acute decompensated heart failure.3 It has positive inotropic4 and anti-stunning effects mediated by calcium sensitization of contractile proteins;5 in addition, it has vasodilatory6 and anti-ischaemic effects mediated by the opening of ATP-sensitive potassium (KATP) channels.7 The KATP channel is an important mediator or end-effector of cardioprotection, thus, levosimendan may offer a beneficial approach in situations of myocardial stress. † Trial registration: clinicaltrials.gov identifier: nCT00610350. Declaration of interest. L.T., F.G., and M.S. have sat on advisory boards for levosimendan on behalf of Orion, the manufacturer, and Abbott, the distributor. They have also received honoraria for chairing/speaking at satellite symposia. ‡ # The Board of Management and Trustees of the British Journal of Anaesthesia 2009. All rights reserved. For Permissions, please e-mail: [email protected] Levosimendan pre-treatment in patients undergoing CABG In clinical studies to date, levosimendan has improved cardiac performance in left ventricular failure8 – 10 and in myocardial stunning after percutaneous coronary intervention.11 In a randomized, placebo-controlled study of 24 patients undergoing CABG, we demonstrated lower postoperative troponin I concentrations (P,0.05) and a higher cardiac index in those randomized to receive a short duration infusion of levosimendan before the initiation of cardiopulmonary bypass (CPB).12 This pilot study encouraged us to see whether this improvement in postoperative cardiac function would translate into clinical outcome benefit and a consequently shorter postoperative length of stay on the intensive care unit (ICU). Methods Between January 2005 and February 2007, we recruited adult patients with coronary artery disease undergoing elective CABG surgery into our double-blind, single-centre, prospective, randomized, placebo-controlled trial. The study was approved by the local research ethics committee, and all patients provided written informed consent. Inclusion criteria were age 18 yr and an intention to perform first-time multi-vessel CABG. Exclusion criteria were unstable angina, valvular disease, diabetes mellitus treated with sulphfonylurea drugs, renal failure (plasma creatinine.130 mmol litre21), severe hepatic disease (alanine aminotransferase or aspartate aminotransferase.100 IU litre21), severe chronic obstructive pulmonary disease (forced expired volume in 1 s ,50% of predicted or ,2.0 litre), a history of prior CABG surgery or recent myocardial infarction (MI) within the previous month. Randomization was achieved with the use of computer-generated random numbers. The study drug [levosimendan (Abbott Pharmaceuticals, Abbott Park, IL, USA), 24 mg kg21] or an identicalappearing placebo prepared and labelled by the pharmacy was administered as a slow i.v. 50 ml bolus through the central venous port of a pulmonary artery catheter over the 10 min before the initiation of CPB. All patients and medical and nursing staff members remained unaware of study group assignments throughout the study period. In the operating room, patients were connected to routine monitoring, which included five-lead ECG, radial and pulmonary artery catheters, pulse oximetry, and capnography. Anaesthesia was induced with a targetcontrolled infusion of propofol (site effect 1.6– 1.8 mg mL21), sufentanil (0.35 – 0.5 mg kg21), and rocuronium (0.6 mg kg21). After tracheal intubation, the lungs were mechanically ventilated with an oxygen – air mixture (FIO2 40%). Anaesthesia was maintained with propofol (site effect 1.6 – 2.2 mg mL21), sufentanil (0.35 mg kg21 h21), and supplemental boluses of rocuronium. CPB was established with the cannulation of the right atrium and ascending aorta and mild hypothermia (328C). A retrograde coronary sinus cannula was inserted transatrially for cardioplegia infusions (cold-blood cardioplegia 6 – 88C). The first cardioplegia infusion was given antegradely via an aortic root cannula for 2 min, and then retrograde cardioplegia was given for a further 2 min. The