Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Artificial heart valve wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Aortic stenosis wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
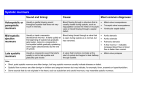
L. Mahmoudieh MD General : 1. 2. 3. 4. 5. 6. General appearance Skin Head and Neck Chest Abdomen Extremities Cardiovascular Examination GENERAL APPEARANCE : Any examination begins with an assessment of the general appearance of the patient : - Is the patient in pain or resting quietly, dyspneic or diaphoretic? - Does the patient choose to avoid certain body positions to reduce or eliminate pain, as might be the case with suspected acute pericarditis? -Are there clues indicating that dyspnea may have a pulmonary cause, such as a barrel chest deformity with an increased anterior –posterior diameter,tachypnea, and pursed-lip breathing? A chronically ill-appearing emaciated patient may suggest the presence of longstanding heart failure or another systemic disorder, such as a malignancy. Height and weight should be measured routinely, and body mass index should be calculated. SKIN : Cyanosis : - Central : Central cyanosis is evident when systemic arterial concentration of deoxygenated hemoglobin (Hb) in the blood exceeds 5 mg/dL. - Peripheral(acrocyanosis) : Is usually related to reduced extremity blood flow due to small vessel constriction, as seen in patients with severe heart failure, shock, or peripheral vascular disease; it can be aggravated by the use of adrenergic β-blockers with unopposed α-mediated constriction. - Differential : Refers to isolated cyanosis affecting the lower but not the upper extremities in a patient with a large patent ductus arteriosus (PDA)and secondary pulmonary hypertension with right -to-left to shunting at the great vessel level. Peripheral cyanosis Central cyanosis Differential cyanosis Cont. Jaundice, which may be visible first in the sclerae, has a broad differential diagnosis but in the appropriate setting can be consistent with advanced right heart failure and congestive hepatomegaly or late-term "cardiac cirrhosis.“ HEAD AND NECK : A high-arched palate is a feature of Marfan syndrome and other connective tissue disease syndromes. Many patients with congenital heart disease have associated hypertelorism, low-set ears, or micrognathia. The funduscopic examination is an often underutilized method by which to assess the microvasculature, especially among patients with established atherosclerosis, hypertension, or diabetes mellitus. The finding of an elevated JVP implies a cardiovascular etiology. CHEST : Midline sternotomy or infraclavicular scars at the site of pacemaker/defibrillator generator implantation should not be overlooked. Obstructive lung disease is suggested by a barrel chest deformity, especially with tachypnea, and use of accessory muscles. ABDOMEN : In some patients with advanced obstructive lung disease, the point of maximal cardiac impulse may be in the epigastrium. The liver is frequently enlarged and tender in patients with chronic heart failure. Splenomegaly may be a feature of infective endocarditis . Ascites is a nonspecific finding but may be present with advanced chronic right heart failure. Cont. In nonobese patients, the aorta typically is palpated between the epigastrium and the umbilicus. The sensitivity of palpation for the detection of an abdominal aortic aneurysm (pulsatile and expansile mass) decreases as a function of body size. Because palpation alone is not sufficiently accurate to establish this diagnosis, a screening ultrasound examination is advised. The presence of an arterial bruit over the abdomen suggests high-grade atherosclerotic disease . EXTREMITIES : The temperature and color of the extremities, the presence of clubbing can be surmised quickly during the examination. Clubbing implies the presence of central right to-left shunting , although it has also been described in patients with endocarditis and etc. The Janeway lesions are nontender, slightly raised hemorrhages on the palms and soles, whereas Osler's nodes are tender, raised nodules on the pads of the fingers or toes. Splinter hemorrhages are classically identified as linear petechiae in the midposition of the nail bed and are suggestive of ENDOCARDITIS . Splinter hemorrhage Osler's nodes Janeway lesions Cont. Lower extremity or presacral edema in the setting of an elevated JVP defines volume overload and may be a feature of chronic heart failure or constrictive pericarditis. Lower extremity edema in the absence of jugular venous hypertension may be due to lymphatic or venous obstruction or, more commonly, to venous insufficiency, as further suggested by the appearance of varicosities, venous ulcers (typically medial in location), and brownish cutaneous discoloration from hemosiderin deposition(eburnation). Muscular atrophy,shiny skin or the absence of hair along an extremity is consistent with severe arterial insufficiency . Cardiovascular Examination JUGULAR VENOUS PRESSURE : Jugular venous pressure is the single most important bedside measurement from which to estimate the volume overload. The internal jugular vein is preferred because the