Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
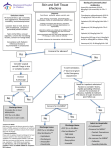
Skin and Soft Tissue Infections Cellulitis Impetigo Erysipelas Abscess Animal bite Human bite Surgical site infection Necrotizing fasciitis Skin and Soft Tissue Infections Increasing ER visits and hospitalizations 29% increase in admissions, 2000 to 2004 Primarily in age <65 Presume secondary to community MRSA 50% cellulitis and cutaneous abscesses Estimated $10 billion SSTI 2010 IDSA Guidelines MUSC Antibiotic Stewardship & Anti-Infective Subcommittee “Practice guidelines are systematically developed statements to assist practitioners and patients in making decisions about appropriate health care for specific clinical circumstances.” Guidelines Reduce emergence of resistant organisms Reduce hospital days Reduce costs: Blood cultures Consultations Imaging Hospital days 2011-Implementation of treatment guidelines Decreased use of blood cx Decreased advanced imaging Decreased consultations Shorter durations of therapy Decreased use of anti-pseudomonal Decreased use of broader spectrum abx Decreased costs No change in adverse outcomes Inpatient Hospitalization Systemic illness HR >100 and Temp >38oC or <36oC and Systolic bp <90 or decrease of 20 mmHg < baseline CRP>13 Marked left shift Elevated creatinine Low serum bicarbonate CPK 2 x the upper limit of normal Inpatient Hospitalization Abnormally rapid progression of cellulitis Worsening infection despite appropriate antibiotics Tissue necrosis Severe pain Altered mental status Respiratory, renal or hepatic failure Co-morbidities: immune compromise, neutropenia, asplenia, preexisting edema, cirrhosis, cardiac failure, renal insufficiency Objectives Classification Skin anatomy Infection caused By SA Infection caused By Streptococcus Necrotizing fascitis Bites ( human and animal) MSSA/MRSA updates what’s new in therapy? CID,2005, 41:1373-1406 What is Localized skin infection? Localized SSSIs include lesions such as furuncles, carbuncles, and abscesses, which would generally be treated by incision and debridement with drainage. When to consider it complicated ? Surrounding cellulitis, immunocompromised, or the presence of potentially infectable prostheses, such as cardiac valves, orthopedic devises or vascular grafts, mandates antibiotic use and might well mean that the infection would be classed as complicated In particular, there are a number of underlying comorbidities that should be sought and excluded as being particularly relevant to the patient with an SSSI. Diabetes Vascular insufficiency in the area of the infection Chronic renal or hepatic disease Potentially infectable prostheses Immunosuppression Debilitation or advanced age Recent antimicrobial therapy Recent surgery; and Recent hospitalization cSSSI Definition Abscess Cellulitis Ulcer Skin/skin structure infections that: • Involve deep, soft tissue • Require surgical intervention • Are associated with significant underlying disease that complicate the response to treatment 36 Epidemiology and Microbiology Colonized with Gram-positive organisms : Staphylococcus epidermidis; Corynebacterium spp; Micrococcus spp; Diphtheroids; Propionibacterium spp; and Anaerobic cocci While the moist intertriginous areas have a wider spectrum of colonizations: Escherichia coli; Proteus spp Enterobacter spp; and Other organism (including fungi) Anatomy of the skin Clinical presentations of SSTIs Surgical site infection Necrotising SSTI Cellulitis Skin and soft tissue infections Diabetic foot infection Infected wound Abscess Infected ulcer ~0.1% of adult population requires hospital treatment for SSTIs each year1 SSTIs may become complicated if require hospitalisation, surgery, involve deeper tissues, co-morbidities or systemic symptoms 1. Eron LJ, et al. J Antimicrob Chemother 2003; 52 Suppl1:i3–17. Obtain Careful History Immune status Geographic locale Travel history Recent trauma or surgery Previous antimicrobial therapy Lifestyle - occupation Hobbies Animal exposure Bite exposure Cultures Blood cultures