potassium concentration of the induction cardioplegia was 20 mmol litre21. After each distal anastomosis, additional cardioplegic solution was delivered for 1 min. Warm-blood retrograde cardioplegia was administered at the end of cross-clamping. A standard coronary artery bypass operation was undertaken using one internal thoracic artery, and one to three peripheral vein grafts obtained from the lower limbs. After rewarming with a 378C maximal heat-exchanger temperature, CPB was discontinued at 36– 378C nasopharyngeal temperature. Intraoperative ventricular tachyarrhythmias were treated with internal cardioversion or lidocaine (1– 1.5 mg kg21). Reversal of heparin was achieved with protamine 1 mg per milligram of heparin. Inotropic support, initially with dopamine (5– 10 mg kg21 min21) and secondly with epinephrine (0.02– 0.15 mg kg21 min21), was commenced if the mean arterial pressure (MAP) was ,65 mm Hg with a cardiac index (CI) 2 litre min21 m22 in the presence of a pulmonary artery wedge pressure (PAWP) of 15 mm Hg and a heart rate of 70– 110 beats min21. I.V. vasoconstrictors were used for a MAP,65 mm Hg, a systemic vascular resistance (SVR) ,800 dyne s21 cm25, and a CI .3 litre min21 m22. Bolus phenylephrine was used until the administration of protamine, after which norepinephrine infusion was used as the vasoconstrictor agent. While in the ICU, patients were routinely sedated with a continuous infusion of sufentanil 0.3 mg kg21 h21 and propofol 1.5 mg kg21 h21 until CI exceeded 2.2 litre min21 m22, no significant dysrhythmias were present, temperature exceeded 368C, haemoglobin .8 g dl21 and no signs of excessive bleeding (.150 ml h21) were present. The patients were weaned from mechanical ventilation with reduction in propofol when the following criteria were met: temperature .368C, maintained haemodynamic stability, chest tube drainage ,100 ml h21, and urine output 0.5 ml kg21 h21. After 15 min, sufentanil was titrated down at 30 min intervals. The tracheal tube was removed when the following criteria were achieved: adequate response to command, arterial oxygen saturation measured by pulse oximetry (SpO2) 95% at a fraction of inspired oxygen (FIO2) 0.5, pH 7.3, arterial carbon dioxide tension (PaO2) 6.7 kPa, and adequate respiratory effort. Patients were eligible for transfer out of the ICU when the following criteria were met: SpO2 90% at an FIO2 0.5 by facemask, adequate cardiac stability with no haemodynamically significant arrhythmia, chest tube drainage ,50 ml h21, urine output 0.5 ml kg21 h21, no i.v. inotropic or vasopressor therapy, and no seizure activity. The criteria for eligibility for hospital discharge were haemodynamic and cardiac rhythm stability, the presence of clean and dry incisions, no pyrexia, the ability to void and move bowels and independent ambulation and feeding. 199 Tritapepe et al. Haemodynamic data [MAP, PAWP, CI, cardiac power index (CPI) and systemic vascular resistance normalized for body surface area (SVRI)] were recorded just before the start of surgery, on admission to the ICU, and at 6 and 24 h later. CPI is a novel haemodynamic measure, which is the product of simultaneously measured CI and MAP.13 Cardiac output was measured using the bolus thermodilution method by injecting 10 ml cold saline at end-expiration. Three measurements within 10% of each other were averaged. Blood samples for cardiac troponin I (cTnI) were drawn at baseline, on arrival in the ICU and at 6, 24 and 48 h after operation. The limit of quantification of cTnI determination was 0.04 ng ml21. When values below the detection limit were reported, zero was used as the value. The coefficient of variation for this assay is 15% for TnI values up to 0.08 ng ml21, 6% for values between 0.47 and 1.44 ng ml21 and 5% for values above 1.44 ng ml21. Standard 12-lead ECG recordings were obtained before operation and on postoperative days 1 and 4. The primary endpoint of the study was the length of ICU stay. Secondary endpoints included the length of hospital stay, tracheal intubation time and reduction