external jugular vein is valved and not directly in line with the superior vena cava and right atrium. Venous pressure traditionally has been measured as the vertical distance between the top of the jugular venous pulsation and the sternal inflection point (angle of Louis). A distance >4.5 cm at 30° elevation is considered abnormal. Venous pulsations above clavicle in the sitting position are clearly abnormal, as the distance between the clavicle and the right atrium is at least 10 cm. Elevated jugular venous pressure indicates increased right atrial pressure which can be caused by various pathologic conditions such as : 1.fluid overload 2. right ventricular failure 3. restriction of right atrial and right ventricular filling (eg, constrictive pericarditis) 4. superior vena cava obstruction Kussmaul's sign is defined by either a rise or a lack of fall of the JVP with inspiration and is classically associated with : constrictive pericarditis Although it has been reported in patients with : 1.restrictive cardiomyopathy 2.massive pulmonary embolism 3.right ventricular infarction ABDOMINOJUGULAR REFLEX(HEPATOJUGULAR REFLUX) : It is elicited with firm and consistent pressure over the upper portion of the abdomen, preferably over the right upper quadrant, for at least 10 s. A positive response is defined by a sustained rise of more than 3 cm in JVP for at least 15 s after release of the hand. In normal subjects this maneuver transiently increases jugular pressure by only approximately 1-3 cm. In patients with right ventricular failure, however, sustained elevation of venous pressure usually greater than 3 cm is observed during discontinued compression. ASSESSMENT OF BLOOD PRESSURE : Blood pressure is best measured in the seated position with the arm at the level of the heart, using an appropriately sized cuff, after 5 –10 min of relaxation. When it is measured in the supine position, the arm should be raised to bring it to the level of the mid-right atrium. The length and width of the blood pressure cuff bladder should be 80% and 40% of the arm's circumference, respectively. an inappropriately small cuff, resulting in marked overestimation of true blood pressure. an inappropriately large cuff, resulting in underestimation of true blood pressure. The cuff should be inflated to 30 mmHg above the expected systolic pressure and the pressure released at a rate of 2–3 mmHg/s. Cont. Blood pressure should be measured in both arms, and the difference should be less than 10 mmHg. A blood pressure differential that exceeds this threshold may be associated with : 1. atherosclerotic or inflammatory subclavian artery disease 2. aortic coarctation 3. aortic dissection Systolic leg pressures are usually as much as 20 mmHg higher than systolic arm pressures. Greater leg–arm pressure differences are seen in patients with : 1.extensive and calcified lower extremity peripheral arterial disease. Cont. The blood pressure measured in an office or hospital setting may not accurately reflect the pressure in other venues. "White coat hypertension" is defined by at least three separate clinic –base measurements >140/90 mmHg and at least two non-clinic-based measurements <140/90 mmHg in the absence of any evidence of target organ damage. Individuals with white coat hypertension may not benefit from drug therapy, although they may be more likely to develop sustained hypertension over time. Orthostatic hypotension is defined by a fall in systolic pressure >20 mmHg or in diastolic pressure >10 mmHg in response to assumption of the upright posture from a supine position within 3 min. It can be exacerbated by advanced age, dehydration and certain medications. PULSUS PARADOXUS :Systemic arterial pressure normally falls by less than 10 mmHg during inspiration, but this decline is not palpable at the peripheral pulse. Moderate to severe cardiac tamponade, and occasionally constrictive pericarditis, induce hemodynamic changes that enhance the inspiratory fall in systolic blood pressure. This exaggerated drop in systemic blood pressure during inspiration is termed pulsus paradoxus. To measure pulsus paradoxus, the cuff is deflated more slowly than usual. During deflation, the first Korotkoff sounds are audible only during expiration, but with further deflation, Korotkoff sounds are heard throughout the respiratory cycle. The difference between these two sounds quantifies pulsus paradoxus. CARDIAC EXAMINATION : Inspection Palpation Ascultation Inspection And Palpation :: Palpation of the heart begins with the patient in the supine position at 30° and can be enhanced by placing the patient in the left lateral decubitus position. The left ventricular apex beat may be visible in the midclavicular line at the fifth intercostal space in thin chested adults. Characteristics such as size and location should be noted. The normal apical impulse is less than 2 cm in diameter and moves quickly away from the fingers; it is better appreciated at end expiration, with the heart closer to the anterior chest wall. Cont. Enlargement of the left ventricular cavity is manifested by a leftward and downward displacement of an enlarged apex beat. In thin, tall patients and patients