Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
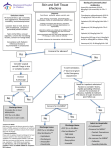
Skin and Soft Tissue Infections in the Inpatient Setting Definition and Epidemiology: Skin and soft tissue infections encompass a range of clinical diagnoses from furuncles and carbuncles to necrotizing fasciitis. They account for 17% of all clinic visits and most often can be dealt with as an outpatient. As this module pertains mainly to the inpatient setting, the discussion below will focus on erysiplelas, cellulitis, abscess, and necrotizing fasciitis. Differential: Many skin disorders can appear to be bacterial in nature but are in fact other diseases. The differential of skin and soft tissue infections include insect bite hypersensitivity, allergic reactions, periodic fever syndromes and familial Mediterranean fever, fixed drug eruptions, pyoderma gangrenosum, erythema nodusum and reflex sympathetic dystrophy. Erysipelas Definition: Erysipelas is a soft tissue infection that involves the upper dermis. The location of infection differentiates it from cellulitis which involves the deeper dermis and subcutaneous fat. Presentation: It often presents with fever, chills, malaise followed by a warm, shiny bright red plaque. The lesion is well demarcated and is often present in the lower extremities. Work up and Treatment: Usually erysipelas can be treated as an outpatient. It is most commonly caused by Streptococcus pyogenes(group A β-hemolytic streptococcus) followed by other streptococci species. Less commonly, Stapylococcus aureus, Klebsiella and Yersinia can be the etiology of the infection. Penicillin is an appropriate antibiotic unless staph is suspected in which case a penicillinase resistant pencillin or first generation cephalosporin should be used. Cellulitis Definition: Cellulitis is inflammation and infection of loose connective tissue limited to the dermis and relative sparing of the epidermis. A break in the skin due to trauma, surgery, underlying skin lesions, lymphatic stasis, diabetes, and immunosuppression all increase the risk of developing such infection. Presentation: Cellulitis presents as warmth, edema, erythema, and tenderness of the involved tissue. The margins of infection are indistinct as it involves the dermis as opposed to the epidermis. Celluitis is common in the lower extremities and can start from fissures within the toes spaces. Secondary complications of cellulitis involve abscess formation, bacteremia, osteomyelitis, septic arthritis, thrombophlebitis, endocarditis and necrotizing fasciitis. Organisms: Cellulitis is most often caused by S. pyogenes and S. aureus. Less likely organisms include Streptococcus pneumoniae, group C and group G streptococci. Haemophilus influenzae was an important cause of cellulitis of the head and neck prior to widespread immunization. Other causes of cellulitis should be considered depending on the clinical scenario to help direct appropriate antibiotic treatment. Pasteurella multocida and Capnocytophaga canimorsus may be involved in cases associated with dog and cat bites. Vibrio species, especially Vibrio vulnificus are associated with salt water immersion, where as Aeromonas hydrophila is associated with fresh water exposure. Human bites commonly involve multiple organisms, but 80% contain strep species and in particular S. viridans. Staph, Haemophilus, Eikenlla corrodens, Fusobacterium species, Prevotella and Porphyromonas species have also been implicated. Work up: In general, diagnosis of cellulitis is made clinically. Blood cultures are negative in more than 95% of patients and should be reserved for those who are particularly ill. When cultures are obtained from the site of infection, only 25% lead to identification of the involved organism. Cultures can be obtained by aspiration or skin biopsy but these methods are invasive and should be reserved for cases in which an unusual organism is suspected or the diagnosis is in question. According to recommendations from adult infectious disease experts, if there are signs and symptoms of systemic toxicity, a CBC with differential, blood culture, creatinine, bicarbonate, CPK and CRP should be obtained. Treatment: Generally, cellulitis can be treated as an outpatient with a penicillinase resistant penicillin or first generation cephalosporin to cover both staph and strep. Given the increasing incidence of MRSA in the community, many physicians will use clindamycin or trimethoprim/sulfamethoxazole (TMP/SMX) as first line therapy. One should remember that first TMP/SMX does not treat group A strep which is an important cause of cellulitis and that second, cellulitis due to staph is more common if there is an underlying abscess or penetrating trauma. One recent study compared clindamycin, β lactams, and TMP/SMX in the treatment of nondrained, noncultured skin and soft tissue infections. They found that there was no difference in treatment failure between clindamycin and β lactams. However, the use of TMP/SMX was significantly associated with failure as well as history of induration or abscess. Reasons for admission include signs of systemic toxicity, no results after 24 to 48 hours of outpatient antibiotics, inability to tolerate oral medications or uncertainty regarding follow up. If a patient is particularly ill, vancomycin or linezolid should also be considered. Also, one should treat the underlying problem such as eczema, tinea and/or trauma. Finally, though often