Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Left Ventricular End-Diastolic
PressureVolume Relationships
in Hypertrophic
Card iomyopathy*
Changes
Michael
Induced
Tendera,
by Verapamil
M.D.;t
Lech
Polonski,
M.D.;
and
Ewa
In 16 patients
with hypertrophic
cardiomyopathy,
an acute
response
of the left ventricular
end-diastolic
pressure
and
volume index to intravenously
administered
verapamil
was
assessed.
Verapamil
decreased
the left ventricular
enddiastolic pressure
from 20 ± 6 to 17 ± 5 mm Hg(p<O.001)
and
increased
the end-diastolic
volume
index from 82 ± 22 to
V
erapamil
the
Both
has
been
treatment
symptomatic
modynamic
some
found
a promising
effects26’#{176}”
and
were
indicate
however,
this
‘
he-
Results
verapamil
in patients
diomyopathy;4’5’
in
beneficial
reported.
that
hypertrophy
drug
cardiomyopathy.
improvement59
studies
reverse
to be
of hypertrophic
may
of
actually
with
hypertrophic
opinion
has
filling
filling
volume
projection
present
study
in left
volume
in
of
MATERIALS
Sixteen
(mean
patients
was
SD,
±
evidence
thickness
ratio
minutes
after
cardiac
output
values
were
All
patients
pressure
gradient
of2O
demonstrated.
All
and
After
heart
informed
0.1 mg/kg
were
catheter
(mean,
mg/kg/mm.
49.9±36.7
mm
no gradient
for 48 hours
was
in the
using
the
onset
a cardiac
After
plane
ofthe
output
obtaining
left
*Fmm
the
Academy,
tCardiology
Nashville,
Manuscript
QRS
computer
complex.
baseline
ventriculographic
Second
Zabrze,
Fellow,
Tenn.
received
pressures
study
orally,
was
to
to each
a Swan-Ganz
pulmonary
artery.
catheter
Department
output
Left
(Cordis
was calculated
Laboratories
9520
and
output,
in the
cardiac
30#{176}
right
November
of
29; revision
left
wall
the study
in all patients.
et
as well
Data
al,’6
the
Judkins
peak
as basal
were
by
of
completed
lesions
loading
were
aorta
gradients,
using
found.
conditions
in the
outflow
left
Selective
technique
pressures
statistically
area-
established
thickness
coronary
left ventricular
analyzed
again.
a planimeter.
of systolic
systolic
of
to the
was
mean
with
influence
of
by infusion
done
index
the
No obstructive
the
an
according
and
measured
point
in a dosage
all measurements
were
mass
employing
measurements,
measured.
infusion,
calculated
ventricular
was
to assess
ventricle,
were
given
followed
ventriculograms,
Rackley
free
on
and
left
were
Students
also
t-test.
RESULTS
a single-
Silesian
oblique
Medical
results
significantly
tolic
pressure
(p<0.001)
Thomas
accepted
Hospital,
February
24.
Pressure-volume
and
are
summarized
decreased
from
in Table
1. Verapamil
both left ventricular
136±41
to 115±30
systolic
aortic
pressure
peak
mm
from
111
±
102 ± 15 mm Hg (p<O.OOl).
The left ventricular
flow gradient,
present
at rest in eight
patients,
reduced
by verapamil
in seven
and
remained
changed
gradient
in one (baseline
after verapamil,
In no instance
did
the
aortic
fall in peak
finding.
The LVEDP
the
represents
( 15 percent
Relationships
from
gradient
increase,
pressure
declined
20±6
by
1 to 8 mm
in one, and
mean
value
to 17±5
Cardiomyopathy
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21369/ on 05/04/2017
even
was a uniform
mm
17 to
outwas
un-
though
concomi-
Hg
in 14 pa-
rose by 3 mm
for LVEDP
Hg (p<0.001).
an average
decrease
in LVEDP
of the control
value).
in Hypertrophic
sysHg
gradient,
50 ± 37 mm
Hg;
25±28
mm Hg [p<O.OOl}).
tients,
remained
unchanged
Hg in one
patient.
The
dropped
University-St.
the
minutes,
these
At that
was
ofthe
of
In all patients,
to baseline.
minutes
as left
arteriograms
tant
anterior
of Cardiology,
by
A).
