Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
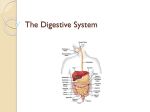
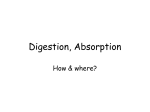
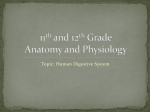
Digestive Organs Digestive System Organs of the Alimentary Canal Keri Muma Bio 6 Histology of the Alimentary Canal Digestive Organs Accessory organs Salivary glands Teeth Pancreas Liver Gallbladder Functions Ingestion – taking food in Propulsion – movement of food along the digestive tract Mucosa – innermost layer lining the lumen, mucus membrane epithelium Submucosa – areolar CT layer Muscularis externa – inner circular and outer longitudinal layer of smooth muscle Serosa – outermost layer lining the external surface Peristalsis Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Involuntary waves of contraction and relaxation of muscles in the organ walls Propel digestive material forward through the digestive tract Peristalsis Segmentation 1 Segmentation Contractions that churn and break apart digestive material Functions Digestion – breaking down food into smaller molecules Functions Absorption Regulation of Digestive Tract Activity – transport of nutrients from the lumen of the gastrointestinal tract to the blood Defecation – elimination of indigestible substances from the body Autonomous Smooth Muscle Mechanical – changing physical structure Chemical – changing chemical structure Regulation of digestion involves: Autonomous smooth muscle Mechanical and chemical stimuli – stretch receptors, osmolarity, and presence of substrate in the lumen Gastrointestinal hormones Extrinsic nerves control by CNS centers Intrinsic nerves control by local centers (Enteric Nervous System) Autonomous Smooth Muscle Visceral smooth muscle is autonomous Smooth muscle pacemaker cells display rhythmic, spontaneous variations in membrane potentials (slow wave potential) Hormones, mechanical stress, and nerve stimuli determines the starting point of the slow wave potentials 2 Receptors of the GI Tract Receptors respond to changes in the digestive tract Nervous Control of the GI Tract Long reflexes Mechanoreceptors – respond to stretch or pressure Osmoreceptors – changes in osmolarity Chemoreceptors – pH, presence of substrates, and end products of digestion Their activation produces short and/or long reflexes that will: Activate or inhibit digestive glands Activate or inhibit smooth muscle Nervous Control of the GI Tract Can alter muscle and gland activity Can alter levels of hormone secretions Modify intrinsic activity Coordinate different parts of the GI tract Example: chewing food causes increased gastric secretions in stomach (feed forward mechanism) Nervous Control of the GI Tract Short reflexes Nervous Control of the GI Tract Stimulus may be within or outside the GI tract Involves integration in CNS (usually in the medulla) and output sent via autonomic nerves to GI tract Extrinsic control Involves the enteric nervous system - myenteric and submucous plexus within the digestive tract wall Intrinsic control - entire reflex arc is carried out within the GI tract (responds to local stimuli) Coordinates local activity, can work independently of the CNS or it can be influenced by extrinsic nerves because it is linked to long autonomic reflex arcs Digestive Peptides Gastrointestinal peptides can act as digestive hormones and paracrine signals Released into the blood or ECF by cells of the digestive tract Can act on digestive organs and accessory organs to excite or inhibit motility or secretions Can also act on the brain to trigger hunger or satiety See table 21-1 in your textbook for a summary of these hormones and their effects 3 Mouth Chewing begins mechanical digestion by breaking food into smaller pieces and mixing food with saliva Compacts food into a bolus The salivary enzyme amylase begins the chemical digestion of carbohydrates Polysaccharides Mouth Saliva Secreted from serous and mucous cells in the salivary glands Composition Maltose amylase Control of Salivation Control of Salivation Salivary secretion is enhanced by two reflexes: Simple reflex - ingested food stimulates chemoreceptors and pressoreceptors that trigger the salivary center in the medulla Acquired