Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychedelic therapy wikipedia , lookup
Orphan drug wikipedia , lookup
Psychopharmacology wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Compounding wikipedia , lookup
Neuropharmacology wikipedia , lookup
Clinical trial wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Drug design wikipedia , lookup
Pharmacognosy wikipedia , lookup
List of off-label promotion pharmaceutical settlements wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Prescription costs wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Theralizumab wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
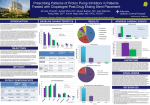
DRUG REGULATORY AGENCIES’ ROLE IN THE INTERACTION BETWEEN CLOPIDOGREL AND PROTON PUMP INHIBITORS Over the last three years, scientific community has followed with great interest the discussion about the potential interaction and its clinical impact between clopidogrel and proton pump inhibitors (PPI). Moreover, and in parallel with the publication of clinical studies, drug regulatory agencies issued successive official statements that deserve, in our opinion, a specific analysis and assessment. The Food and Drug Administration (FDA) has been leading this issue since its first statement in January 2009. In this document(1) the FDA warned about the potential interaction and advised to reassess the appropriate use of each PPIs. Ten months later, they issued a second report(2) based primarily on the findings of two unpublished pharmacodynamic studies requested to the clopidogrel manufacturers(3). This new recommendation, which is currently in force, puts the emphasis on discouraging the concomitant use of clopidogrel with omeprazole or esomeprazole, claiming insufficient information for the rest of PPIs. On the other hand, each FDA statement was followed shortly after by a report published by the European Medicines Agency (EMA)(4,5). National drug regulatory agencies such as the British MHRA(6) or the Spanish Medicines Agency (AEMPS)(7,8) transferred the European recommendations to the healthcare professionals, providing the scientific references that could justify them. What considerations can be made after a detailed reading of these documents? Initially we find it reasonable and positive that drug regulatory agencies publish their findings even in the absence of conclusive data. However, there are important questions that must be analyzed carefully. For example, have been properly selected and weighted key trials that support the new recommendation? Is it possible to improve the transparency and quality of the scientific references provided? In short, are the new recommendations appropriate in the light of up-todate scientific evidence? In our view, the current approach discouraging exclusively the concomitant use of either omeprazole or esomeprazole with clopidogrel is biased for several reasons: The main argument supporting the recommendation, first advocated by the FDA and then assumed by the rest of agencies, seems to come from the small pharmacodynamic trials previously mentioned(Error! Bookmark not defined.). In these studies unusually high doses of omeprazole (80 mg daily) were used, the clinical relevance of the interaction was not considered and no comparative information with respect to other PPIs, except for pantoprazole 80 mg, has been provided(3). A question raise immediately: if omeprazole 20 mg or pantoprazole 40 mg is commonly recommended for the protection of gastrointestinal injury, why were selected so unusual doses of PPI in these trials? Secondly, omeprazole 80 mg and pantoprazole 80 mg are not equipotent doses, so this suggests that the outcomes of the studies could be biased twice: a very high and also no comparable dose selected, promoting a more favourable outcome for pantoprazole. And last but not least, surprisingly pantoprazole is directly claimed as a safe PPI, even though the degree of platelet inhibition observed with high doses of pantoprazole was less than observed with clopidogrel alone, as the FDA report says literally(3). We think it's necessary to clarify without delay all these questions, in order to maintain or not a different recommendation about particular PPIs. At the same time, it is quite surprising the low significance given to the information provided by experimental studies focused on clinical outcomes. Furthermore, although the latter also have some limitations, they are better designed to minimize the selection bias than observational trials, and have shown that adding a PPI to clopidogrel provides gastrointestinal protection(9) without increasing cardiovascular risk(9,10). Moreover, scientific references cited by national drug health authorities to support their conclusions are not really convincing. While the EMA published its two documents without attaching any related reference(4,5), the AEMPS based its new recommendation on incomplete sources such as the following(8): pharmacodynamic studies previously considered in its first report(7), two trials whose findings do not match the recommendations of the report(9,10) and two observational studies with limited novelty in one case(11) and no assessment of the interaction in the other one(12). The MHRA was more accurate in selecting the references