Poland.
Vanderbilt
ten
volumes
coronary
The
Hg)
prior
explained
a pigtail
Cardiac
(Edwards
After
method,n
repeated.
two
analyzed.
measurements
(Isoptin)
over
wall
F 8). Pressures
were measured
by means of transducers
(Statham
P
23 ID), with
the
zero
reference
point
at midchest
level.
Left
ventricular
end-diastolic
presure
(LVEDP)
was measured
50 msec
after
returned
as well
ventricular
intraventricular
eight,
withheld
to have
weight
ventricular
method
cardiac
obtained.
placed
performed
to free
of other
An
10 mg of diazepam
was
was
absence
procedure
was
with
a septal
rhythm.
Hg
17 to 51 years
were
ventriculo-
were
ventriculogram,
of verapamil
of body
adequate
arrhythmias,
first
of
echocardiographic
with
remaining
ofthe
consent
catheterization
sinus
in the
nature
premedication
All had
in the
to 130 mm
medications
The
thermodilution
in
patients;
investigation.
patient,
1.5’’
were
in eight
studied.
found
technically
pressure
injection
In order
aged
and
the
an augmentation
pressure.
Only
Twenty
diastolic
women)
hypertrophy
than
depend
METHODS
three
were
septal
greater
disease.
found
and
33 ± 10 years)
ofasymmetric
of
changes
performed.
catheter-induced
the
measurements.
AND
(13 men
and
producing
filling
without
length
administration
if these
hemodynamic
evaluate
pressure
acute
to determine
baseline
to
end-diastolic
setting
and
on the
undertaken
ventricular
the
verapamil
was
conditions,
at a lower
grams,
Left
changes
54
ventricular
of pressure,
The
the
91 ± 23 ml/sqm
(p<O.Ol).
In 13 (81 percent)
of 16 patients,
an
improvement
of end-diastolic
pressure-volume
relationships
occurred.
In hypertrophic
cardiomyopathy,
intravenous
verapamil
exerts
a beneficial
effect
on
left
0.01
gained
wide
was
M.D.
intravenous
car-
not
Kozielska,
(‘Tendera.
This
by 3 mm
Polonski,
Hg
Kozi&ska)
Table
1 -Baseline
Hemodynarnic
LVEDP,
LVEDVI,
Hg
lUllS
Verapaniil-Induced
us
,-#{176}----.
m
A
B
A
Hypertrophk
Cardiomyopathy*
Basal
Outflow
per
LVSP.
miii
mm
-,.-----,
,-.-----.,
B
with
in Patients
Rate,
beats
inllsq
Case
Changes
Heart
LVESVI.
iiil/sq
,-.-,---.--‘
and
Data
AoSP,
Hg
mm
,.-.--.--.,
B
A
B
A
A
LV Free
Gradient
Hg
mm
,-.-----.----‘
B
LV
Hg
A
Wall
Mass
Thick-
Index,
,-#{176}----‘
B
LV
B
A
g/sq
ness,
in
mm
1
20
13
60
77
9
16
72
67
90
90
90
90
134
12.6
2
20
19
85
86
21
18
66
72
140
102
100
92
40
10
352
21.3
3
22
16
100
105
12
20
88
93
240
180
110
100
130
80
225
19.0
4
32
28
77
65
16
13
65
76
181
143
104
95
77
48
241
19.5
5
15
14
95
94
27
30
73
82
105
96
105
96
492
28.0
6
13
10
109
110
28
21
84
82
105
100
105
100
173
12.8
7
20
18
106
129
25
30
61
72
120
100
120
100
280
17.4
8
18
16
109
131
18
32
66
71
137
110
100
100
37
10
478
25.4
30
30
9
16
14
70
78
13
21
86
92
190
165
160
135
276
20.3
10
13
9
56
58
18
19
68
69
100
95
100
95
150
14.0
11
13
16
83
83
17
13
87
83
110
90
110
90
245
17.5
12
32
25
48
76
7
9
88
86
110
104
110
104
353
32.3
13
22
16
56
62
7
8
90
87
120
110
120
110
396
27.0
14
24
16
112
119
24
26
62
72
115
85
90
85
25
0
314
19.6
15
20
17
60
85
16
15
79
85
170
162
130
140
40
22
329
24.1
279
18.4
16
22
22
86
98
23
20
60
62
140
105
120
105
20
0
Mea,i
20t
17t
82
911
18
19
751
781
136t
115t
lilt
102t
50t
25t
±SD
±6
r22
-r23
±7
±7
±9
±41
±5
*B, Baseline;
tp<0.00l
A, after
The
left
value
ventricular
of82
in
± 22
after
changed
(in
was
in ten,
and
m (11
LVEDVI
a range
of
percent
remained
± 3
declined
remained
unchanged
decreased
in two.