reflex - the thought of food, cortex triggers the salivary center in the medulla Involves the coordinated activity of the tongue, soft palate, pharynx, and esophagus Buccal phase – bolus is forced into the oropharynx (voluntary) Pharyngeal-esophageal phase – controlled by the medulla and lower pons (involuntary) Peristalsis moves food through the pharynx and the esophagus Autonomic Nervous System (ANS) Deglutition (Swallowing) 97-99.5% water Digestive enzyme – salivary amylase Mucus – moistens food and holds bolus together Lysozyme and IgA – antibacterial action Parasympathetic – larger volume of saliva, watery and rich with amylase Sympathetic – smaller volume, more mucus, results in dry mouth Stomach Food enters stomach from the esophagus through the gastroesophageal sphincter 4 Digestion in the Stomach Gastric Phase: Long and Short Reflexes Functions of the stomach: Mixes and stores food until it can be emptied into the small intestines Degrades the bolus both physically and chemically Food is mixed with gastric juices to produce chyme Enzymatically digests proteins with the enzyme pepsin Secretes intrinsic factor required for absorption of vitamin B12 Digestion in the Stomach Digestion in the Stomach Four phases of gastric motility Gastric filing Storage Mixing Emptying Gastric filling Stomach relaxes as it fills, rugae flatten out Stomach dilates in response to gastric filling (1L) Gastric storage Peristaltic contractions are weak in the body of the stomach, so little mixing occurs Digestion in the Stomach Gastric mixing Takes place in the muscular antrum Occurs as chyme is propelled forward against the closed pyloric sphincter by peristaltic contractions Gastric Secretions Exocrine Mucous cells – produce mucus to protect stomach wall from harsh acids Parietal cells – produce HCL and intrinsic factor Chief cells – produce pepsinogen, an inactive form of the protein digesting enzyme pepsin 5 Digestion in the Stomach Gastric Secretions Chemical digestion of proteins begins in the stomach Pepsinogen is converted into pepsin by HCl Pepsin breaks down proteins into peptide fragments Proteins Peptides Cephalic (reflex) phase: prior to food entry Gastric phase: once food enters the stomach Intestinal phase: as partially digested food enters the duodenum Regulation of Gastric Secretion ECL cells – secrete histamine, stimulates secretion from parietal cells D cells – secrete somatostatin, inhibits secretions from parietal, ECL cells, and G cells Regulation of Gastric Secretion Neural and hormonal mechanisms regulate the release of gastric juices Excitatory and inhibitory events occur in three phases: G cells – produce the hormone gastrin which stimulates gastric acid secretion Paracrine Pepsin Regulation of Gastric Secretion Endocrine Cephalic phase – prior to food entry Excitatory events include: Sight or thought of food Stimulation of taste, smell, pressure receptors; chewing Vagal stimulation releases ACh – stimulates parietal, G cells, and ECL cells Inhibitory events include: Loss of appetite or depression Decrease in stimulation of the parasympathetic division Summary of Gastric Secretions Gastric Phase Excitatory events include: Stomach distension - activation of stretch receptors (neural activation) Activation of chemoreceptors by peptides, caffeine, and alkaline pH Triggers release of gastrin into the blood Inhibitory events include: An acidic pH lower than 2 - triggers release of somatostatin 6 Regulation and Mechanism of HCl Secretion Regulation of Gastric Secretions Figure 23.17 Release of Gastric Juice Regulation of Gastric Secretion Intestinal Phase Mostly inhibitory Inhibitory phase – distension of duodenum, presence of fatty, acidic, or hypertonic chyme in the duodenum Initiates local reflexes and vagal nuclei Closes the pyloric sphincter Release of hormones that inhibit gastric secretion Cholecystokinin and Secretin – decrease gastric secretions and slows gastric motility Gastric inhibitory peptides (GIP) – inhibits gastric acid secretion, also promotes insulin release from pancreas Figure 23.16 Digestion in the Stomach Gastric emptying A strong enough peristaltic wave can push a small amount of chyme through