in inotropic support over the first 7 days. Additional postoperative data specifically collected included number of deaths, number of acute MIs, incidence of atrial fibrillation, any type of adverse event, and serum creatinine concentrations. The definition of acute MI was as follows: new Q-wave or new persistent ST-segment or T-wave changes accompanied by a creatine kinase MB isoenzyme level .50 units litre21 and a creatine kinase-MB/creatine kinase ratio .5% or a troponin I level .10 mg litre21. A sample size of 100 subjects was estimated to provide a 90% power (with a two-sided a¼0.05) to detect a decrease of at least 11 h (i.e. 24 vs 35 h) in the median ICU length of stay in the levosimendan arm. To account for the skewed distribution of the primary endpoint, sample size estimation was performed using nonparametric methods based on bootstrap simulation. A pilot study data set,12 from which the ICU length of stay empirical distribution had been estimated, was used for the bootstrap resampling.14 One hundred and forty patients were screened for eligibility, anticipating a 40% rate of potential dropouts, either for non-willingness to participate or lack of eligibility. Patients’ baseline characteristics in treated and control groups are reported as mean (SD), median (range), or frequencies and percentages. Differences were assessed using x 2 or the Fisher exact test for categorical variables and the Mann – Whitney U-test for continuous ones. Owing to the non-normal distribution of ICU and hospital stay, the Mann – Whitney U-test was also used to assess differences in the main endpoints between the treatment group and controls. As secondary outcomes, cTnI and haemodynamic data (i.e. MAP, PAWP, CI, SVRI and CPI) were analysed with a hierarchical linear model for repeated measurements to assess differences over time between treatment and control groups.15 16 An unstructured correlation type was used to account for unequally spaced time occasions during follow-up. P-values ,0.05 were considered statistically significant. All analyses were performed using SAS Statistical Package Release 9.1 (SAS Institute, Cary, NC, USA). Results One hundred and forty patients were assessed for eligibility, of whom 106 were randomly assigned to levosimendan (n¼53) or placebo (n¼53). One patient in the levosimendan group and three in the placebo group were withdrawn after randomization because their surgery was cancelled (Fig. 1). Preoperative patient characteristics are summarized in Table 1. The ICU length of stay (time meeting fit-for-discharge criteria) and duration of tracheal intubation were significantly lower in the levosimendan group (P¼0.002 and P¼0.02, respectively), although the hospital length of stay showed no difference between the groups (Table 2). Troponin I increased transiently in both groups (Fig. 2), but this increase was significantly lower in the levosimendan group (treatment-by-time interaction P,0.0001). Haemodynamic data are presented in Figure 3. After operation, there were significantly higher values of MAP, CI and CPI (all treatment-by-time P,0.007) and a lower SVRI (P¼0.005) in those treated with levosimendan. Four patients in the levosimendan group developed hypotension, which was successfully treated with phenylephrine. In the first 7 days after surgery, 34% (17/50) of the patients in the placebo group vs 17.3% (9/52) of the levosimendan patients (P¼0.053) received inotropic support with dopamine 5 mg kg21 min21 (Table 2). The number of patients requiring inotropic support for .12 h was significantly higher in the control group (18.0% vs 3.8%; P¼0.02). The groups were similar with respect to frequency of atrial fibrillation, MI and postoperative serum creatinine .130 mmol litre21, and mortality (Table 2). Discussion Variable degrees of postoperative myocardial stunning occur after cardiac surgery, and these may result in transient myocardial dysfunction. Different cardioprotective strategies have been tested to reduce myocardial injury during cardiac surgery, including short-term preconditioning using ischaemia,17 volatile anaesthetic agents18 – 20 and opiates.21 To our knowledge, the current study using a short-term infusion of levosimendan before CPB in patients undergoing first-time surgical myocardial revascularization is the first to demonstrate a reduction in the ICU stay in addition to reduced tracheal intubation time and inotropic support requirements. 