provided(6), but their findings clearly disagree (9,10,13) with the final recommendations of the document. Considering the lower gastroprotective efficacy of the H2 antihistaminic drugs, the absence of interaction between clopidogrel and H2 antihistaminics (and even antiacids) mentioned by the FDA(2) calls for a critical appraisal of their place in therapy, which is crucial to be addressed especially in haemorrhagic high-risk patients. Finally, from a practical point of view, both clopidogrel and omeprazole are very useful drugs when used appropriately, being a first-line treatment in well defined conditions. Thus, a warning published on the grounds of a poor clinical outcome can promote a quick shift to drugs with similar uncertainties and a less favorable efficiency profile. In summary, we could say that the new recommendations made by the drug agencies are primarily based on a few pharmacodynamic data, not available for all PPIs, and of uncertain clinical relevance. Thinking about future statements, it would be needed to optimize the scientific references support. In relation to clopidogrel and PPIs interaction, drug authorities should call for caution on all PPIs to the same extent, outweigh properly their gastroprotective benefit, clarify the role of H2 antihistaminics and promote studies with all PPIs at standard and equipotent doses. In this regard, recent articles such as full publication of COGENT study(14) or AHA/ACC/AGA 2010 consensus(15) emphasize the central role of PPIs in reducing serious gastrointestinal complications related with antiplatelet therapy. In brief, we demand comprehensive recommendations based on the best available clinical evidence. Otherwise, we will extend the confusion and distrust among healthcare professionals. 1 Food and Drug Administration. Early Communication about an Ongoing Safety Review of clopidogrel bisulfate (marketed as Plavix). [26 january 2009]. Free access on: http://www.fda.gov/cder/drug/early_comm/clopidogrel_bisulfate.htm 2 Food and Drug Administration. Information for Healthcare Professionals: Update to he labeling of clopidogrel bisulfato (marketed as Plavix) to alert healthcare professionals about a drug interaction with omeprazole (marketed as Prilosec and Prilosec OTC). [17 november 2009]. Free access on: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm190848.htm 3 Plavix (clopidogrel bisulfate) US label [august 2010]. Free access on: http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/020839s048lbl.pdf 4 European Medicines Agency. Public statement on possible interaction between clopidogrel and proton pump inhibitors. [29 may 2009]. Free access on: http://www.ms.public.lu/fr/activites/pharmacie-medicament/clopidogrel-emea-statement.pdf 5 European Medicines Agency. Interaction between clopidogrel and proton-pump inhibitors. [17 march 2010]. Free access on: http://www.ema.europa.eu/docs/en_GB/document_library/Public_statement/2010/03/WC500076346.pdf 6 Clopidogrel and proton pump inhibitors: interaction-updated advice. Drug Safety Update. April 2010;3(9):4-5. Free access on: http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON087711 7 Spanish Medicines Agency. Informative note 2009/07 [3 juin 2009] “Clopidogrel and proton pump inhibitors possible interaction” [Posible interacción de clopidogrel con los inhibidores de la bomba de protones]. Free access (in Spanish) on: http://www.aemps.es/actividad/alertas/usoHumano/seguridad/NI_2009-07_clopidogrel.htm 8 Spanish Medicines Agency. Informative note 2010/04 [26 april 2010] “Clopidogrel and proton pump inhibitors interaction: information updated and use recommendations” [Interacción de clopidogrel con los inhibidores de la bomba de protones: actualización de la información y recomendaciones de uso]. Free access (in Spanish) on: http://www.aemps.es/actividad/alertas/usoHumano/seguridad/2010/NI_2010-04_clopidogrel.htm 9 Bhatt DL, Cryer B, Contant CF, et al. The COGENT Trial: A prospective, randomized, placebo-controlled trial of omeprazole in patients receiving aspirin and clopidogrel. Presented at: Annual Meeting of Transcatheter Cardiovascular Therapeutics; September 24, 2009; San Francisco, CA, USA. 10 O’Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Lancet. 2009;374:989-97. 11 Stanek EJ, Aubert R, Flockhart D, et al. A national study of the effect of individual proton pump inhibitors on cardiovascular outcomes in patients treated with clopidogrel following coronary stenting: the clopidogrel Medco Outcomes Study. Presented at SCAI, Las Vegas 2009:Abstract O-11. 12 Wallentin L, Becker RC, Budaj AB, et al. for the PLATO investigators. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. NEJM. 2009;361:1045-57. 13 Yasuda H, Yamada M, Sawada S, et al. Upper gastrointestinal bleeding in patients receiving dual antiplatelet therapy after coronary stenting. Intern Med. 2009;48(19):1725-30. 14 Bhatt DL, Cryer BL, Contant CF, et al. for the COGENT Investigators. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med. 2010;363:1909-17. 15 ACCF/ACG/AHA 2010 Expert Consensus Document on the Concomitant Use of Proton Pump Inhibitors and Thienopyridines: A Focused Update of the ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use. A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. 2010;56:2051-66.