the pyloric sphincter before it closes tightly The rate of gastric emptying is controlled by both gastric and duodenal factors Digestion in the Stomach Gastric factors that increase gastric emptying Amount of chyme in the stomach – the stomach empties at a rate that is proportional to the volume of chyme Distention – triggers smooth muscle and intrinsic plexuses Fluidity of chyme Signaling by the vagus nerve (extrinsic control)" The hormone gastrin " 7 Rate of Gastric Emptying Regulation of Gastric Emptying The duodenum controls gastric emptying by reducing peristaltic activity in the stomach until it is ready to accommodate more chyme The neural enterogastric reflex -when the duodenum fills stretch receptors are stimulated and the pyloric sphincter closes Hormonal mechanisms: Cholecystokinin and secretin – released by duodenal endocrine cells into the blood; will inhibit gastric motility Duodenal factors that decrease gastric emptying Gastric emptying is regulated by: Fatty chyme – digested and absorbed slower than other nutrients in the duodenum Acidity – chyme must be completely neutralized Hypertonicity – need time for absorption of nutrients to catch up with digestion Distention – needs to cope with volume before receiving more Small Intestines Regulation of Gastric Emptying Extends from the pyloric sphincter to the ileocecal valve Main function is chemical digestion and absorption of nutrients Three regions: Duodenum – first part Chemical digestion, absorption Jejunum – middle Absorption Ileum – last part, joins the large intestines Figure 23.19 Small Intestines Surface area for absorption is increased by villi and microvilli Substances must pass through an epithelial cells and then diffuse through the interstitial fluid in the underlying CT into a capillary or lacteal Duodenum Chyme enters the duodenum where it is mixed with bile from the liver and digestive enzymes from the pancreas 8 Functions of the Liver Produces bile to aid in the digestion of fats Stores excess nutrients and releases them when needed Detoxifies drugs and metabolites Produces plasma proteins Function of Bile Bile is secreted into the duodenum to emulsify fats Bile increases the surface area for lipase to work on fats Production of Bile by the Liver Hepatocytes produce bile and secrete it into bile ducts that empty into the common hepatic duct. The sphincter of Oddi at the base of the common bile duct prevents bile from entering the duodenum between meals Bile will back up into the gallbladder where it is concentrated and stored Composition of Bile Bile is composed of: Aqueous alkaline solution Bile salts Regulation of Bile Release Cholesterol Lecithin – a phospholipid Bilirubin – byproduct of destruction RBC Regulation of Bile Release Acidic, fatty chyme causes the duodenum to release: Cholecystokinin (CCK) and secretin into the bloodstream Nonpolar portion – cholesterol based steroid Polar portion Secretin transported in blood stimulate the liver to produce bile Cholecystokinin causes the gallbladder to contract and the sphincters to relax Vagal stimulation causes weak contractions of the gallbladder Figure 23.25 9 Recycling of Bile Salts The Pancreas Most bile salts are reabsorbed back into the blood in the ileum are returned by the hepatic portal system About 5% of bile escapes in feces Secretes pancreatic juices into the duodenum that break down all categories of food Acini cells secrete digestive enzymes Duct cells secrete NaHCO3– which neutralizes acidic chyme Regulation of Pancreatic Secretion When chyme enters the duodenum CCK and secretin enter the bloodstream Upon reaching the pancreas: Regulation of Pancreatic Secretion CCK induces the secretion of enzyme-rich pancreatic juice Secretin causes secretion of bicarbonate-rich pancreatic juice Vagal stimulation also causes release of pancreatic juice Figure 23.28 Summary of Intestinal-Phase Pancreatic Enzymes See Table 21-1 on page 702 for summary of hormones Proteolytic enzymes are released in an inactive form and are activated in the duodenum Each breaks different peptide bonds resulting in short peptides and amino acids Enterokinase Trypsinogen Chymotrypsinogen Procarboxypeptidase