200 Levosimendan pre-treatment in patients undergoing CABG 140 subjects screened for eligibility 34 excluded (20 refused to participate, 14 did not meet inclusion criteria) 106 randomized 53 assigned to receive placebo 53 assigned to receive levosimendan 1 withdrawn as surgery was cancelled 3 withdrawn as surgery was cancelled 52 received levosimendan 50 received placebo Fig 1 Study flow diagram. Table 1 Baseline characteristics. Data are reported as mean (range) for age, mean (SD), median (range) or frequencies and percentages. P-values refer to x 2 or the Fisher exact test for categorical variables and Mann –Whitney U-test for continuous ones Variable Control Treatment n Age, yr Sex: male, n (%) Body mass index, kg m22 EuroSCORE Ejection fraction, % Aortic cross-clamp time, min CPB time, min Number of bypasses ACE-inhibitor, n (%) b-Blockers, n (%) Calcium channel blockers, n (%) Antiarrhythmic drugs, n (%) Diuretics, n (%) Nitrates, n (%) Platelet inhibitor therapy, n (%) Statins, n (%) 50 66.5 (54.0 –87.0) 39 (78.0) 28.8 (2.3) 3.5 (1.0 – 7.0) 44.1 (9.8) 53.6 (7.1) 83.2 (12.4) 3.0 (2.0 – 4.0) 20 (40.0) 40 (80.0) 17 (34.0) 5 (10.0) 10 (20.0) 18 (36.0) 24 (48.0) 39 (78) 52 64.0 (54.0 –86.0) 43 (82.7) 28.1 (2.5) 2.5 (1.0 – 7.0) 41.6 (10.7) 54.6 (6.7) 85.8 (10.2) 3.0 (2.0 – 4.0) 17 (32.7) 43 (82.7) 16 (30.8) 4 (7.7) 9 (17.3) 16 (31.4) 26 (51.0) 41 (79) Table 2 Postoperative results. Data are reported as mean (SD), or frequencies and percentages. P-values refer to x 2 or the Fisher exact test for categorical variables and Mann –Whitney U-test for continuous ones Variable Control Treatment P-value n Thirty-day mortality MI, n Atrial fibrillation, n (%) Time on ventilator, h Received inotropes, n (%) Received inotropes .12 h, n (%) Postoperative serum creatinine .130 mmol litre21, n (%) ICU stay, h Hospital stay, days Re-admission to ICU, n (%) Re-exploration for bleeding, n (%) 50 0 1 10 (20.0) 13.6 (4.5) 17 (34.0) 9 (18.0) 4 (8) 52 0 0 12 (23.1) 11.3 (2.5) 9 (17.3) 2 (3.8) 2 (3.8) NS 0.5 0.7 0.02 0.053 0.02 0.4 32.7 (12.9) 12.0 (2.5) 1 (2.0) 1 (2.0) 24.8 (7.1) 11.1 (2.3) 0 1 (1.9) 0.002 0.09 0.5 0.9 P-value 0.2 0.6 0.07 0.1 0.2 0.4 0.3 0.2 0.4 0.7 0.7 0.7 0.7 0.6 0.8 0.9 A considerable body of experimental and clinical evidence indicates that levosimendan pre-treatment induces protection against subsequent ischaemic stress through its KATP channel-opening properties.22 The opening of mitochondrial KATP channel protects the heart against ischaemia – reperfusion damage.23 The increased potassium influx associated with mitochondrial KATP channel opening is sufficient to protect/preserve mitochondrial function, perhaps via the normalization of matrix and intermembrane space volumes, in situations of distress such as ischaemia or reperfusion. Previous studies have demonstrated improved survival with post hoc treatment with levosimendan after MI9 24 201 Tritapepe et al. Troponin I (ng/ml) 6 Control Control Levosimendan Levosimendan Mean arterial pressure (mm Hg) 4 80 2 0 Baseline 0 76 72 6 24 48 68 h Cardiac index (litre min–1 m–2) Fig 2 Cardiac troponin I concentrations (mean and 95% confidence intervals) in the levosimendan and placebo groups before surgery (baseline), on arrival in the intensive care unit (0), and after 6, 24, and 48 h. 3.5 3.0 2.5 and in one of the two multi-centre studies of patients with acute decompensation of chronic heart failure.25 26 To our knowledge, this study is the first to confirm improved cardiac function (haemodynamics, and inotropic requirements), reduced myocardial damage ( postoperative cTnI concentrations) and outcome benefit (reduced ICU length of stay) with the use of levosimendan pre-treatment. Postoperative