mI/sq
by
peak
-‘30
±17
systolic
pressure;
in
in
in nine
verapamil
was
not
32-
r15
and
Un-
subjects,
subject.
±37
AoSP,
±28
aortic
rose
between
state and
in five,
30
I
-
peak
systolic
pressure.
--
28-
26
24
22
20
.
\
in
In
12
with
and six without
obstruction),
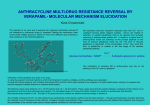
shifted
downwards
and to the right;
the LVEDVI
This group
percent)
represents
a
favorably
modified
left
the
remaining
three
in both
pressure
end-diastolic
pressure
This
last
tion.
Relationships
verapomil
veropomal
I
;
-
a
#{149}
\;.I
L 160
-
-.
o
6 -
50
(81
pressure-
verapamil.
the
in
rose while
of 13 pa-
fraction
in
whom
ventricular
filling
patients,
two showed
a
and volume,
and in one,
increased
patient
had
between
LVEDP
in Table
vs baseline
2. Changes
Table
2-Correlation
induced
Changes
with
no
no basal
changes
hemodynamic
in LVEDVI
in
in
change
outflow
obstruc-
LVEDVI
and
indices
are
did not depend
shown
on the
\
(\
\\
-
Of
volume.
\
-
2
after
by
one (with a low basal gradient),
LVEDP
remained
unchanged.
decrease
\
8-
(4
before
in end-diastolic
induced
conditions.
significant.
0
I
patients
(six
relationships
verapaniil
and
mean values
19 ± 7 mI/sq
changes
relationships
tients
volume
index
The LVESVI
patients,
statistically
of the
in one
1 shows
volume
P
(mmHq)
(0
five
Figure
mean
mean
virtually
m)
12 rnl/sq
The difference
m in the control
of 18 ± 7 mI/sq
FiGURE
ventricular
index
the
The
n (p<0.Ol).
mI/sq
9
The
from
The
left
ventricular
end-systolic
(LVESVI)
was not uniformly
changed.
diastolic
left
volume
verapamil
to 91 ± 23 mi/sq
LVEDVI
value).
LVLDP
LVSP,
end-diastolic
increased
control
after
rll
ventricular;
for B vs A.
for B vs A.
(LVEDVI)
rose
LV, left
for B vs A.
1:p<O.Ol
§p<O.O2
rise
vezapamil;
70
1. Verapamil-induced
pressure-volume
80
(
#{246}
%
90
relations.
S-..
Coefficients
and
Baseline
x
(0
changes
BSA,
I
I
20
30
40
EDVI
Values*
LVEDVIt
r=
LVEDP
LV issass index
LV free wall thickness
T
Verapamil-
y
LVEDVI
00
between
Hemodynamic
-0.167
r=0.226
r=0.159
r = 0.204
r=
r
r
-0.528
r = 0.152
0.347
-
0. 132
8LV Left ventricular.
(mI/m2BSA)
in left ventricular
Body surface
area.
LLVEDPt
end-
tChanges
induced
by verapalnil.
p<0.05.
CHEST
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21369/ on 05/04/2017
I
84
1 1 I JULY,
1983
55
.
3.0
cardiac
y2.09
-0.269x
-0
00’
..
-.-
.
-30
0.
left
ventricular
to baseline.
Bonow
et al,
recently
reported
techniques,
.
,-
-.-
528
.
output
returned
S
and
higher
doses
trophic
cardiomyopathy,
that
this
and
not
of
finding
in
from
LVEDV
patients
further
with
with
hyper-
supporting
direct
had
radionuclide
increasing
verapamil
results
pressures
using
12
the
action
view
ofverapaniil,
S
WI
>E
-‘a
of the
contrast
material.
