Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Duffy antigen system wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Neonatal infection wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Globalization and disease wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Infection control wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Hepatitis B wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Molecular mimicry wikipedia , lookup
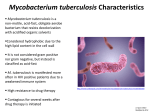
ดร. อมรรัตน อินทรสูต ภาควิชาจุลชีววิทยา คณะแพทยศาสตร มหาวิทยาลัยเชียงใหม • ทราบชนิดของเชื้อกอโรคที่สาํ คัญ ตลอดจนโรคที่เกีย่ วของ จากเชื้อกลุม Mycobacteria และMycoplasmas • ทราบปจจัยการกอโรคของเชื้อที่มีความสําคัญ • รูจักวิธีการรักษาและปองกันโรค • The genus Mycobacterium is the only genus in the Mycobacteriaceae family, Actinomycetales order, and Actinomycetes class. • Over 71 species found in this genus • Aerobic, non-spore forming, non-motile, slightly curved or straight rods (0.2-0.6 x 1.0-10 µm) • Grow more slowly than most other human pathogenic bacteria because of their hydrophobic cell surface (organisms tend to clump, nutrients are not easily allowed into cell) • Extremely slow dividing rate (16-20 hr) • Gram’s stain: Gram positive bacillus (poor stained, beaded rod or ghost cell) • Acid-fastness (20% acid alcohol, modified acid fast : ≤ 5% acid) • Resist to disinfectants and antibiotics • Protein coated on peptidoglycan acts as antigen to induce antibody production and delayed type hypersensitivity (purified protein derivatives; PPD is species-specific; skin test for exposure to TB) Mycobacteria Cellular structure • Gram positive bacteria • Complex cell wall (hydrophobic) ♥ long chain mycolic acid ♥ arabinogalactan ♥ cord factor (trehalose-6,6’dimycolate; granuloma formation, cord formation or serpentine cord) • Lipoarabinomannan : ligand for receptor on mφ • Mycobacteria can be divided into two major groups: 1. Mycobacterium tuberculosis complex 2. Nontuberculous mycobacteria (NTMs) • Smooth to rough colony cauliflower-shaped Mycobacterium smegmatis Mycobacterium tuberculosis Mycobacterium tuberculosis complex: - including M. tuberculosis, M. bovis, M. africanum, M. canetti and M. microti - these species are capable cause of tuberculosis - the main public health problem is M. tuberculosis - M.africanum, M. canetti (rare): significantly cause of tuberculosis in Africa - M. bovis : pasteurized milk has largely reduced infection - M. microti : mostly seen in immunodeficient people M. tuberculosis • discovered by Robert Koch • causes of pulmonary tuberculosis • human is natural reservoir (especially lung) • transmit through the droplets of infected patients (cough, sneeze and speak) • one small droplet nuclei carry 1-3 cells of Mycobacterium • The infectious dose of tuberculosis is very low and inhaling less than 10 bacteria may cause an infection • infect alveolar macrophage in alveoli (intracellular infection) → multinucleated giant cell (Langhans’ cell) → spread to lymph nodes or blood circulation → organs • HMI : induce antibody response (not play the role in protection) • CMI : play a role in killing intracellular pathogen activated mφ (kill microorganism living inside) cytotoxic T-cell (kill infected mφ) Lesion at the upper lobe of lung (Gohn focus) spread over the lung (miliary tuberculosis) Granuloma formation around the inflammatory tissue Careous necrosis (Tissue necrosis caused by immune response) Tubercle in lung (fibrous formation around necrotic tissue) Scar formation cavity (Fibrosis or calcification) (The organisms are released after breaking of tubercle) Signs and symptoms: range from asymptomatic (predominant) to acute infection 1. Pulmonary tuberculosis: 75% of the cases - chest pain, coughing up blood (prolonged cough > 3 weeks) 2. Extrapulmonary tuberculosis: Systemic symptoms - fever, chills, night sweats, appetite loss, weight loss, fatigue, etc. - Ex. meningitis in central nervous system urogenital tuberculosis in genitourinary system 3. Co-exist tuberculosis: Pulmonary & extrapulmonary tuberculosis Laboratory diagnosis 1. Specimens: expectorated sputum, urine, CSF, blood, feces, etc. adequate sputum : PMN>25 cells/LPF, squamous epithelial cell < 10 cell/LPF 2. Chest x-ray: granuloma formation 3. Tuberculin skin test or Mantoux test: - A primary means to identify individuals infected with M. tuberculosis (MTB) - After 48-72 hr intracutaneously injected with culture extract of MTB, a person who has been infected will exhibit a delay type hypersensitivity (erythema or redness on the skin) 4. Direct stain: Acid-fast stain (Kinyoun, Ziehl-Neelsen) (stain with carbolfuchin and counter stain with methylene blue) 5. Culture: contain malachite green or antibiotics to inhibit the contaminants Lowenstein-Jensen medium (egg-based medium) Middlebrooks medium (agar-based medium) conditions: 35 oC, 5-10% CO2 incubate 6-8 wks (antibiotics : polymixin B, amphotericin B, nalidixic acid, trimethoprim, azlocilin; PANTA) 6. Nucleic acid analysis : PCR, DNA probe etc. 7. Biochemical test : many enzyme production etc. 8. Antigen detection : ELISA, agglutination test etc. Acid-fast staining (Kinyoun’s method) A drop of distill water Smear the organism on glass slide flaming stained with Kinyoun carbon fuchsin (phenol) for 3-5 min washing Decolorized with acid alcohol washing counter stained with Methylene blue for 1 min washing The genus Mycobacterium and the genus Nocardia are acid-fast (stain red). Other bacteria will be decolorized and stain blue. Acid-fast stain: positive Acid-fast smear reporting (WHO) Examination No. of fields examined Result Grading >10 AFB/oil field 20 positive 3+ 1-10 AFB/oil field 50 positive 2+ 10-99 AFB in 100 oil fields 100 positive 1+ 1-9 AFB in 100 oil fields 100 scanty record actual number No AFB in 100 oil fields 100 negative 0 Chest x-ray: granuloma formation Tuberculin skin test (injection with PPD) The test is designed to measure delayed-type hypersensitivity reactions. An infected individuals, the body will recognize the antigens in the Tuberculin and cause a local reaction at the site of injection. (also found in person with BCG vaccination or TB exposure in history) False negative : immunocompromise patient, AIDS Treatment: combined drugs isoniazid, rifampin, ethambutol, pyrazinamide, streptomycin Prevention: vaccine - usually uses Bacille Calmette-Guérin (BCG) live attenuated vaccine (from M. bovis BCG) for infants (up to 