Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
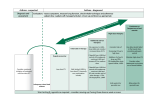
Salmeterol vs. Combination Therapy Replacement/Addition to the List Peer Feedback: “salmeterol/fluticasone or formoterol/budesonide or formoterol/mometasone - the danger with salmeterol alone if the risk of not coupling this drug with an inhaled corticosteroids, which has been associated with an increased risk of death.” “Symbicort (budesonide and formoterol) - I think you need a combination puffer for asthma, again for the compliance issues” Note: Second suggestion was made as an addition. Literature Review Question: Do combination medications have better compliance and outcomes then salmeterol independently? Literature Search: Cochrane Review (2013, 2012) eCPS - Respiratory Disorders: Asthma in Adults Pubmed – “salmeterol AND ((Salmeterol AND fluticasone) or (Formoterol AND budesonide) or (Formoterol AND mometasone)) AND (adherence OR compliance)”; “laba AND asthma AND adverse AND review” References taken from SMART 2011 Cochrane Review 2013 (Combined vs ICS) A total of 15 studies of good methodological quality met the inclusion criteria by randomly assigning 7814 participants with predominantly poorly reversible, severe COPD. Data were most plentiful for the FPS combination. Exacerbation rates were significantly reduced with combination therapies (rate ratio 0.87, 95% CI 0.80 to 0.94, 6 studies, N = 5601) compared with ICS alone. The mean exacerbation rate in the control (ICS) arms of the six included studies was 1.21 exacerbations per participant per year (range 0.88 to 1.60), and we would expect this to be reduced to a rate of 1.05 (95% CI 0.97 to 1.14) among those given combination therapy. Mortality was also lower with the combination (odds ratio (OR) 0.78, 95% CI 0.64 to 0.94, 12 studies, N = 7518) than with ICS alone, but this was heavily weighted by a three-year study of FPS. When this study was removed, no significant mortality difference was noted. The reduction in exacerbations did not translate into significantly reduced rates of hospitalisation due to COPD exacerbation (OR 0.93, 95% CI 0.80 to 1.07, 10 studies, N = 7060). Lung function data favoured combination treatment in the FPS, BDF and MF/F trials, but the improvement was small. Small improvements in health-related quality of life were measured on the St George’s Respiratory Questionnaire (SGRQ) with FPS or BDF compared with ICS, but this was well below the minimum clinically important difference. Adverse event profiles were similar between the two treatments arms, and rates of pneumonia when it was diagnosed by chest x-ray (CXR) were lower than those reported in earlier trials. Combination ICS and LABA offer some clinical benefits in COPD compared with ICS alone, especially for reduction in exacerbations. This review does not support the use of ICS alone when LABAs are available. Adverse events were not significantly different between treatments. Further long-term assessments using practical outcomes of current and new 24-hour LABAs will help determine their efficacy and safety. For robust comparisons as to their relative effects, long-term head-to-head comparisons are needed. Nannini, Luis Javier, et al. "Combined corticosteroid and long‐acting beta2‐agonist in one inhaler versus inhaled corticosteroids alone for chronic obstructive pulmonary disease." The Cochrane Library (2013). Safety of LABAs in Asthma (2012) Concerns about the safety of long-acting b2-agonist (LABA) therapy, has led to the appearance of multiple publications and recommendations. This review critically examines the available clinical evidence and safety requirements for LABA use. An appropriate clinical study would require an extremely large sample, making it impractical. Based mainly on the safety concerns arising from the SNS and SMART5 6 studies, some authors have suggested withdrawing LABA use for asthma therapy. However, these serious events have been infrequent and appeared when LABAs were used as monotherapy. By contrast, evidence from RCTs, meta-analysis of RCTs and observational studies, although limited by low statistical power, have indicated that the use of combination therapy (LABAs plus ICS) is associated with a decreased risk of serious asthma-related events. This is particularly true when the concomitant use of LABAs plus ICS can be reasonably assured (combined in a single inhaler). Therefore, the use of separate inhalers could result in periods of LABA monotherapy because of poor compliance with ICS use. Combination therapy could reduce asthma mortality by increasing the prescription and increasing compliance with ICS