..,.-
The
-60
most
pronounced
hypertrophic
pathophysiologic
cardiomyopathy
is
feature
an
of
impairment
of
S
diastolic
-9.0
represents
is due
10.0
I
5.0
20.0
LVEDP
2. Correlation
FIGURE
verapainil
and
baseline
values.
found
between
baseline
I
I
25.0
30.0
35.0
produced
by
values.
A significant
between
the
negative
extent
changes
in LVEI)P
p<O.OS;
There
Fig 2).
was
no
and
significant
changes
in
left
of
correlation
LVEDP
(r=
peak
ventricular
induced
by verapamil
(r =
0. 117) and LVEDVI
systolic
and
changes
(r = 0.311).
-
The
present
study
in
filling
All
instances
indicates
LVEDP.
occurring
included
Verapamil
effect.
substantial
decreased
In our
pressure.
study
had
this
group
ume
values
Left
ventricular
may
be
to
been
material;
the
56
affected
however,
contrast
minutes
effect
volumes
we
injection.
starting
by the
first
hemodynamic
medium
after
by
calculated
should
1921
We
administration
after
injection
changes
be
negligible
effect
since
be affected
by
changes
and
in
between
rather
the
to see
altered
may be
measure-
it
involved.
this
observed
Therefore,
study
to
the
form
can
and
studied,
benefi-
verapamil
or improved
Rosing
state
that
patients
ofthe
disease
may
adversely
form
any
with
the
respond
detrimental
verapamil
hemoin any of
left ventricular
outflow
gradient
patients
in whom
it was present
in
conditions.
nor
or
In
none
the
two
of contrast
induced
by
15 to 20
this
after
Pressure-dume
to left
change
ofthose
none
of
study
systolic
of verapamil
the
tended
ventricular
in
them
drop
to
be
ventricular
in
was
a rise
it
variations,
patient
to verapamil
baseline
hemodynainic
Whether
an acute
information
long-term
regarding
treatment
We
conclude
patients
travenous
end-diastolic
Relationships
that
with
can serve
LVEDP
in
pressures.
significant,
in
was
weak
could
verapamil
the
left
correlation
considerable
response
be
of
In our
higher
with
and
of a given
established
from
measurements.
response
to the
drug
predictability
of the
remains
questionable
in a considerable
acutely
improves
Cardiomyopathy
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21369/ on 05/04/2017
carries
any
results
percentage
of
left
inventricular
relationships,
(Tendera,
in
8
cardiomyopathy,
pressure-volume
in Hypertrophic
by
with
the
not
thickThus,
patient.
Although
so that
wall
as a predictor
induced
patients
hypertrophic
verapamil
index,
conditions.
in a particular
greater
filling
mass
loading
measurements
efficacy
individual
verapamil
virtually
excluded
of verapamil
the
pressure-vol-
of 16 patients
our patients.
The
declined
in all eight
was
of
from
it
clarify
if verapamil
end-diastolic
to verapamil.
We did not see
dynamic
effect
with
intravenous
ness,
a
with
of
relaxation,
interaction
are
of
not
properties
relations.
volume,
of LVEDP
after
or near
normal
Values
this
clear,
LVEDP
observed.
The extent
ofimprovement
in LVEDVI
and LVEDP
was not related
to the baseline
ventricular
diastolic
signifi-
a common
were
ventriculograms.
have
but
baseline
response.6
consecutive
also
objective
modify
Epstein
verapamil
negative
in-
congruent
Hg). Elevation
with
normal
appears
can
mechanical
mechanisms
an
obstructive
elevated
pressure
ofpatients,
in LVEDP,
(13 to 16 mm
in patients
passive
conditions,
what
not
LVEDP
former
observations
by Kaltenbach
et al,5 Bonow
et al,2
and Rosing
et al.6 Only
one patient,
with
the nonobstructive
form ofthe
disease,
had an elevation
of the
baseline
ventricles.
two
mechanism,
lowers
LVEDP
and
a beneficial
effect on
relations,
with
larger
at lower
in this
decrease
LVEDP
verapamil
the
cially
hypertrophic
than
hypertrophic
cardiomyopathy,
to elevate
LVEDP’7”8
due to its
otropic
is not
curve
but
loading
pressure
both in patients
with and without
obstruction.
normal
subjects
and in patients
with
conditions
In
in
myocardium,
between
cantly,
other
tends
changes
systolic
intravenous
with
pressure-volume
volumes
patients
by
pressure-volume
In 13 (81 percent)
that
in patients
cardiomyopathy
in most
increases
LVEDVI.
