Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Triclocarban wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Gastroenteritis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Onchocerciasis wikipedia , lookup
Sarcocystis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Schistosomiasis wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Hepatitis B wikipedia , lookup
Urinary tract infection wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Infection control wikipedia , lookup
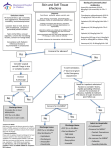
Skin and Soft Tissue Infections (SSTIs) Dr.Hisham Ahmed,M.D,MRCS.Eng Asst.Professor of General & Pediatric Surgery Background Skin and soft tissue infections (SSTIs), which include infections of skin, subcutaneous tissue, fascia, and muscle, encompass a wide spectrum of clinical presentations, ranging from simple cellulitis to rapidly progressive necrotizing fasciitis. Diagnosing the exact extent of the disease is critical for successful management of a patient of soft tissue infection classification Simple uncomplicated (mostly Gram +) cellulitis Folliculitis impetigo erysipelas simple abscess furuncles (boils) carbuncles • Complicated ( gram + & gram -) decubitus ulcers necrotizing fasciitis pyomyositis gas gangrene Causative pathogens Staphylococcus aureus (the most common pathogen) Streptococcus pyogenes Site-specific infections - Indigenous organisms (e.g., gram-negative bacilli in perianal abscess) Immunocompromised hosts and complicated SSTIs Multiple organisms or uncommon organisms (e.g., Pseudomonas aeruginosa, beta-hemolytic streptococci, Enterococcus) Cont. Polymicrobial necrotizing fasciitis - Mixed infection with both aerobes (e.g., streptococci, staphylococci, or aerobic gram-negative bacilli) and anaerobes (e.g., Peptostreptococcus, Bacteroides, or Clostridium) Monomicrobial necrotizing fasciitis: S pyogenes Predisposing factors Breach in the epidermis Dry and irritated skin Immunocompromised status - Malnutrition, hypoproteinemia, burns, diabetes mellitus, AIDS Chronic venous insufficiency Chronic lymphatic insufficiency Chronic neuropathy Laboratory tests Patients with uncomplicated SSTIs usually do not require any investigations and need not be hospitalized. However, patients with symptoms and signs of systemic toxicity, such as tachycardia and hypotension, should undergo the following tests: Blood culture and drug susceptibility Complete blood count (CBC) with differential Creatinine level Cont. Bicarbonate level Creatine phosphokinase level C-reactive protein level Additional investigations may be indicated, depending on the severity of systemic toxicity. Cellulitis Acute diffuse non-suppurative inflammation affecting epidermis and dermis Inflammation with little or no necrosis, edema Lymphatic involvement tense ill defined area showing criteria of inflammation. Lymphangitis & lymphadenitis Complications: Abscess and osteomyelitis Streptococcus pyogenes fibrinolysin & hyaluronidase enzymes facilitate spread of infection. Obesity Edema ◦ Venous insufficiency ◦ Lymphatic obstruction Fissured toe webs Inflammatory dermatoses – eczema Repeated cellulitis Subcutaneous injection Previous cutaneous damage All lead to breaches in the skin for organism invasion ◦ Maceration ◦ Fungal infection Saphenous venectomy Axillary node dissection for breast cancer Pelvic lymphadenectomy for malignancy in conjunction with radiotherapy. Liposuction Fate; Resolution Localization abscess formation Sloughing of overlying skin Spread Recurrent attacks lymphatic destruction Treatment ; Medical in the form of Antibiotics e.g. ampicillin, Vancomycin and Clindamycin for resistant cases suspecting MRSA Leg elevation Elastic stocking GIII Weight reduction Care of the skin esp. web space Impetigo Contagiosa & Erysipelas ◦ Etiology Caused by A-beta-hemolytic streptococci, S aureus or combination of these bacteria Spread through close contact Impetigo occurs most in children Erysipelas can also occur in the elderly ◦ Signs and Symptoms Mild itching and soreness followed by eruption of small vesicles and pustules that rupture and crust Generally develops in body folds that are subject to friction ◦ Management Cleansing and topical antibacterial agents Systemic antibiotics e.g. Ampecillin abscess Abscess is a localized collection of pus, Surrounded by a pyogenic membrane Staphylococcus aureus is the causative organism…coagulase enzyme……localization The route of infection either, direct, blood or lymphatic spread. Painful compressible mass that is red, warm to touch, and tender. Fate; Resolution Rupture Spread Chronic abscess formation Treatment Pre-suppurative stage Rest Elevation Warm packs NSAIDs Antibiotics • Suppurative stage Incision & Drainage under G.A using Hilton’s method What are the abscess that we do not wait for fluctuation? Hand infection Pulp space Palm space Tenosynovitis Parotid abscess Breast abscess Buttock abscess Peri-anal abscess Peri-nephric abscess Furunculosis (Boils) Etiology Infection of hair follicle that results in pustule formation Generally the result of a staph. Aureus infection ◦ Signs and Symptoms Pustule that becomes reddened and enlarged as well as hard from internal pressure Pain and tenderness increase with pressure Most will mature and rupture ◦ Management Care involves protection from additional irritation Referral to physician for antibiotics Keep athlete from contact with other team members while boil is draining Carbuncles ◦ Etiology Similar in terms of early stage development as furuncles ◦ Signs and Symptoms Larger and deeper than furuncle and has several openings in the skin May produce fever and elevation of WBC count Starts hard and red and over a few days emerges into a lesion that discharges yellowish pus ◦ Management Surgical drainage combined with the administration of antibiotics Warm compress is applied to promote circulation Folliculitis ◦ Etiology Inflammation of hair follicle Caused by noninfectious or infectious agents Moist warm environment and mechanical occlusion contribute to condition Psuedofolliculitis (PFB) ◦ Signs and Symptoms Redness around follicle that is followed by development of papule or pustule at the hair follicle Followed by development of crust that sloughs off with the hair Deeper infection may cause scarring and alopecia in that area ◦ Management Management is much like impetigo Moist heat is used to increase circulation Antibiotics can also be used depending on the condition Necrotizing Fasciitis “Flesh Eating Strep” Streptococcus pyogenes (Group A Strep) Tissue digesting enzymes ◦ Hyaluronidase ◦ Streptokinase ◦ Streptolysins Rapidly spreading cellulitis may lead to loss of limb Necrotizing Fasciitis Disease starts as localized infection • Pain in area, flu-like symptoms Invasive and spreading May lead to toxic shock (drop in blood pressure) Incidence 1-20/100,000 30-70% mortality Surgical removal, antibiotics • Gas Gangrene ◦ Signs and symptoms Blackening of infected muscle and skin Presence of gas bubbles ◦ Pathogens and virulence factors Caused by several Clostridium species Bacterial endospores survive harsh conditions Vegetative cells secrete endotoxins Gas Gangrene ◦ Pathogenesis and epidemiology Traumatic event must introduce endospores into dead tissue Mortality rate exceeds 40% ◦ Diagnosis, treatment, and prevention Appearance is usually diagnostic Rapid treatment is crucial Surgical removal of dead tissue Administration of antitoxin and penicillin Prevent with proper cleaning of wounds Thank you