Trypsin Trypsin Trypsin Chymotrypsin Carboxypeptidase 10 Proteolytic Enzyme Activation Pancreatic Enzymes Amylase – hydrolyzes polysaccharides into disaccharides Nucleases – hydrolyzes nucleic acids into nucleotides Lipase – hydrolyzes triglycerides into monoglycerides and fatty acids Brush Border Enzymes Final chemical digestion is carried out by brush border enzymes found in the plasma membrane of the small intestine’s mucosal cells Disaccharides Monosaccharides Maltase Sucrase Lactase Peptides Amino Acids aminopeptidase Absorption in the Small Intestines Most electrolytes, nutrients and vitamins are completely absorbed Vitamins Fat soluble vitamins such as A, D, E, and K are absorbed along with lipids Water soluble vitamins such as C and B are passively absorbed with water Vitamin B12 is combined with intrinsic factor and absorbed by receptor mediated endocytosis in the ileum 11 Absorption in the Small Intestines Minerals Absorption in the Small Intestines Iron Ca2+ and iron are absorbed on an as needed basis mostly by active transport Ca2+ absorption: Depends on blood levels of ionic calcium Is regulated by vitamin D and parathyroid hormone (PTH) Absorption of Nutrients Electrolyte Absorption Cl-, H20, glucose, and amino acids absorption depends on active transport of Na+ into the interstitial fluid Active transport of Na+ creates a concentration gradient Water follows the osmotic gradient and anions passively follow the electrical gradient established by sodium Na+ re-entry through a cotransporter can drive solutes against the concentration gradient Absorption of Sugars Absorbed iron is stored in the epithelial cells as ferritin until needed If blood iron levels are low it is released into the blood Carried in the blood by transferrin to the bone marrow to be used for RBC production Absorption of sugars and amino acids Facilitated diffusion via cotransport with Na+, Driven by secondary active transport Enter the capillary bed in the villi Transported to the liver via the hepatic portal vein Absorption of Amino Acids 12 Absorption of Lipids When micelles get close to the absorptive surface lipids are released and diffuse into intestinal cells where they are: Synthesized into triglycerides in the SER Combine with proteins to form chylomicrons in the golgi apparatus Released by exocytosis Enter lacteals and are transported to systemic circulation via lymph Motility in the Small Intestine Motility in the Small Intestine After nutrients have been absorbed: A series of peristaltic waves called the migrating motility complex begins with each wave starting distal to the previous Sweeps remnants of the previous meal, bacteria, mucosal cells, and debris into the large intestine Regulated by the hormone motilin which is released during the postabsorptive state by mucosa endocrine cells Functions Absorb remaining water, electrolytes, vitamin K Eliminates indigestible food from the body Factors enhancing the intensity of segmentation contractions: Distention Gastrin Extrinsic nerves Ileum empties into the cecum through the ileocecal valve The gastroileal reflex – ileocecal sphincter relaxes and allows chyme to pass into the large intestine Large Intestines Frames the small intestines Extends from the ileocecal valve to the anus It is initiated by intrinsic pacemaker cells (Cajal cells) Mixes chyme with digestive juices and exposes it to the absorptive surface of the small intestines Moves contents steadily toward the ileocecal valve Motility of the Small Intestines Segmentation is the most common motion of the small intestine Triggered by food entering stomach Gastrin and increased motility of the small intestines Motility of the Large Intestines Segmentation in the large intestines occurs less frequently (3 to 4 times a day) Gastrocolic reflex – contraction of the ascending and transverse colon results in mass movement of content forward into the rectum Triggered by gastrin and extrinsic nerves when food enters the stomach 13 Defecation Reflex Distention of the rectum triggers stretch receptors causing the internal sphincter to relax (involuntary) When the external sphincter is voluntarily relaxed defecation occurs Figure 23.32 14