Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
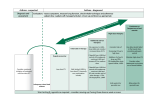
CHRONIC ASTHMA Resident Author: Julia Wystma. MD Faculty Advisor: Lisa Bell, MD CCFP Created: January 2012 Overview1,2,3 • • Asthma - inflammatory disorder of the airways characterized by paroxysmal or persistent symptoms (see below) with associated variable airflow limitation and airway hyper-responsiveness. It is common (affects 12% of children and 8% of adults), has significant impact (mortality rate of 20 children/year and 500 adults/year, and leading cause of missed school and third for work) Diagnostic Considerations • Clinical diagnosis made by combining genetic predisposition, clinical signs and symptoms, and objective measures of lung function • History: frequent episodes of dyspnea, wheezing, cough, or chest tightness Symptoms often: • Are worse at night and early morning or • Develop with URTI, or after exercise/laughing/playing , or after exposure to allergens or irritants • Improve with bronchodilators and steroids • Physical exam: wheezing, tachypnea, decreased breath sounds, accessory muscle use, indrawing and nasal flaring • Investigations: 3 methods for diagnosis- one preferred and two alternates (see Table 1) Table 1. Diagnosis of asthma Pulmonary function measurement Criteria for children (ages ≥ 6) Adult criteria 1) Preferred = Spirometry: showing reversible airway obstruction Reduced FEV1/FVC AND Increase in FEV1 after a bronchodilator or course of controller therapy Less than lower limit of normal based on age, sex, height, and ethnicity AND ≥ 12% Less than lower limit of normal based on age, sex, height and ethnicity AND ≥12% (and minimum ≥200mL) 2) Alternate = Peak expiratory flow (PEF) variability: showing variable airflow limitation Increase after a bronchodilator or after a course of controller therapy OR Diurnal variation ≥20% OR Not recommended 60L/min (≥20%) OR >8% based upon twice daily readings; >20% based upon multiple daily readings 3) Alternate = Positive challenge test: showing airway hyper-responsiveness Metacholine challenge OR Exercise challenge • PC20 < 4mg/mL (4-15mg/mL is borderline) OR ≥10-15% decrease in FEV1 post-exercise Differential diagnosis of coughing + wheezing by age: o Infants and children: allergic rhinosinusitis, cystic fibrosis, enlarged lymph nodes, foreign body, heart disease, tumour, viral bronchiolitis, vocal cord dysfunction o Adults: COPD, CHF, Ace inhibitor cough, post-nasal drip, GERD, pertussis, post-viral cough, mechanical airway obstruction, PE, pulmonary infiltration with eosinophils, vocal cord dysfunction Management Considerations1,2,3,4 Management includes a) education b) pharmacotherapy, and c) regularly reassessment of control A) Self-management education: ongoing (≥2x/year) education includes: o Lifestyle: identify and avoid personal irritant and allergic triggers (ex. pets, mould, pollen, etc) (see: http://www.uptodate.com/contents/patient-information-trigger-avoidance-in-asthma) o Medications: review adherence, benefits, and side effects, and check inhaler techniques (see: http://www.asthma.ca/adults/treatment/howToUse.php) o Written action plan: a plan that outlines 1) daily preventative management for control 2) when and how to adjust reliever and controller therapy during exacerbations, and 3) when to seek urgent medical attention (see: http://www.lung.ca/_resources/asthma_action_plan.pdf, or www.AsthmaActionPlan.com) o Working with a support team (eg. asthma educator) B) Pharmacologic management: use a step wise approach 1. Begin with reliever therapy o Reliever therapy= SABA as needed. Indicated for all patients and as monotherapy for patients with mild infrequent symptoms and normal expiratory flow. 2. If reliever use >3 times per week or any other indicator of poor control present (see Table 2) add on controller therapy starting with low dose ICS (or LTRA as second line for pediatrics) o Controller therapy = daily ICS,ICS plus LABA, or LTRA. (see Table 3) Dr. Michael Evans developed the One-Pager concept to provide clinicians with useful clinical information on primary care topics. CHRONIC ASTHMA Table 2. Indicators of asthma control INDICATOR FREQUENCY/VALUE Daytime symptoms <4 days/week Night-time symptoms <1 night/week Physical activity Normal Exacerbations Mild, infrequent Absence from work/school due to asthma None Need for SABA <4 doses/week FEV1 or PEF >90% personal best PEF diurnal variation <10-15% 3. If control suboptimal then adjust based on age (Table 3): Table 3. Recommended controller therapy by age 6-11 years old >12 years old First line low dose ICS low dose ICS Second line med dose ICS low dose ICS + LABA Third line med dose ICS + LABA OR med dose ICS + LTRA med dose ICS + LABA OR low dose ICS + LABA + LTRA 4. Additional considerations: consider oral steroids for severe symptoms, theophylline as fourth line in adults only, and omalizumab (XolairTM) for poor control of atopic asthma in patients older than 12 C) Reassessment: assess control at each visit via history and objective measures (see Table 2) , as well assess inhaler techniques, adherence, triggers, comorbidities, and growth in children. Patients on reliever-only therapy require yearly follow-up, patients on controller therapy should be seen at least twice a year. Repeat spirometry every 1-2 years to assess airway function and response to treatment. Pharmacotherapy 2,4,5 DRUG NAME DRUG FORM STRENGTH ADULT DOSE DOSE/DAY AGE COMMENTS -side effects: tremor, nervousness, tachycardia, prolonged QT, headache, hypokalemia, increased insulin secretion and hyperglycemia (caution in diabetics) Short-acting Beta2 Agonists (SABA) Salbutamol (VentolinTM) MDI 100ug 1-2 puffs PRN 1200ug PRN ≥4y Diskus 200, 400ug 200ug inh PRN 1600ug PRN ≥4y Terbutaline (BricanylTM) Turbuhaler 500ug 500ug inh PRN 4000ug PRN ≥6y Long-acting Beta2 Agonists (LABA) Salmeterol (SereventTM) Diskus 50ug 50ug inh BID 100ug ≥4y Formoterol (OxezeTM) Turbuhaler 6ug, 12ug 6-12ug puff BID 24-48ug ≥6y -NOT as controller monotherapy , to be used as an add-on agent with steroid (see below, LABA and ICS Combos) -formoterol has faster onset and in an emergency may be used as rescue therapy -side effects: tachycardia and tremor (worse with formoterol) -formoterol contains lactose Long-acting Beta2 Agonist and Inhaled Corticosteroid Combos (LABA+ICS) Formoterol + Budenoside (SymbicortTM) Turbuhaler 6/100ug 6/200ug 2 puffs BID 1-4 puffs BID ≥12y Salmeterol + Fluticasone (AdvairTM) MDI 25/125ug 25/250ug 2 inh BID 1-2 inh BID ≥12y Diskus 50/100ug 50/250ug 50/500ug 1 inh BID 1 inh BID ≥4y Formoterol + Memetasone (ZenhaleTM) MDI 5/50 ug 5/100 ug 5/200 ug 2 inh BID 2ihn BID ≥12y -combo convenient but dose less flexible -allows safe administration of LABA and may be steroid-sparing -see LABA and ICS side effects -symbicort contains lactose -do not use 2 puffs on diskus, instead increase to next strength to avoid LABA adverse effects Inhaled Corticosteroids (ICS) Fluticasone (FloventTM) MDI 50, 125, 250ug 2 puffs BID 100-2000ug ≥1y Diskus 50,100, 250, 500ug 2 puffs 50-250 BID or 1 puff 250-500 BID 100-2000ug ≥4y Budenoside (PulmicortTM) Turbuhaler 100,200,400ug 2 puffs BID 400-2400ug ≥6y Beclomethasone (QvarTM) MDI 50, 100ug 2 puffs BID 100-800ug ≥5y Ciclesonide MDI 100,200,400 ug 1 puff daily 400ug ≥6y (AlvescoTM) -requires regular use -use lowest effective dose, may try nocturnal use -side effects: oral thrush and dysphonia (reduced with spacer and rinsing), mildly reduced growth velocity in children for first year of use (not sustained), at high doses may have adrenal dysfunction, hyperglycemia, and osteoporosis - increase risk of Cushing’s CHRONIC ASTHMA Leukotriene receptor antagonists (LTRA) Montelukast Tab Age 1-5: 4 mg chewable Age 6-14: 5 mg chewable Age >14: 10 mg 10mg PO qhs 10mg ≥1y Tab 20mg 20 mg PO BID 40mg ≥12y (SingulairTM) Zafirlukast (AccolateTM) -second/third-line controller -usually used for pediatrics -oral treatment option, good for patients with exercise induced bronchospasm, ASA sensitivity, and allergic rhinitis -side effects: rare eosinophilic vasculitis, possible psych, increased LFTs for zafirlukast -drug interaction between zafirlukast and warfarin/ theophylline *Asthma management in pregnancy good asthma control is associated with improved neonatal outcomes and asthma medications have not been shown to increase the risk of fetal malformations. Motherisk recommends that asthma treatment be similar for pregnant and non-pregnant patients (for further details please see: http://www. motherisk.org/women/updatesDetail.jsp?content_id=296 ) Colour Drug BLUE Salbutamol (Ventolin) GREEN Salmeterol (Serevent) ORANGE Fluticasone (Flovent) PURPLE Salmeterol/Fluticasone (Advair) Patient Resource (please also see resources under Self-Management stage of Management) http://www.ginasthma.org/pdf/GINA_PatientGuide2007.pdf http://www.lung.ca/diseases-maladies/asthma-asthme_e.php Bottom Line Asthma is chronic disease with paroxysmal symptoms that continues to cause significant morbidity and mortality. Diagnosis is made based on a combination of clinical history and exam with objective measures of lung functions, with spirometry being the preferred method. Management involves patient education, step-wise pharmacotherapy, and routine reassessment. Abbreviations SABA = short acting beta agonist ICS = inhaled corticosteroids LABA = long acting beta agonist LTRA = leukotriene receptor antagonist FEV1 = forced expiratory volume in 1 second FVC = forced vital capacity Diurnal variation = difference between morning pre-bronchodilator PEF and maximum daily, as percent maximum PC20 = provocative concentration of metacholine producing a 20% fall in FEV1 References can be found online at http://www.dfcm.utoronto.ca/programs/postgraduateprograme/One_Pager_Project_References.htm