with advanced obstructive lung disease and flattened diaphragms, the cardiac impulse may be visible in the epigastrium. Systolic and diastolic thrills signify turbulent and high-velocity blood flow. Their locations help identify the origin of heart murmurs. Ascultation : Sounds : - S1 , S2 - systolic - diastolic Murmurs - systolic - diastolic - continuous S1 : Normal heart sound is prodused by valve closure. The first heart sound (S1) includes mitral and tricuspid valve closure. S1 is best heard with the diaphragm of the stethoscope. The intensity of S1 is normally maximal over the cardiac apex. S2 : Aortic and pulmonic valve closure constitutes the second heart sound (S2). The two components of S2 are best heard with the diaphragm of the stethoscope and over the left second interspace close to the sternal border. S2 sound may be splitted normaly or pathologically : With normal or physiologic splitting, the A2–P2 interval increases with inspiration and narrows during expiration. This physiologic interval will widen with right bundle branch block because of the further delay in pulmonic valve closure and in patients with severe MR because of the premature closure of the aortic valve. Reversed or paradoxical splitting refers to a pathologic delay in S2 aortic valve closure, such as that which occurs in patients with left bundle branch block,severe AS . The intensity of any heart sound, however, can be reduced by any process that increases the distance between the stethoscope and the responsible cardiac event, including : 1.Obstructive lung disease 2.Obesity 3.Pneumothorax 4.Pleural effusion 5.Pericardial effusion SYSTOLIC SOUNDS : 1.Ejection sound (AS , PS ) 2.Click ( MVP ) An ejection sound is a high-pitched early systolic sound . It is best heard with the diaphragm of the stethoscope. It usually is associated with a deformed but mobile aortic or pulmonic valve . ejection sounds are heard frequently in patients with mild to moderate valve stenosis; they may be absent in severe calcific stenosis, presumably due to the loss of valve mobility. Nonejection sounds (clicks), are related to mitral valve prolapse and may be followed by murmur. This click-murmur complex will move away from the first heart sound with maneuvers that increase ventricular preload, such as squatting. On standing, the click and murmur move closer to S1 . DIASTOLIC SOUNDS : 1. S3 , S4 2. opening snap ( MS, TS ) S3 And S4 : S3 and S4 are low-frequency diastolic sounds and are best heard with the bell of the stethoscope. S3 is just after S2 and S4 occurs prior to S1. S3 occurs as passive ventricular filling begins after actual relaxation is completed . S4 occurs after the P wave on the electrocardiogram and coincides with atrial systole and with the apical impulse. A left-sided S3 , S4 is best heard over the left ventricular (LV) apex. A right -sided S3, S4 is usually better heard over the lower left sternal border and becomes louder with inspiration. Cont. S3 can be heard in healthy young adults. However, it is usually abnormal in patients over the age of 40 years signifies heart failure . S4 can be heard in many healthy older adults without any other cardiac abnormality . An S4 is more common among patients with chronic left ventricular hypertrophy or active myocardial ischemia. An S4 is not present with atrial fibrillation. Opening Snap : The opening snap is a high-frequency, early diastolic sound associated with mitral or tricuspid valve opening. The opening snap results from rapid opening of the valve to its maximal open position. It is absent when the valve is heavily calcified and immobile. The opening snap is best heard with the diaphragm of the stethoscope The OS of mitral stenosis is heard best over medial to the cardiac apex. A tricuspid valve opening snap is heard best over the lower left sternal border. MURMURS : Heart murmurs result from audible vibrations that are caused by increased turbulence. MURMUR DESCRIPTION — The character of a murmur is described by a number of features, including : 1. intensity (grade) 2. frequency 3. timing 4. shape 5. location 6. radiation 7. response to bedside maneuvers Intensity —Six grades are used to classify the intensity of a murmur : grade 1 murmur is very soft and is heard only with great effort. grade 2 murmur is easily heard but not particularly loud. grade 3 murmur is loud but is not accompanied by a palpable thrill over the site of maximal intensity. grade 4 murmur is very loud and is accompanied by a thrill. grade 5 murmur is loud enough to be heard with only the edge of the stethoscope touching the chest. grade 6 murmur is loud enough to be heard with the stethoscope slightly off the chest. The frequency of the murmur determines the pitch, which may be high or low. Timing — The duration of a murmur is assessed by determining the length of systole or diastole that the murmur occupies : 1. systolic murmurs: - Midsystolic - Early systolic - Late systolic - Holosystolic (or pansystolic) 2. diastolic murmurs: - Early diastolic - Mid-diastolic 3. Continuous murmurs Shape — The time course of murmur intensity corresponds to the "shape" of a diagram of murmur intensity over time . crescendo - Crescendo (increasing) -Decrescendo (diminishing) plateau -Crescendo-decrescendo (increasing-decreasing or diamond shaped) -Plateau (unchanged in intensity) Diamond shape decrescendo Location — The location on the patient's chest where the murmur is loudest is typically described as apical or parasternal. Parasternal murmurs are further described by the intercostal space and right or left side of the sternum . Radiation Response to maneuvers SYSTOLIC MURMURS : A systolic murmur starts with or after S1 and terminates before or at S2. Systolic murmurs are recognized by identifying S1 and S2 and timing them with the carotid pulse. Systolic murmurs are further classified according to the time of onset and termination in systole: 1. A midsystolic murmur (MSM) begins after S1 and ends before A2 (left sided) or P2 (right sided) . Both S1 and S2 are audible 2.A holosystolic (or pansystolic) murmur starts with S1 and extends up to A2 (left sided) or P2 (right sided), obscuring both S1 and S2 3.An early systolic murmur obscures S1 and extends for a variable length in systole but does not extend up to S2 4.A late systolic murmur starts after S1 and obscures A2 (left sided) or P2 (right sided) Midsystolic murmurs: Mid-systolic murmurs begin at a short interval after S1 and end before S2. The intensity of the MSM increases (crescendo) during acceleration of blood flow early in systole; intensity declines (decrescendo) with the later deceleration of flow, resulting in a crescendo-decrescendo configuration. Includes : 1. Innocent 2. Increased semilunar blood flow 3. Aortic stenosis (supravalvular,subvalvular,valvular) 4. pulmonic stenosis (supravalvular,subvalvular,valvular,functional) 5.HOCM Innocent Murmur : These innocent or benign "flow" murmurs are typically midsystolic in timing. Innocent MSM can be heard in children and young adults that is best heard over the left second interspace. The "innocence" of an MSM should not depend upon the duration or intensity of the murmur, but on the absence of other abnormal findings. Increased semilunar blood flow : An MSM also occurs in the presence of normal valves when flow across the semilunar valve is significantly increased, as occurs in the following settings : - Anemia - pregnancy - thyrotoxicosis - fever Aortic stenosis : In valvular AS, the maximum intensity is appreciated over the right second interspace. A thrill may be palpable over the same area. The murmur radiates up into the neck and over both carotid arteries. It is often difficult to estimate the severity of the valve lesion on the basis of the physical examination findings. A aortic ejection sound at the onset of the murmur may be heard. S2 is paradoxically splitted in mod.-severe aortic stenosis. In severe cases S4 maybe heard. Pulmonic stenosis : The murmur of valvular pulmonic stenosis is best heard over the left second interspace. When the murmur is loud it radiates to the left side of the neck and is frequently accompanied by a palpable thrill. A pulmonic ejection sound at the onset of the murmur may be heard. S2 is widely split. HOCM : The obstructive form of hypertrophic cardiomyopathy (HOCM) is associated with a midsystolic murmur that is usually loudest along the lower left sternal border and without radiation to the carotid artery. The systolic murmur of HOCM usually can be distinguished from other causes on the basis of its response to bedside maneuvers, including valsalva, passive leg raising, and standing/squatting. Holosystolic Murmurs : Holosystolic murmurs are usually regurgitant murmurs and occur when blood flows from a chamber whose pressure throughout systole is higher than pressure in the chamber receiving the flow. There are three causes of holosystolic murmurs: - MR - TR - VSD MR : The holosystolic murmur of chronic MR is best heard at the apex and radiates to the axilla . it is usually plateau in configuration because of the wide difference between left ventricular and left atrial pressure throughout systole. TR : The holosystolic murmur of chronic TR is loudest at the left lower sternal border. Usually increases in intensity with inspiration . An enlarged and pulsatile liver maybe seen. VSD : The murmur of a VSD (without significant pulmonary hypertension)is holosystolic and loudest at the mid -left sternal border (third and fourth interspaces ), where a thrill is usually present. The character and timing of the systolic murmur change with large VSDs due to increased right ventricular and pulmonary artery pressure and an elevated pulmonary vascular resistance. Instead of being holosystolic, it becomes early systolic and the peak of the murmur occurs earlier. Thus, a loud holosystolic murmur in a patient with a VSD indicates favorable hemodynamics (eg, relatively normal right-sided pressures). Early Systolic Murmurs : Early systolic murmurs begin with S1, do not extend to S2, and generally have a decrescendo configuration. Early systolic murmurs may result from : - MR - TR - VSD. MR , TR : An equalization of left atrial and left ventricular pressure may occur, preventing the regurgitant flow during whole part of systole. Thus, the regurgitant murmur terminates before S2. Since the regurgitant flow