positive <5% Needle aspiration 5-40% Punch biopsy 20-30% Blood Cultures HR >100 , Temp >38oC and <36oC, Sys <90mmHg Lymphedema Immune compromise/neutropenia/malignancy Pain out of proportion to exam Infected mouth or eyes Unresponsive to initial antibiotics Water-associated cellulitis Diabetes Recurrent or persistent cellulitis Concern for a cluster or outbreak Needle Aspiration or Skin Biopsy HR >100 , Temp >38oC and <36oC, Sys<90mmHg CRP>13 Marked left shift Elevated creatinine Low serum bicarb CPK 2 x upper limit of normal Immune compromise/neutropenia/malignancy Diabetes Animal or human bite wounds Broaden Antibiotics If no improvement in systemic signs in 48 hours If no improvement in skin in 72 hours As antibiotics kill organisms, released toxins may cause a worsening of skin findings in first 48 hours Deescalation Acute skin findings resolving Afebrile No signs of systemic illness Should see systemic signs improvement by 48 hours Should see skin improvement 3-5 days by at the latest What are the four main organisms? FIRST :S. aureus Is the commonest Two potent and clinically relevant exotoxins from S. aureus are the enterotoxins (responsible for food poisoning) and toxic shock syndrome toxin (TSST-1) SECOND :Group A streptococci ( GAS) (S. pyogenes), much like S. aureus can produce a variety of virulence factors. Group A streptococci secrete an array of soluble exotoxins some of which are extremely potent causing systemic toxicity known as streptococcal toxic shock syndrome 9STSS) and necrotizing fascitis. THIRD :Clostridium perfringens is the most frequently isolated, although isolates of C. septicum, C. histolyticum, C. bifermentans, and C. novyii can be equally pathogenics. Cellulitis 65% relative increase since 1999 600,000 admissions annually Risk Factors for Cellulitis Obesity Edema Venous insufficiency Lymphatic obstruction Fissured toe webs Maceration Fungal infection Inflammatory dermatoses – eczema Repeated cellulitis Subcutaneous injection or illegal drugs Previous cutaneous damage All lead to breaches in the skin for organism invasion Post-Surgical Risk Factors Saphenous venectomy Axillary node dissection for breast cancer Gyn malignancy surgery with lymph node dissection *** in conjuction with XRT Liposuction Non-Purulent Cellulitis INTACT SKIN No purulent drainage, no exudate, no associated abscess Beta hemolytic streptococci Antibiotic: Cefazolin Documented anaphylactic cephalosporin allergy - Vancomycin Non-Purulent Cellulitis Deescalation: Cephalexin Beta-lactam anaphylaxis - clindamycin 5 days of treatment Purulent/Complicated Cellulitis BROKEN SKIN Purulent drainage Exudate Absence of a drainable abscess Purulent/Complicated Cellulitis Deescalation: Trimethoprim/sulfamethoxazole + cephalexin Beta lactam anaphylaxis – clindamycin Sulfa allergy – tetracycline or doxycycline If sulfa and beta lactam allergies - linezolid 5 days of treatment Empiric SSTI algorithm *This algorithm does NOT include: surgical site infections, diabetic foot ulcers, decubitus ulcers, insect, animal or human bites, or gangrene **Please see order form for guidance (including renal dosing adjustments) If cephalosporin allergic: Vancomycin can be substituted for cefazolin 1 The preferred method of treatment is I&D Clinical Pearl: Treatment should continue for 48 hours prior to determination of clinical failure; SSTIs often appear worse during initial treatment period Antibiotic De-escalation Criteria 1.Culture susceptibilities 2.Clinical response 1. Clinically stable 2. Decreased erythema 3. Decreased edema 4. Decreased warmth 5. Resolving leukocytosis 6. Afebrile Total course of antibiotics is 5 days (i.e. 2 days of IV cefazolin + 3 days of PO cephalexin) Note: Renal dose adjustments are required for patients with CrCL less than 30 mL/min If sulfa allergic: Either tetracycline or doxycycline can be substituted to replace TMP/SMX If beta-lactam anaphylaxis: Clindamycin (non-severe infection) can be substituted to replace cephalexin, or linezolid can be substituted to replace both TMP/SMX