overlooked, immobilization and elevation can also help as they promote drainage of the inflammation. Abscess Definition: An abscess is a localized collection of pus resulting from the disintegration of tissue in the dermis and deeper skin tissues. The overlying epidermis is normal but the dermis contains inflammatory cells and broken down tissue. Presentation: Abscesses present as firm, tender, erythematous nodules that may be initially indurated but become fluctuant with time. Often there is a pustule present with a rim of erythematous tissue. Patients may also mistake the clinical symptoms for a “spider bite.” Generally, constitutional signs are absent unless the process is located in the deeper tissues or the infection enters the blood stream. Organisms: The most common etiology of an abscess is S. aureus followed by S. pyogenes, alpha hemolytic and nonhemolytic streptococci, Enterococcus, Enterobacter, E. coli and Pseudomonas. If the abscess is located in the perineal area, multiple species of facultative and anaerobic fecal organisms can be present. Work up/Treatment: Incision and drainage is the key to treatment. This can provide cultures for definitive identification of the involved organism(s) and it is also therapeutic. After I & D, simply covering the area with a dry dressing is the easiest and most effective way to treat the wound. Often, no antibiotics are necessary unless the patient is immunocomprimised, has multiple lesions or a very large lesion, has an underlying cellulitis, a high fever or is very young. Admission should be considered for those with large abscesses (>5cm) or signs of systemic toxicity. Depending on the clinical scenario, some patients may require drainage in the OR to allow for appropriate sedation and complete drainage. MRSA: MRSA deserves special consideration in the management of abscesses. MRSA was first described in the 1960s as a source of health care associated infections and then reported in healthy children without healthcare exposure in the 1980s. It became more widespread in the 1990s and is the predominant form of staph in some regions of the country. Outbreaks may occur among certain groups of people (inmates, teammates, etc) but the majority of infections occur in individuals that are not members of a particular group. MRSA more commonly affects children and young adults as well as minorities and those of low socioeconomic status. Though in the past, culture and testing of purulent abscess was not always routine, it is now necessary given the prevalence of MRSA. MRSA is resistant to β lactam antibiotics but often susceptible to clindamycin, doxycycline, clindamycin, TMP/SMX, fluoroquinolones, vancomycin and linezolid. There has been concern for rising resistance to clindamycin secondary to strains that are inducibly resistant to erythromycin. Patient education should be provided regarding clean hands, covering lesions, bathing regularly and not sharing personal items. Different decolonization regimens have been tried but are difficult to evaluate. Mupirocin ointment can eliminate nasal colonization in the short term and reduce recurrences of furuncles by 50% but there is concern about long term use leading to significant resistance. Necrotizing Fasciitis Definition: Necrotizing fasciitis is a subcutaneous infection that involves the deep layer of superficial fascia but spares the epidermis, deep fascia and muscle. Necrotizing fasciitis involves the death of tissue as opposed to cellulitis which simply involves inflammation. Presentation: Necrotizing fasciitis presents with acute onset of local swelling, erythema, tenderness and warmth. It is most often present in the extremities(more often lower), abdomen and perineal region. The risk of infection is increased in those who are immunocomprimised or have undergone surgery or have a break in the skin due to trauma, abrasion, laceration, or varicella skin infection. Constitutional signs including fever, pain, and toxicity are often out of proportion to cutaneous symptoms with cutaneous symptoms less severe than expected given the degree of underlying tissues destruction. It can be difficult to differentiate between necrotizing fasciitis and cellulitis. However symptoms that may be more indicative of fasciitis include severe and constant pain, bullae and skin necrosis, gas in the soft tissue, edema that extends beyond the erythema, cutaneous anesthesia, systemic toxicity and rapid spread. Necrotizing fasciitis also has a wooden hard sensation to the tissue. Organisms: Most organisms cannot cause the infection on their own. However, S. pyogenes may be the sole organism in necrotizing fasciitis is associated with fulminant infection and a high case fatality. Other bacteria that have been implicated include staph, Clostridium perfingens, Clostridium septicum, Pseudomonas, Vibrio species and fungal organisms. Work up/Treatment: Necrotizing fasciitis can be difficult to differentiate from cellulitis. MRI and CT can aid in delineating the extent and planes of involvement. However, imaging should not delay treatment which includes antibiotics, supportive care and most importantly surgical exploration. In surgery, the fascia and subcutaneous tissues are grey with brown exudates with no true pus. Antibiotic treatment should include penicillin as well as clindamycin and aminoglycosides. Clindamycin is important for its role in inhibiting protein synthesis of new bacterial necrotizing toxins.