in the community. Furthermore, combination therapy should be applied to all patients with moderate to severe asthma, and not just paediatric and adolescent patients, as suggested by the FDA guidelines. Rodrigo, Gustavo J., and José A. Castro-Rodríguez. "Safety of long-acting β agonists for the treatment of asthma: clearing the air." Thorax 67.4 (2012): 342-349. Cochrane Review 2012 (Combined vs LABA) There was low quality evidence that exacerbation rates in people using LABA/ICS inhalers were lower in comparison to those with LABA alone, from nine studies which randomised 9921 participants (rate ratio 0.76; 95% CI 0.68 to 0.84). This corresponds to one exacerbation per person per year on LABA and 0.76 exacerbations per person per year on ICS/LABA. Our confidence in this effect was limited by statistical heterogeneity between the results of the studies (I2 = 68%) and a risk of bias from the high withdrawal rates across the studies. When analysed as the number of people experiencing one or more exacerbations over the course of the study, FPS lowered the odds of an exacerbation with an odds ratio (OR) of 0.83 (95% CI 0.70 to 0.98, 6 studies, 3357 participants). With a risk of an exacerbation of 47% in the LABA group over one year, 42% of people treated with LABA/ICS would be expected to experience an exacerbation. Concerns over the effect of reporting biases led us to downgrade the quality of evidence for this effect from high to moderate. There was no significant difference in the rate of hospitalisations (rate ratio 0.79; 95% CI 0.55 to 1.13, very low quality evidence due to risk of bias, statistical imprecision and inconsistency). There was no significant difference in mortality between people on combined inhalers and those on LABA, from 10 studies on 10,680 participants (OR 0.92; 95% CI 0.76 to 1.11, downgraded to moderate quality evidence due to statistical imprecision). Pneumonia occurred more commonly in people randomised to combined inhalers, from 12 studies with 11,076 participants (OR 1.55; 95% CI 1.20 to 2.01, moderate quality evidence due to risk of bias in relation to attrition) with an annual risk of around 3% on LABA alone compared to 4% on combination treatment. There were no significant differences between the results for either exacerbations or pneumonia from trials adding different doses or types of inhaled corticosteroid. ICS/LABA was more effective than LABA alone in improving health-related quality of life measured by the St George’s Respiratory Questionnaire (1.58 units lower with FPS; 2.69 units lower with BDF), dyspnoea (0.09 units lower with FPS), symptoms (0.07 units lower with BDF), rescue medication (0.38 puffs per day fewer with FPS, 0.33 puffs per day fewer with BDF), and forced expiratory volume in one second (FEV1) (70 mL higher with FPS, 50 mL higher with BDF). Candidiasis (OR 3.75) and upper respiratory infection (OR 1.32) occurred more frequently with FPS than SAL. We did not combine adverse event data relating to candidiasis for BDF studies as the results were very inconsistent. Nannini, Luis Javier, Toby J. Lasserson, and Phillippa Poole. "Combined corticosteroid and long‐acting beta2‐agonist in one inhaler versus long‐acting beta2‐agonists for chronic obstructive pulmonary disease." The Cochrane Library (2012). SMART (2011) Adherence to regular inhaled corticosteroid regimens is often poor, with only 15–20% of those people deemed to need such drugs actually using them regularly.8 The importance of using inhaled corticosteroids correctly needs to be discussed with patients by all those involved in the care of their asthma. Many patients will benefit more from the addition of a LABA than from increasing the corticosteroid dose,3,9 but there has also been a safety concern that LABAs used without concurrent inhaled corticosteroids in patients with asthma (an unlicensed use) may be associated with an increased risk of death from asthma.10 Consequently, both the Medicines and Healthcare products Regulatory Agency and the National Institute for Health and Clinical Excellence have recommended the use of combination inhalers to ensure that LABAs are only taken with an inhaled corticosteroid.3 Furthermore, the BTS/SIGN guideline now states that “in clinical practice…it is generally considered that combination inhalers aid compliance and also have the advantage of guaranteeing that the long-acting β2 agonist is not taken without the inhaled steroids”.3 However, the use of combination inhalers could limit flexibility of dosing when patients need to have their treatment stepped up or down. Reddel, Helen K., and Kwok Y. Yan. "Single maintenance and