and cephalexin Secondary Treatment of Cellulitis Elevation of affected leg Compression stockings Treat underlying tinea pedis, eczema, trauma Keep skin well hydrated Abscess Abscess ALWAYS, ALWAYS Incision and drainage Drainable Abscess <3cm Incision and drainage No blood cultures No aspirate culture NO ANTIBIOTICS Abscess –When to Add Antibiotics Drainable abscess >3cm Undrainable Multiple sites of infection Rapid progression in presence of cellulitis Systemic illness (fever, hypotension, tachycardia) Immune compromise Elderly Difficult to drain area (hand, face, genitalia) Lack of response to incision and drainage Septic phlebitis - multiple lesions Gangrene Bacterial pathogens as causative agents of SSTIs in hospitalised patients Relative incidence (%) 35 30 Enterococcus spp 25 S. aureus 20 Coagulase-negative Staphylococci E. coli 15 10 P. aeruginosa 5 0 USA France Germany Italy Spain Data from clinical laboratories participating in The Surveillance Network (TSN), 2001. Jones M, et al. Int J Antimicrob Agents 2003; 22:406–419. What sort of skin structure infections are usually caused by staphylococci? It is often helpful to remember that localized SSSIs above the belt are more likely to be caused by S. aureus than those below the belt, which are more likely to be associated with mixed flora Furunculosis Cellulitis Abscesses Staphylococcal Toxic Shock Syndrome STSS It occurs in menstruating young females, but, at present, most staphylococcal toxic shock syndrome results from skin abscesses, intravascular catheter infections, and S. aureus pneumonia complicating influenza. Provable cases =microbiological criteria +4 of the five clinical criteria. Confirmed cases =microbiological criteria + all five of the clinical criteria. Diagnostic Criteria for the Diagnosis of Staphylococcal Toxic Shock Syndrome Clinical Criteria Fever 38.9oC Rash Diffuse macular erythroderma rash Desquamation Desquamation of rash 1-2 weeks after onset of illness, especially on palms and soles Hypotension Systolic blood pressure 90 mmHg (for adults), <5th percentile by age for children under 16 years Orthostatic drop in diastolic blood pressure mmHg from lying to sitting, orthostatic syncope or orthostatic dizziness. Multiple organ failure At least three of: •Gastrointestinal involvement – vomiting or diarrhea at onset, hyperemic mucosa •Muscular involvement – severe myalgia or creatinine phosphokinase at least twice the upper limit of normal • renal involvement – urea at least twice the upper limit of normal, or urinary sediment with pyuria ( 5 leukocytes per hpf) in the absence of urinary tract infection •Hepatic involvement – total bilirubin, alanine aminotransferase, or aspartate aminotransferase twice the upper limit of normal •Hematological involvement – platelets <100 x 109/liter •Neurological involvement – disorientation or reduced consciousness without focal neurological signs when fever and hypotension are absent •Mucous membrane involvement – vaginal, oropharyngeal, or conjuctival hyperemia Microbiological Criteria (if Specimens Obtained) Negative Results Blood culture, throat culture, cerebrospinal fluid culture. Anti-MRSA (other than vancomycin) Treatment failures with clindamycin have been reported Clindamycin resistance is due to methylation of the 235 portion of the ribosomal target preventing the attachment of clindamycin to its target Detection of inducible MLSb resistance in staphylococci can easily be performed in the microbiology laboratory by use of the D-test Anti-MRSA (other than vancomycin) The overall cure rates with TMP-SMZ and vancomycin were 85% and 98% (p=0.014. It is interesting to note that all infections (endocarditis, SSSIs, and others) due to MRSA were cured. Rifampin should not be used as single agent Against S. aureus both doxycycline and minocycline are more potent than tetracycline and a recent study indicated that 95% or more of all MRSA and MSSA isolates were susceptible to doxycyline. What infections are caused by sterptococci? Impetigo Cellulitis Erysipelas STSS Necrotizing