This
Whether
acutely
improved
LVEDP
and LVEDVI
the LVEDP
without
affecting
the volume.
demonstrates
of verapamil
end-diastolic
only
ments,
-0.528;
DISCUSSION
infusion
diastolic
was
correlation
filling.
in compliance
As pointed
out by Glantz
and Parmley,2
difficult
to sort out, even with high-fidelity
was
verapamil-induced
baseline
the
the
in LVEDP
change
shift
rela-
I
BASELINE
mmHg
changes
improved
to a true
verapamil-induced
pressure-volume
.
ventricular
tions
I
The
end-diastolic
compliance
of left
resulting
Polonski,
Kozie/ska)
in lowered
filling
volume.
Response
pressure
and an augmented
filling
to verapamil
cannot
be predicted
on
the grounds
ofbaseline
to be assessed
in every
hemodynamic
findings
patient
individually.
and
has
1 1 Hanrath
of
We thank
Dr.
septal
W. B. Campbell
for review
13
of the manuscript.
DG, Kremer
on
the
left
P, Sonntag
ventricular
cardiomyopathy.
Am J Cardiol
12 Troesch M, Hirzel HO, Jenni
thickness
septal
ACKNOWLEDGMENT:
P, Mathey
verapamil
following
hypertrophy
Doi
YL,
1980;
verapamil
WJ,
Mode
echocardiography
nostic
criteria
J,
prediction
HP
Reduction
with
1979;
JE M-
Goodwin
cardiomyopathy:
ofobstruction.
of
assymetric
60:11-155
CM,
Oakley
in hypertrophic
and
hypertrophic
in patients
Circulation
Gehrke
W. Effect
in
45:1256-64
R, Krayenbuehl
(abstract).
McKenna
F, Bleifeld
filling
diag-
J Cardiol
Am
1980;
45:6-14
REFERENCES
1 Bonow
SI,
RO, Ostrow
function
reduced
stract).
2 Bonow
SI,
et
RO, Ostrow
HG,
(abstract).
Bonow
RO,
Rosing
Lipson
u:,
et al. Effect
and
M,
Therapie
5
Kaltenbach
1976;
M,
Hopf
Treatment
of
verapamil.
Br Heart
ES.
DR.
Verapamil
treatment
effects.
7 Rosing
fects
G.
1979;
a new
RO,
(abstract).
filling
Am
ventricle
a new
Am
BJ,
Maron
SF,
M,
DR.
the
19
to the
pharmacologic
I.
Hemodynamic
with
1981;
Am
Singh
20
Lewis
BS,
of verapamil
HT,
echocardi-
Cardiol
1981;
plane
volume
Coble
YD,
mass
MB,
to
21
Mullins
Mitha
48:418-28
angiocardiograms
in man.
Hay
in
Am
J
Heart
RE.
man.
A method
for
Circulation
1964;
CB,
22
Stern
Goodwin
48:545-53
23 Goodwin
Verapamil
the
of
capacity
24 Glantz
LC,
25 Karliner
ventricu-
Cardiac
cardiomyopathy
RB,
diastolic
1981;
Jones
RN,
mechanics
47:411
MS.
Immediate
Cardiology
verapamil
Am
on
J 1977;
Heart
haemodynamic
1975;
WS.
Aronow
60:366-76
Effect
of verapamil
disease.
on
Circulation
1979;
Mierzwiak
BG,
DS,
GJ,
Markham
coronary
JE
Hypertrophic
HD,
Mitchell
function
produced
Am Heart
J 1972; 83:373-81
Dehmer
ejection
Alsobrook
ventricular
media.
and
Rankin
of the
identity.
R\
in
by
Lewis
arteriography
fraction
SE,
the
Hillis
on left ventricular
man.
J Cardiol
Am
(Vol
SA,
26
Epstein
Cardiol
1980;
trends
10).