is maximal at the beginning of systole and decreases with increasing left atrial pressure, a decrescendo configuration of this early systolic murmur is common VSD : In a large VSD with pulmonary hypertension, the murmur may be early systolic in timing, since the increasing right ventricular pressure during late systole decreases the left-to-right shunt. Findings of pulmonary hypertension are always present. Late Systolic Murmurs : A late systolic murmur starts after S1 and, if left-sided, extends to A2 . Mitral valve prolapse — Mitral valve prolapse is the most common cause of a late systolic murmur. It is best heard with the diaphragm of the stethoscope, over or just medial to the cardiac apex. It is usually preceded by click. DIASTOLIC MURMURS : A diastolic murmur starts with or after S2 and ends at or before S1. Diastolic murmurs are also classified according to the time of onset and termination of the murmur in diastole: 1. An early diastolic murmur starts with A2 (left sided) or P2 (right sided) and extends into diastole for a variable duration. 2. A mid-diastolic murmur starts after S2 and terminates before S1. Early Diastolic Murmurs : Early diastolic murmurs, most often due to aortic or pulmonary regurgitation, typically start at the time of semilunar valve closure and their onset coincides with S2. An aortic regurgitation murmur begins with A2; pulmonary regurgitation begins with P2. Includes : - AR - PR Aortic regurgitation : The murmur of aortic regurgitation is best heard with the diaphragm of the stethoscope.It could be best heard over the right second interspace, while the patient sits and leans forward with the breath held in full expiration . The radiation of an aortic regurgitation murmur is toward the cardiac apex . The configuration of the aortic regurgitation murmur is usually decrescendo because the magnitude of regurgitation progressively declines. Pulmonic regurgitation : The murmur has a decrescendo configuration like that of aortic regurgitation; differentiation is difficult if not impossible by auscultation alone. The murmur may increase in intensity during inspiration and can be more localized. It is best heard over the left second interspaces. Pathologic pulmonic regurgitation is most frequently a result of pulmonic hypertension. Mid-Diastolic Murmurs : Mid-diastolic murmurs result from turbulent flow across the atrioventricular valves during the rapid filling and atrial contracture phase because of mitral or tricuspid valve stenosis and an abnormal pattern of flow across these valves. Includes : - MS(Mitral stenosis) - TS ( tricuspid stenosis ) MS , TS : The mid-diastolic murmur of mitral stenosis is best heard with the bell of the stethoscope over the apex in the left lateral decubitus position . Tricuspid stenosis is best heard along the lower left sternal border. Presystolic accentuation is absent in patients with atrial fibrillation. It characteristically starts with an opening snap. CONTINUOUS MURMURS : Continuous murmurs are defined as murmurs that begin in systole and extend up to diastole without interruption. They do not necessarily need to occupy the total duration of systole and diastole. Their presence throughout the cardiac cycle implies a pressure gradient between two chambers or vessels during both systole and diastole. The continuous murmur associated with a patent ductus arteriosus is best heard at the upper left sternal border. Other cause of a continuous murmur include an arteriovenous fistula constructed to provide dialysis access. Effects of Physiologic Interventions on the Intensity of Heart Murmurs and Sounds : Respiration : Right-sided murmurs and sounds generally increase with inspiration, except for the PES.Left-sided murmurs and sounds are usually louder during expiration. Valsalva maneuver : Most murmurs decrease in length and intensity. Two exceptions are the systolic murmur of HOCM, which usually becomes much louder, and that of MVP, which becomes longer and often louder. Positional changes : With standing, most murmurs diminish, with two exceptions being the murmur of HOCM, which becomes louder, and that of MVP, which lengthens and often is intensified. With squatting,most murmurs become louder, but those of HOCM and MVP usually soften and may disappear. Passive leg raising usually produces the same results.The intensity of the murmurs associated with MR, VSD, and AR will increase in response to maneuvers that increase LV afterload, such as hand grip and vasopressors. PERICARDIAL DISEASE : A pericardial friction rub is nearly 100% specific for the diagnosis of acute pericarditis, though the sensitivity of this finding is not nearly as high, as the rub may come and go over the course of an acute illness or be very difficult to elicit. Classically, the three components are ventricular systole, rapid early diastolic filling, and late presystolic filling after atrial contraction in patients in sinus rhythm. It is necessary to listen to the heart in several positions. Additional clues may be present from the history and 12-lead electrocardiogram. The rub typically disappears as the volume of any pericardial effusion increases. www.practicalclinicalskill.com