fascitis Streptococcal Cellulitis Erysipelas is a type of cellulitis most commonly caused by group A streptococci, although in rare cases other types of streptococci or S. aureus are implicated. Erysipelas involves more superficial layers of the skin than cellulitis which is a deeper infection. There is prominent involvement of the lymphatic vessels. The more superficial nature of erysipelas accounts for its predominant clinical feature, that of an area of inflammation that is raised above the surrounding normal skin and has an edematous, indurated appearance. Vessels and lymphoedema Diagnostic Criteria for the Diagnosis of Streptococcal Toxic Shock Syndrome Clinical Criteria Hypotension Multiple organ failure Clinical Criteria Systolic blood pressure 90 mmHg (for adults), < 5th percentile by age for children under 16 years At least two of: •Renal involvement – creatinine mol/liter for adults, more than twice the upper limit of normal by age for children; in pre-existing renal disease, more than twice the baseline level •Hematological involvement – platelets <100x109/liter or disseminated intravascular coagulation •Hepatic involvement – total bilirubin, alanine aminotransferase or aspartate aminotransferace twice the upper limit of normal for the patient’s age: in preexisting hepatic disease, more than twice the baseline level •Respiratory involvement – acute respiratory distress syndrome •Rash – generalized erythematous macular rash, which may desquamate •Soft-tissue necrosis, including necrotizing fasciitis or myositis, or gangrene Microbiological Criteria Isolation of group A streptococci Necrotizing Fascitis Necrotizing fascitis is a fulminating inflammation of the fascia that results in thrombosis of the subcutaneous blood vessels and necrosis of the underlying tissue Necrotizing fascitis itself is generally divided into two broad Type I, caused by mixed aerobic/anaerobic bacteria, including enterococci and non-group A streptococci (usually C or G); and Type 2, caused by group A streptococci, either alone or in combination with other organisms What are the Clinical Features of Necrotizing Fasciitis? The most common site of infection is the distal lower limb, although fascial extension up the leg is common. The progression is often alarmingly rapid from a silent or apparently minor process to a fulminant condition with clinical features of systemic toxicity, extensive destruction with threat to the affected limb, and even imminent death. The first clue may be unexplained and rapidly worsening pain By the time the bullae have appeared, there is usually already extensive necrosis. How to diagnose Necrotizing Fascitis? Ncrotizing Facitis is LIMB + LIFE threatening Immediate extensive surgical debridement must be done ASAP CLINDAMYCIN must be give , it also has antitoxin action Clostridial Infections Clostridia are large, anaerobic Gram- positive, spore-forming bacilli. Clostridial infection can cause myonecrosis, or gas gangrene, which can be divided into three major groups Post-traumatic; post-operative or non-traumatic; and spontaneous Infectious Gangren and gangrenous cellulitis Clostridial Infections Clostridial myonecrosis is often associated with a traumatic event It can also develop in pre-existing wounds or infections such as skin ulcers and rhinocerebral or orbital mucormycosis. C. perfringens is the most frequent cause of clostridial myonecrosis but less frequent causes include C. septicum, C. novyii, C. histolyticum, and C. sordelli.ws Animal Bites Animal Bites Pasteurella – mc organism Antibiotics: Ampicillin/sulbactam Piperacillin/tazobactan Cefoxitin Meropenem Ertapenem (restricted to ID and Surgery) Tetanus toxoid (if not up to date) Human Bites Human Bite Antibiotics: Ampicillin/sulbactam Meropenem Ertapenem (restricted to ID and Surgery) Tetanus toxoid (if not up to date) Closed fist*** Antibiotics: Cefoxitin Ampicillin/sulbactam Ertapenem(restricted to ID and Surgery) Tetanus toxoid (if not up to date) Hand surgery consult*** Human Bites Deescalation: Amoxicillin/clavulanate