serum cTnI concentrations, indicative of myocardial damage, have been shown to increase to some extent in all patients undergoing cardiac surgery, even in the absence of postoperative MI.27 This may be influenced by the type of surgery,28 the choice of cardioplegic solution and its mode of delivery.29 However, after accounting for the complexity of the surgery and other potential confounding factors, cTnI levels at 24 h remain independent predictors of short, medium, and long-term outcome.30 An increased cTnI (.13 ng/ml) in adults undergoing cardiac surgery is associated with major postoperative complications31 with delayed extubation and a prolonged length of ICU stay.32 On the basis of published literature, including our previous pilot study findings,12 we predicted that greater preservation of cardiac function immediately after CPB would result in a better recovery after cardiac surgery. Our results are indeed consistent with these findings. We did not find any significant difference in 30 day mortality, likely because of the low perioperative risk profile of the patients enrolled. Further studies are required to determine whether benefit can be achieved in high-risk patients. Larger outcome effects may be achieved, though potentially, at the risk of more adverse events such as hypotension. We also did not perform any cost– benefit analysis arising from a shorter ICU stay. The duration of tracheal intubation in the current study is comparable with what has been reported in other studies that did not use fast-rack anaesthesia protocols. The length of stay in our ICU and that in hospital are longer than those reported by North American centres33 34 but reflect typical practice in Italy and other countries,35 36 where there is less economic pressure for earlier discharge. 2.0 1.5 Pulmonary artery wedge pressure (mm Hg) 16 14 12 10 Systemic vascular resistance index (dyne s–1 cm–5 m–2) 2100 2000 1900 1800 Cardiac power index (W m–2) 0.6 0.5 0.4 0.3 Baseline 0 6 24 h Fig 3 Longitudinal assessment of arterial pressure, cardiac index, cardiac power index, pulmonary artery wedge pressure and systemic vascular resistance. Data shown as mean and 95% confidence intervals. CPI is a relatively novel haemodynamic parameter, which was the strongest haemodynamic correlate of in-hospital mortality in patients admitted with cardiogenic 202 Levosimendan pre-treatment in patients undergoing CABG shock.13 In our study, levosimendan treatment led to a significant postoperative increase in both CI and CPI. The increase in CPI indicates that increased myocardial contractility contributes to the increase in CI, rather than a reduction in SVRI alone. Reported kinetics for levosimendan37 would exclude the haemodynamic benefit being derived from its calcium-sensitizing effect. We thus feel the observed effect is more likely to be related to a cardioprotective effect that persists after drug elimination. The dosage used and the mode of administration in our study would achieve neither a minimum effective concentration of the drug nor appreciable amounts of its active metabolite, OR-1896.38 Kinetic models have not yet considered the potential influences of hypothermia or CPB; however, we feel this low dose of levosimendan (and its metabolite) is very unlikely to exert any haemodynamic effect after operation. Owing to its KATP channel-opening properties, levosimendan will produce vasodilatation and, potentially, significant hypotension. In our study, we observed mild hypotension (MAP,65 mm Hg) in four patients treated with levosimendan during CPB. This was transient (,10 min) and easily managed by titrated doses of phenylephrine. In conclusion, short pre-treatment with levosimendan in patients undergoing myocardial revascularization resulted in a reduction of tracheal intubation time, decreased requirement for inotropic support and thus a shorter duration of ICU stay. Further studies should investigate patients undergoing high-risk cardiac surgery and procedures where myocardial stress is likely, for example invasive