Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
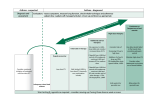
Asthma - Treatment UCI INTERNAL MEDICINE MINI-LECTURE SERIES BY KEVIN COOK Objectives Understand severity scoring vs. control in guiding the treatment of asthma Discuss the utility of the “asthma ladder” in step up and step down therapy Introduce new therapies used in patients with refractory asthma Asthma Severity vs. Control Severity - the intrinsic intensity of the disease process Dictates which step to initiate treatment Intermittent symptoms require rescue medication Persistent symptoms require controller medication Control - the degree to which the goals of therapy are met prevent symptoms/exacerbations, maintain normal lung function and activity levels Assessing Severity Class Daytime symptoms Nocturnal symptoms Intermittent 2x or less per week 2x or less per mo Mild Persistent >2x per week >2x per mo Moderate Persistent Daily >1x per week Severe Persistent Continual Frequent All patients classified in a “persistent” asthma category will require initiation of controller medications Assessing Control - The Asthma Ladder High dose ICS + LABA AND oral corticosteroid Step 5 High dose ICS + LABA Step 4 Medium dose ICS + LABA Step 3 Low dose ICS + LABA OR Medium dose ICS Step 2 Low dose ICS Step 1 SABA as needed Step Up Therapy Step 6 Step Down Therapy Intermittent Asthma Persistent Asthma Asthma Step Ladder Assessing Control – Should I Step Up? Well controlled Not well controlled Poorly controlled Daytime symptoms 2x or less per week >2x per week daily Night awakenings 2x or less per month >2x per month >3x per week SABA use 2x or less per week >2x per week daily FEV1 or peak flow >80% 60-80% <60% Recommendation Maintain current step Step up 1, reevaluate 2-6 weeks Step up 1-2, Consider short course of oral steroids, reevaluate in 2 weeks Case Study A 24 y/o patient with mild persistent asthma was initially well controlled with low dose inhaled corticosteroid. Today he returns for follow up. He is now complaining of increasingly frequent episodes of shortness of breath, using his short-acting beta agonist 3 times per week. Which of the following statements is correct regarding management of this patient? a) continue current management as symptoms require beta agonist less than once daily b) add a long acting beta agonist c) increase to medium dose inhaled corticosteroid d) add tiotropium e) B or C Assessing Control – Should I Step Up? Well controlled Not well controlled Poorly controlled Daytime symptoms 2x or less per week >2x per week daily Night awakenings 2x or less per month >2x per month >3x per week SABA use 2x or less per week >2x per week daily FEV1 or peak flow >80% 60-80% <60% Recommendation Maintain current step Step up 1, reevaluate 2-6 weeks Step up 1-2, Consider short course of oral steroids, reevaluate in 2 weeks Assessing Control - The Asthma Ladder High dose ICS + LABA AND oral corticosteroid Step 5 High dose ICS + LABA Step 4 Medium dose ICS + LABA Step 3 Low dose ICS + LABA OR Medium dose ICS Step 2 Low dose ICS Step 1 SABA as needed Step Up Therapy Step 6 Step Down Therapy Intermittent Asthma Persistent Asthma Asthma Step Ladder Case Study A 24 y/o patient with mild persistent asthma was initially well controlled with low dose inhaled corticosteroid. Today he returns for follow up. He is now complaining of increased shortness of breath and using his short-acting beta agonist 3 times per week. Which of the following statements is correct regarding management of this patient? a) continue current management as symptoms require beta agonist less than once daily b) add a long acting beta agonist c) increase to medium dose inhaled corticosteroid d) add tiotropium e) B or C On step 6 and still not well controlled? Alternative diagnoses such as COPD, left ventricular failure, localized obstruction, cystic fibrosis and/or vocal cord dysfunction should be ruled out Omalizumab - anti-IgE therapy in patients with allergic asthma (works by binding IgE so that it cannot complex with allergens to stimulate immune cells Bronchial thermoplasty – heat applied directly to the airways by bronchoscopy to reduce the airway smooth muscle mass and attenuate bronchoconstriction Summary Initial treatment of asthma requires assessment of severity Longitudinal treatment requires assessment of control with the use of the “asthma ladder” for step up and step down therapy Persistent symptoms require controller medication: start with ICS and add LABA if still not controlled Seek consultation if high dose ICS are required References National Asthma Education and Prevention Program, Third Expert Panel on the Diagnosis and Management of Asthma. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda (MD): National Heart, Lung, and Blood Institute (US); 2007 Aug.Available from: http://www.ncbi.nlm.nih.gov/books/NBK7232/ Scialla, Timothy. “Asthma Summary 2013”. Hopkins Modules.