80% protection) Nontuberculous mycobacteria (NTMs): NTMs was classified into 3 groups 1.1 Rapidly growing NTM (gr. 4) 1.2 Slow-growth NTM (divided into 3 groups bases on phenotypic characteristics) 1.2.1 Photochromogens (gr. 1; colonies become pigmented when exposed to light) 1.2.2 Scotochromogens (gr. 2; colonies are pigmented when grown in the dark) 1.2.3 Nonphotochromogens (gr.3; produce no pigment) 1.3 Nonculturable NTM (Leprosy caused by M. leprae) ( Runyon’s classification of NTM : group 1- 4 ) 1.1 Rapidly growing NTM - culture colonies appear in ≤ 7 days - Gram’s stain: GPB resembling diphtheroids - ubiquitous in the environment (soil, river, etc.) - may be commensals on the skin - mostly potential pathogenic in immunocompromised patients - Pathogens: M. fortuitum, M. chelonae, M. abscessus 1.2 Slow growth NTM - culture over 7 days - ubiquitous in the environment (soil, river, etc.) and animal (pigs, chickens, cats, dogs) - Natural waters served as the major reservoir for most human infections - route of infection : eating contaminated food or water, inhalation of infectious droplet - mostly potential pathogenic in AIDS patients (30-50%) - Pathogens: M. avium, M. intracellulare, M. paratuberculosis (called M. avium complex or MAC) 1.3 Nonculturable NTM - caused of Leprosy or Hansen’s disease (chronic disease of skin, mucous membranes, and nerve tissue) -M. leprae is the only one species that has not yet cultivated in vitro - Incubation time : 2-10 years (doubling time ~14 days) - Natural habitat: human, armadillo - it could be cultivated in armadillo and footpads of mice - most prevalent in tropical countries - Infection is acquired from infected patients (human to human) through close contact, nasal secretion • Intracellular infection (WBC, nerve cell) • Pathogen → upper respiratory tract → blood circulation → skin & nerve (temperature < 37 oC) • Skin : hypopigmentation, papule, nodule, skin infiltration • Nerve : peripheral neuropathy • clinical manifestation : 1. Tuberculoid leprosy : mild symptoms (low HMI, low rate of transmission) 2. Lepromatous leprosy : severe symptoms (low CMI, high rate of transmission) Diagnosis - Direct stain: acid-fast stain - Culture: Similar to MTB (except M. leprae) Treatment - Many infections caused by NTMs are resistant to primary regimen of antituberculous agents. (at least four agents). • Mycoplasmas หมายถึงเชื้อที่เปนสมาชิกใน genus Mycoplasma และ genus Ureaplasma Family : Mycoplasmataceae Class : Mollicutes (soft skin, สิ่งมีชีวิตเซลลเดียวขนาด เล็กที่สุด ไมมีผนังเซลล และสามารถดํารงชีวิต อยางอิสระ) • การจําแนก species นิยมใชโครงสรางแอนติเจน และโครงสราง ทางพันธุกรรม • Mycoplasmas พบเปน normal flora ในสัตวเลี้ยงลูกดวยนม, สัตว มีกระดูกสันหลัง แมลง และพืช • เปน normal flora ในคนบริเวณเยื่อเมือกบุผิว • ไมมีผนังเซลล เซลลถูกลอมดวยเยื่อหุม เซลลเทานั้น ( จึงไมสามารถยอมติดสี แกรม ) • มีสาร sterol เปนสวนประกอบของเยื่อหุม เซลล ( ไมมใี นแบคทีเรียทั่วไป ) • มีขนาดและรูปรางไมแนนอน M. pneumoniae มีรูปแทง ปลายเรียว หรือเปนสาย U. urealyticum, U. hominis มีรูปกลม • มีขนาดเล็กมากคลายไวรัส (แยกดวยการแบงตัว, DNA+RNA, เพาะเลี้ยงไดดวยอาหารเลี้ยงเชื้อ) • สวนใหญเปน facultative anaerobe (M. pneumoniae เปน strict aerobe) • อาศัยอยูภายนอกเซลล (extracellular bacteria) แตสามารถพบ เชื้อภายในเซลลได • พบการกอโรคไดทั้งในคน สัตว และพืช • Protein และ glycolipid ในชั้น cell membrane มีคุณสมบัติเปน antigen แตสามารถเกิด x-reaction กับ เชื้อแบคทีเรียชนิดอื่นและ เซลลคนได • ดื้อตอยากลุม ที่ออกฤทธิ์กับผนังเซลล • ขนาดสารพันธุกรรมเล็กกวาแบคทีเรียอื่น • ตองการสารอาหารพิเศษจากภายนอก เชน sterol ซึ่งเปน สวนประกอบของ cell membrane • มีอัตราการเจริญชา ระยะเวลาแบงตัวนาน ตางกันไปตาม species • เชื้อตายงายในสภาวะแวดลอมไมเหมาะสม เชน ในที่แหง อุณหภูมิ สูง • M. pneumoniae ( โรคติดเชื้อในระบบทางเดินหายใจ ) • M. hominis ( เปน normal flora ในระบบสืบพันธุ, กอโรคในระบบ ทางเดินปสสาวะและอวัยวะสืบพันธุ ) • U. urealyticum ( พบอาศัยอยูไดบริเวณอวัยวะสืบพันธุ กอโรคใน ระบบทางเดินปสสาวะและอวัยวะสืบพันธุ ) • กอใหเกิดการติดเชื้อในระบบทางเดินหายใจเปนสําคัญ • Route of infection : ทางการหายใจ (ละอองอากาศที่ปนเปอน) • ระยะฟกตัว : 2-3 สัปดาห • การกอโรค : อาศัยโปรตีน P1 adhesin รวมกับโปรตีนชนิดอื่นที่ cell membrane ในการเกาะติดกับ receptor ที่สวนฐานของ cilia ของเซลลเยื่อบุทางเดินหายใจ และทําใหเกิดภาวะ cilliostasis (ยับยั้งการทํางานของ cilia) และทําลายเซลลเยื่อบุผิว จนเชื้อ สามารถเขาสูทางเดินหายใจสวนลางและกอใหเกิดการติดเชื้อ • ปจจัยการกอโรค : ยังไมทราบแนชัด ( hemolysin, inflammation, autoantibody) • อาการทางคลินิก : อาการไมรุนแรง – อาการรุนแรง • อาการในระยะแรกมักคลายไขหวัดใหญจากเชื้อไวรัส ในระยะ หลังมีการไอพรอมเสมหะเปนมูกเปนเลือด • เด็กเล็กและผูสูงอายุอาจมีอาการรุนแรง • โรคติดเชื้อทางเดินหายใจที่พบบอยสุด คือ หลอดลมอักเสบ • การติดเชื้อในเด็กเล็ก : โรคติดเชื้อในทางเดินหายใจสวนบน • การติดเชื้อในเด็กโตและผูใหญ : โรคติดเชื้อในทางเดินหายใจ สวนลางและโรคปอดบวม (atypical pneumonia อาการไมคอย รุนแรงเมื่อเทียบกับโรคปอดบวมที่เกิดจากแบคทีเรียชนิดอื่น, community-acquired pneumonia) • โรคสามารถหายไดเองใน 1-2 สัปดาห ( ยาปฏิชีวนะจะลดระยะเวลาดําเนินโรค ) • ผูปวยโรคเอดสมักพบการติดเชื้อแบบลุกลามเขาสูอวัยวะตางๆ และรักษาไดยาก • การวินิจฉัยโรคโดยพิจารณาจากการตรวจพบเชื้อจากสิ่งสง ตรวจอาจเกิดความผิดพลาด เพราะเชื้อสามารถอยูใน ทางเดินหายใจไดหลังจากหายจากโรคแลว ดังนั้นควรอาศัย ลักษณะอาการทางคลินิกควบคูดวยเสมอ • สิ่งสงตรวจ : เก็บจากตําแหนงที่ติดเชื้อ เชน เสมหะ น้ําจาก เยื่อหุมปอด การตรวจพิสูจนเชื้อ • การตรวจโดยตรง : เชื้อเล็กมากและไมติดสียอมแกรม (จึงไม มีประโยชน) แตสามารถตรวจหา antigen หรือสารพันธุกรรม ของเชื้อได • การเพาะเชื้อ : M. pneumoniae มีอัตราการเจริญชาตอง เพาะเลี้ยงในอาหารที่มี sterol เปนสวนผสม เปนเวลานาน กวา 21 วัน จึงมีความยุง ยาก ไมเหมาะสมกับหอง Lab ทั่วไป • การทดสอบทางชีวเคมี : ไมนิยมทํา เพราะเชื้อหลาย species ใหผลการทดสอบคลายกัน • การทดสอบทาง serology : คนทั่วไปอาจมี antibody ตอเชื้อ Mycoplasma ที่เปน normal flora บริเวณทางเดินปสสาวะ และระบบสืบพันธุได จึงไมนิยมทํา การตรวจหา antigen มี ขั้นตอนยุงยากไมนิยมทําในหองปฏิบัติการทั่วไป • การตรวจหาสารพันธุกรรม : มีบทบาทมากขึ้น แตมักทําใน หองปฏิบัติการอางอิง • ยากลุม tetracyclines และ macrolides เปน drug of choice ของ M. pneumoniae (แตถา เชื้อสัมผัสยาแลว มีโอกาสดือ้ ยาได ; acquired resistance) • ระวังการแพรกระจายเชื้อจากผูปวย • วัคซีนปองกันโรคติดเชื้อ M. pneumoniae มีประสิทธิภาพต่ําและไม เปนที่นิยม • Murray PR et al. Medical Microbiology. 2005 • Nancy AK. Tuberculosis: Pathophysiology, Clinical Features, and Diagnosis. Clinical journal of the American association of Critical-Care Nurses. 2009. • ภัทรชัย กีรติสิน. วิทยาแบคทีเรียการแพทย พิมพครั้งที่ 2. กรุงเทพฯ: หจก. วี. เจ. พริ้นติง้ , 2551