aortic – iliac vascular surgery requiring vessel cross-clamping. Funding This study was funded by an independent research grant from the Department of Anesthesiology and Intensive Care of the ‘Sapienza’ University of Rome. References 1 Christakis GT, Fremes SE, Naylor CD, Chen E, Rao V, Goldman BS. Impact of preoperative risk and perioperative morbidity on ICU stay following coronary bypass surgery. Cardiovasc Surg 1996; 4: 29 –35 2 Loop FD, Higgins TL, Panda R, Pearce G, Estafanous FG. Myocardial protection during cardiac operations. Decreased morbidity and lower cost with blood cardioplegia and coronary sinus perfusion. J Thorac Cardiovasc Surg 1992; 104: 608 – 18 3 Slawsky MT, Colucci WS, Gottlieb SS, et al. Acute hemodynamic and clinical effects of levosimendan in patients with severe heart failure. Study Investigators. Circulation 2000; 102: 2222 – 7 4 De Hert SG, Lorsomradee S, Cromheecke S, Van der Linden PJ. The effects of levosimendan in cardiac surgery patients with poor left ventricular function. Anesth Analg 2007; 104: 766 – 73 5 Toller WG, Stranz C. Levosimendan, a new inotropic and vasodilator agent. Anesthesiology 2006; 104: 556 – 69 6 Michaels AD, McKeown B, Kostal M, et al. Effects of intravenous levosimendan on human coronary vasomotor regulation, left ventricular wall stress, and myocardial oxygen uptake. Circulation 2005; 111: 1504– 9 7 Du Toit EF, Muller CA, McCarthy J, Opie LH. Levosimendan: effects of a calcium sensitizer on function and arrhythmias and cyclic nucleotide levels during ischemia/reperfusion in the Langendorff-perfused guinea pig heart. J Pharmacol Exp Ther 1999; 290: 505 – 14 8 De Santis V, Vitale D, Tritapepe L, Greco C, Pietropaoli P. Use of levosimendan for cardiogenic shock in a patient with the apical ballooning syndrome. Ann Intern Med 2008; 149: 365– 7 9 Moiseyev VS, Põder P, Andrejevs N, et al. RUSSLAN Study Investigators Safety and efficacy of a novel calcium sensitizer, levosimendan, in patients with left ventricular failure due to an acute myocardial infarction. A randomized, placebo-controlled, doubleblind study (RUSSLAN). Eur Heart J 2002; 23: 1422 – 32 10 Russ MA, Prondzinsky R, Christoph A, et al. Hemodynamic improvement following levosimendan treatment in patients with acute myocardial infarction and cardiogenic shock. Crit Care Med 2007; 35: 2732– 9 11 Sonntag S, Sundberg S, Lehtonen LA, Kleber FX. The calcium sensitizer levosimendan improves the function of stunned myocardium after percutaneous transluminal coronary angioplasty in acute myocardial ischemia. J Am Coll Cardiol 2004; 43: 2177 – 82 12 Tritapepe L, De Santis V, Vitale D, et al. Preconditioning effects of levosimendan in coronary artery bypass grafting – a pilot study. Br J Anaesth 2006; 96: 694– 700 13 Fincke R, Hochman JS, Lowe AM, et al. SHOCK Investigators Cardiac power is the strongest hemodynamic correlate of mortality in cardiogenic shock: a report from the SHOCK trial registry. J Am Coll Cardiol 2004; 44: 340 – 8 14 Walters SJ. Sample size and power estimation for studies with health related quality of life outcomes: a comparison of four methods using the SF-36. Health Qual Life Outcomes 2004; 2: 26 15 Singer JD, Willett JB. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence. New York: Oxford University Press, 2003 16 Diggle PJ, Liang KY, Zeger SL. Analysis of Longitudinal Data. Oxford: Oxford University Press, 1994 17 Hausenloy DJ, Mwamure PK, Venugopal V, et al. Effect of remote ischaemic preconditioning on myocardial injury in patients undergoing coronary artery bypass graft surgery: a randomised controlled trial. Lancet 2007; 370: 575 – 9 18 Piriou V, Mantz J, Goldfarb G, et al. Sevoflurane preconditioning at 1 MAC only provides limited protection in patients undergoing coronary artery bypass surgery: a randomized bi-centre trial. Br J Anaesth 2007; 99: 624 – 31 19 Meco M, Cirri S, Gallazzi C, Magnani G, Cosseta D. Desflurane preconditioning in coronary artery bypass graft surgery: a double-blinded, randomised and placebo-controlled study. Eur J Cardiothorac Surg 2007; 32: 319 – 25 20 Tritapepe L, Landoni G, Guarracino F, et al. Cardiac protection by volatile anaesthetics: a multicentre randomized controlled study in patients undergoing coronary artery bypass grafting with cardiopulmonary bypass. Eur J Anaesthesiol 2007; 24: 323 – 31 21 Murphy GS, Szokol JW, Marymont JH, Avram MJ, Vender JS. Opioids and cardioprotection: the impact of morphine and fentanyl on recovery of ventricular function after cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2006; 20: 493 – 502 203 Tritapepe et al. 22 Pollesello P, Papp Z. The cardioprotective effects of levosimendan: preclinical and clinical evidence. J Cardiovasc Pharmacol 2007; 50: 257 – 63 23 Garlid KD, Dos Santos P, Xie ZJ, Costa AD, Paucek P. Mitochondrial potassium transport: the role of the mitochondrial ATP-sensitive K(þ) channel in cardiac function and cardioprotection. Biochim Biophys Acta 2003; 1606: 1 – 21 24 Fuhrmann JT, Schmeisser A, Schulze MR, et al. Levosimendan is superior to enoximone in refractory cardiogenic shock complicating acute myocardial infarction. Crit Care Med 2008; 36: 2257– 66 25 Follath F, Cleland JG, Just H, et al. Steering Committee and Investigators of the Levosimendan Infusion versus Dobutamine (LIDO) Study Efficacy and safety of intravenous levosimendan compared with dobutamine in severe low-output heart failure (the LIDO study): a randomized double-blind trial. Lancet 2002; 360: 196– 202 26 Mebazaa A, Nieminen MS, Packer M, et al. SURVIVE Investigators Levosimendan vs dobutamine for patients with acute decompensated heart failure: the SURVIVE Randomized Trial. JAMA 2007; 297: 1883– 91 27 Jaffe AS, Ravkilde J, Roberts R, et al. It’s time for a change to a troponin standard. Circulation 2000; 102: 1216– 20 28 Etievent JP, Chocron S, Toubin G, et al. Use of cardiac troponin I as a marker of perioperative myocardial ischemia. Ann Thorac Surg 1995; 59: 1192 – 9 29 Chocron S, Alwan K, Toubin G, et al. Crystalloid cardioplegia route of delivery and cardiac troponin I release. Ann Thorac Surg 1996; 62: 481 – 5 30 Croal BL, Hillis GS, Gibson PH, et al. Relationship between postoperative cardiac troponin I levels and outcome of cardiac surgery. Circulation 2006; 114: 1468 – 75 31 Lasocki S, Provenchère S, Bénessiano J, et al. Cardiac troponin I is an independent predictor of in-hospital death after adult cardiac surgery. Anesthesiology 2002; 97: 405– 11 32 Fellahi JL, Gué X, Richomme X, Monier E, Guillou L, Riou B. Short- and long-term prognostic value of postoperative cardiac troponin I concentration in patients undergoing coronary artery bypass grafting. Anesthesiology 2003; 99: 270 – 4 33 Howie MB, Cheng D, Newman MF, et al. A randomized doubleblinded multicenter comparison of remifentanil versus fentanyl when combined with isoflurane/propofol for early extubation in coronary artery bypass graft surgery. Anesth Analg 2001; 92: 1084– 93 34 Cheng DCH, Newman MF, Duke P, et al. The efficacy and resource utilization of remifentanil and fentanyl in fast track coronary artery bypass graft surgery: a prospective randomized, double-blinded controlled, multi-center trial. Anesth Analg 2001; 92: 1094 –102 35 Al-Ruzzeh S, George S, Bustami M, et al. Effect of off-pump coronary artery bypass surgery on clinical, angiographic, neurocognitive, and quality of life outcomes: randomised controlled trial. Br Med J 2006; 332: 1365 – 72 36 Van der Linden PJ, De Hert SG, et al. Hydroxyethyl starch 130/ 0.4 versus modified fluid gelatin for volume expansion in cardiac surgery patients: the effects on perioperative bleeding and transfusion needs. Anesth Analg 2005; 101: 629 – 34 37 Lilleberg J, Sundberg S, Nieminen MS. Dose-range study of a new calcium sensitizer, levosimendan, in patients with left ventricular dysfunction. J Cardiovasc Pharmacol 1995; 26: S63– 9 38 Sundberg S, Antila S, Scheinin H, Hayha M, Virtanen M, Lehtonen L. Integrated pharmacokinetics and pharmacodynamics of the novel calcium sensitizer levosimendan as assessed by systolic time intervals. Int J Clin Pharmacol Ther 1998; 36: 629 – 35 204