Moxifloxacin + clindamycin Trimethoprim/sulfamethoxazole + metronidazole Treatment duration: Discontinue abx 3 days after acute inflammation disappears Usually 5-10 days of treatment if no joint or tendon involvement Surgical Site Infection Surgical Site Infection Pain, swelling, erythema, purulent drainage Usually have no clinical manifestations for at least 5 days after operation Most resolve without antibiotics Open all incisions that appear infected >48 hours after surgery No antibiotics if temperature <38.5oC and HR <100 bpm Surgical Site Infection If temperature >38.5oC or HR >100 bpm: Trunk, head, neck, extremity Cefazolin Clindamycin Vancomycin if MRSA is suspected Perineum, gi tract, female gu tract Cefotetan Ampicillin/sulbactam Ceftriaxone + metronidazole or clindamycin Fluoroquinolone + clindamycin Treatment duration: Usually 24-48 hours or for 3 days after acute inflammation resolves Neutropenia and SSTI’s Neutropenic Patients with SSTI ALWAYS blood CULTURES Initial infection - <7 days neutropenia Antibiotics Carbapenems Cefepime Ceftazidine Piperacillin/tazobactam PLUS Vancomycin Linezolid (restricted to ID) Daptomycin (restricted to ID) (discontinue if culture negative after 72-96 hours) Neutropenic Patients with Subsequent infection- >7days neutropenia (fungi, viruses, atypical bacteria) SSTI Treatment: Amphotericin B Micafungin (may require higher dose and ID consult) Voriconazole (restricted to ID, Heme/Onc, Critical Care, Pulmonary, and Transplant) PLUS Carbapenems Cefepime Ceftazidine Piperacillin/tazobactam PLUS Vancomycin Linezolid (restricted to ID) Daptomycin (restricted to ID) (discontinue if culture negative after 72-96 hours) Neutropenic Patients with SSTI Deescalation: Ciprofloxacin and amoxicillin/clavulanate Treatment duration: At least 7 days Vascular-Access Devices in Neutropenia Device predisposes to SSTI 66% Gram positive Entry site infection Antibiotics Tunnel infection and vascular port-pocket infection Device removal and antibiotics Diabetic Foot Ulcers Diabetic Foot Ulcers Not all diabetic foot ulcers are infected. Infection if at least 2 present: Purulent secretions Redness Warmth Swelling/induration Pain/tenderness Diabetic Foot Ulcers Common, complex, costly Largest number of diabetes-related hospital bed days Most common proximate, non-traumatic cause of amputations MRSA Risk Factors Recent hospitalization last 90 days Residence in long term care facility Antibiotics last 90 days Injection drug use Hemo- or peritoneal dialysis Incarceration last 90 days Home infusion therapy History of MRSA colonization Immunosupressive state/medications Wound care in past 30 days Pseudomonas Risk factors ICU stay in last 90 days Immunosuppressive state/medications Immunosuppressive states includes: HIV, solid organ transplants, BMT Immunosuppressive medications includes: Rejection medications, >20mg/d prednisone x2w Mild Diabetic Foot Ulcer Cellulitis or erythema extends <2cm around ulcer, infection limited to skin – no systemic indications Obtain foot xray – screen for osteomyelitis Antibiotics: No MRSA risk: Cephalexin Amoxicillin/clavulanate MRSA risk: Trimethoprim/sulfamethoxazole Doxycycline Treatment duration Usually 1-2 weeks treatment (can be as long as 4 weeks) Moderate Diabetic Foot Ulcers Erythema extends >2cm around ulcer or signs of abscess, osteomyelitis, septic arthritis, fasciitis – no systemic signs Foot x-ray Culture wound Wound care Assess need for debridement general surgery CRP ESR Bone biopsy for culture MRI if ESR and CRP elevated ID consult if osteomyelitis present Severe Diabetic Foot Ulcers Erythema extends >2cm around ulcer and signs of systemic infection(hypotension, hyperthermia, tachycardia) Foot xray Culture wound Blood cultures Wound care Assess need for debridement general surgery CRP ESR Consider MRI if suspect abscess or uncertain if osteomyelitis or if the ESR and CRP Bone biopsy ID consult if osteomyelitis Secondary Treatment of Diabetic Foot Ulcers Wound care Debridement Glycemic control Evaluate vascular status