reliever therapy (SMART) of asthma." Thorax 66.1 (2011): 86-87. Regular use of ICS and Asthma Prevention (2002) The implications of our results for the treatment of asthma are important. This study strongly suggests that it is not the use—but the regular use—of inhaled corticosteroids that is essential to the effectiveness of these drugs. In addition, this effectiveness is sustained in the long term as long as the medications are taken regularly. This aspect of asthma management seems especially important in view of suggestions that compliance with inhaled corticosteroids appears to diminish over time on treatment.35 Our study indicates that few patients were actually benefiting from these medications. In our full cohort 22.3% of subjects had been dispensed inhaled corticosteroids sometime during the year before the index date but only 3.8% used them regularly, while in the hospitalised cohort 34.7% were prescribed inhaled corticosteroids but only 7.5% used them regularly. Thus, only 15– 20% of users deemed to need these drugs use them regularly and draw the full benefit. Recognising that this study spanned the period 1976–97 when the primary role of inhaled corticosteroids was less emphasised, it nevertheless seems important to assess and monitor these patterns of use. In addition, strategies such as targeting of patients at greatest risk for exacerbations, patient education on the importance of regular treatment, and reassurance concerning safety could help to ensure that the potential benefits suggested by clinical trials and observational studies can be translated into benefits at the clinical and population level. Suissa, S., P. Ernst, and A. Kezouh. "Regular use of inhaled corticosteroids and the long term prevention of hospitalisation for asthma." Thorax 57.10 (2002): 880-884. eCPS (2015) Class Beta2-adrenergic Agonists, longacting Drug salmeterol Serevent Corticosteroid/LA budesonide/formotero BA l fumarate dihydrate Combinations Symbicort Corticosteroid/LA fluticasone/salmeterol BA Combinations Advair pMDI, Advair Dose Adverse Effects Comments Cos ta Diskhaler 50 µg/blister:1 blister BID Diskus 50 µg/inhalation: 1 inhalation BID Nervousness, tremor, tachycardia, palpitations. Recommended only if confident patient will use prescribed inhaled corticosteroid as well. Combination LABA/corticosteroid product preferred. Not for reliever therapy. $$$ Maintenance therapy: DPI 100/6 µg or200/6 µg: 1–2 inhalations daily–BID; maximum 4 inhalations/day. May temporarily increase to 4 inhalations BID for worsening asthma Maintenance and reliever therapy: 1–2 inhalations BID or 2 inhalations once daily. Inhale 1 additional inhalation PRN in response to symptoms; if symptoms persist after a few min, an additional dose should be taken; maximum 6 inhalations on any single occasion; maximum 8 inhalations/day Sore mouth, sore throat, dysphonia, oral thrush (can be reduced by rinsing mouth or using spacer). Nervousness, tremor, tachycardia, palpitations. Bone densitometry is suggested in patients who require high doses or have risk factors for osteoporosis. $$$ pMDI 125/25 µg or250/25 µg: 2 puffs BID Diskus 100/50 µg, 250/50 µg or 500/50 Patients with personal or family history of glaucoma (and need high-dose inhaled corticosteroids) should have IOP checked soon after starting therapy and periodically thereafter. Fixed-dose combination inhalers are more convenient, enhance adherence, ensure the patient receives their inhaled corticosteroid with their LABA, and are less $$$ $ Class Drug Adverse Effects Dose µg: 1 inhalation BID Diskus expensive than the individual agents combined. Not for reliever therapy. Corticosteroid/LA mometasone/formoter BA ol fumarate dihydrate Combinations Zenhale Cos ta Comments A disadvantage is a loss in dosing flexibility. pMDI 50/5 µg, 100/5 µg or200/5 µg: 2 puffs BID $$$ Not for reliever therapy. Legend: $ < $25 $$ $25–50 $$$ $50–75 $$$$ $75–100 $$$$$ $100–125 Respiratory Disorders: Asthma in Adults; David G. McCormack, MD, FRCPC, FCCP; Date of revision: April 2015 Medication salmeterol Uses asthma adjuvant, nocturnal and exercise induced Contraindications (CI), drug interactions (DI) or cautions DI: CYP 3A4 inhibitor Increased deaths in African-American and children Long acting beta agonists increases risk of asthma related death Adverse Effects (common and severe) upper respiratory tract infection, inflammation, pharyngitis, hoarseness, dysphonia, bronchitis, cough, headache, nausea, vomiting, sinusitis, musculoskeletal pain, fever, dizziness Initial dose; typical dose MDI: 25mcg 2 puffs every 12 hours Diskus: 50mcg inhaled every 12 hours Monitoring