Peterson
systolic
and
Res
KL,
Ross
diastolic
catheterization
and
JF,
and
Factors
Circ
I. predictions
Goodwin
Lea
WW.
curve.
eds.
Febiger,
which
1978;
J
in search
45:177-80
in cardiomyopathy:
Philadelphia:
Parmley
a disease
1980;
In: Yu PN,
volume
JS,
cardiomyopathy:
J
Am
JF Future
mechanics:
Febiger,
Peyton
JS,
cardiomyopathies.
pressure
Lipson
disease.
in coronary
ofselective
cardiology
60:1208-13
on left
JL,
in left
L, Firth
SE.
MV,
Gotsman
in man.
Leshin
Effect
of its own
Ef-
treatment
AS,
of contrast
1981;
Green
of intravenous
heart
46:827-31
pharIII.
on exercise
Effects
with
performance
Changes
LD.
Bonow
the
AHG.
J, Easthope
Ferlinz
injection
47:409
Cardiol
J
ventricular
in patients
effects
Cardiol
hypertrophic
on the
two-dimensional
Am
ventricular
Roche
BN,
Epstein
ofverapamil
GL,
J
Leon
approach
SL,
effects
significance
in hypertrophic
59:313-19
Y.
with
BJ, Epstein
pharmacologic
Bacharach
in patients
J Cardiol
Peterson
Maron
KM.
J
and
94:593-99
Dtsch
cardiomyopathy:
KM.
to
Dodge
left
hemodynamics
volumes
administration.
(abstract).
systolic
hypertrophic
Keller
approach
therapy:
angle
ofleft
CE,
JH.
BJ, Kent
10 VanTrigt
P, Olsen
CO. Pellom
JS, et al. The effect ofverapamil
left
17
60:1201-07
JR, et al. Long-term
lar diastolic
KM.
cardiomyopathy
Maron
approach
Rackley
myocardial
Seides
Patterns
HT The use ofsingle
calculation
determining
Calciumantagonistische
of hypertrophic
Rosing
16
18
hypertrophic
cardiomyopathy:
II. Effects
and symptomatic
status.
Circulation
1979;
9 Bonow
Condit
ventricular
cardiomyopathv:
JR,
Kent
Kent
Kardiomyopathie.
JS,
a wide
of 125 patients.
H, Dodge
SE.
hypertrophy
1968; 75:325-34
ventricular
MV,
with
WD,
Epstein
ventricular
29:666-71
patients
M.
a new
Circulation
DR.
Allen
JS,
of left
study
15 SandIer
42:35-42
Borer
therapy:
oflong-term
KM.
64:787-96
Bussman
1979;
DR,
therapy:
in
Keler
of hypertrophic
8 Rosing
(ab-
cardiomy-
Green
obstructive
KM.
RO, et al: Verapamil
macologic
treatment
ographic
101:1284-87
J
Condit
Kent
of left
on left
1981;
hypertrophic
Kent
IC,
SL,
hypertrophobstruktiver
bei
Wochenschr
6 Rosing
filling
R,
cardiomyopathy:
64:IV-35
of verapamil
Hopf
and
in hypertrophic
1981;
Circulation
volume
symptoms
measurement
Bacharach
diastolic
cardiomyopathy.
Med
DR.
of distribution
for the
Lipson
ofverapamil
Circulation
Allen
mechanisms
improved
BJ, Gottdiener
LC,
1981
DR,
probe
opathy
Kaltenbach
and
Rosing
effect
Lipson
in ventricular
64:IV-11,
Scintillation
function:
KM.
cardiomyopathy:
gradient
1981;
al
Kent
changes
subvalvular
function
4
DR.
in hypertrophic
Circulation
diastolic
3
Rosing
et al. Verapamil-indiiced
diastolic
for
HG,
14 Maron
for
Progress
1981;
affect
the
in
175-85
diastolic
42:171-80
Jr.
Ventricular
function.
myocardial
In: Grossman
angiography.
W, ed,
Philadelphia:
Lea
and
1980; 245-67
SE,
Rosing
serious
complications
opathy.
Circulation
DR.
Verapamil:
in patients
1981;
its
with
potential
for
hypertrophic
causing
cardiomy-
64:437-41
CHEST
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21369/ on 05/04/2017
I
84
I 1 I
JULY,
1983
57