Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
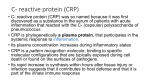
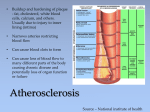
Technical Bulletin Number 116 High Sensitivity C-Reactive Protein (hs-CRP) Introduction Why High Sensitivity CRP? Over 50% of coronary events occur in individuals with low to moderate low density lipoprotein (LDL) cholesterol.1 The search for additional predictive risk factors has recently focused on the role of inflammation in the development of atherosclerosis. High sensitivity C-reactive protein, or hsCRP, is a systemic marker of inflammation and an effective marker for long-term risk assessment.2 Low level increases in CRP have been reported in various conditions and disease states that are thought to be associated with inflammation.2,5-7 The most prominently studied utility has been for cardiovascular disease, where CRP has been reported to predict cardiovascular outcomes independently of other conventional markers of risk.2,8,9Increases in CRP are nonspecific and should be interpreted in the context of a complete clinical evaluation. If elevated values are observed in an apparently healthy individual, the test should be repeated in order to help rule out a recent response to undetected infection or tissue injury. What is CRP? C-reactive protein (CRP) is an acute phase reactant that responds as a sensitive, though nonspecific, marker of systemic inflammation. The pentameric, globular protein is synthesized by the liver in response to stimuli from circulating inflammatory cytokines. CRP has traditionally been used as a systemic marker of infection and tissue injury.3 An expanding body of research now indicates that CRP likely plays a direct, active inflammatory role in blood vessels, leading to the development of atherosclerosis.4 Within 24–48 hours of an infectious or noninfectious stimulus, CRP levels may rise up to 3000-fold over circulating levels seen in apparently healthy individuals, typically less than 10 mg/L.3 CRP levels in conditions characterized by chronic inflammation, such as rheumatoid arthritis and certain other rheumatic disorders, are likewise characterized by significant elevations. Conventional CRP assays have therefore been optimized to facilitate measurement of dynamic increases in concentration. But this is achieved at the expense of sensitivity to detect low level increases due to more subtle causes of inflammation. Conventional CRP assays that can accommodate very large increases have not been optimized for the highly sensitive detection of the low level increases characterizing these clinical applications. CRP levels in apparently healthy individuals can be below 0.2 mg/L,10 requiring high sensitivity – or hs-CRP – assays. How are hs-CRP Results Interpreted? Hs-CRP values range between 0.3 and 8.6 mg/L in healthy men and between 0.2 and 9.1 mg/L in healthy women who are not taking hormone Low grade replacement therapy.10 inflammation may occur in apparently healthy individuals, placing them at increased risk of the conditions noted above. In a recent scientific statement,9 the Centers for Disease Control and Prevention (CDC) and the American Heart Association (AHA) recommended the following interpretation of hs-CRP results: • < 1 mg/L Low Risk • 1–3 mg/L Average Risk • > 3 mg/L High Risk Increases in CRP are nonspecific, however, and should be interpreted in the context of a complete clinical evaluation. Hs-CRP values > 8 mg/L observed in an apparently healthy individual should be repeated in order to help rule out a recent response to undetected infection or tissue injury.9 Standardization of hs-CRP The CDC is coordinating a project to standardize hs-CRP assays. Cholestech participated in the first phase of this project which concluded that it is feasible to use Certified Reference Material (CRM) 470 as a secondary reference material for hs-CRP assays.11 The second phase of the standardization project involves working with manufacturers to ensure accurate calibrator value assignment and to normalize assay results. Cholestech standardizes the Cholestech LDX® hs-CRP assay using diluted CRM470, and intends to adjust its process in accord with CDC recommendations. Differences Among hs-CRP Methods A variety of methods are employed by the various manufacturers of hs-CRP assays. These include several immunoturbidometric approaches, chemiluminescence, particleenhanced immunonephelometry, and the lateral flow immunoassay technique of the Cholestech LDX hs-CRP assay. Like Cholestech, most manufacturers claim to standardize their assays using CRM470. However, differences in standardization are clearly evident,11,12 likely as a result of differences in assay methodologies and manufacturing processes. Testing hs-CRP on the Cholestech LDX Cholestech LDX hs-CRP is an in vitro diagnostic test for the quantitative determination C-reactive protein in whole blood or serum. Measurement of CRP is useful as an aid in the detection and evaluation of infection, tissue injury, inflammatory disorders, and associated diseases. Cholestech LDX hs-CRP tests are for use in laboratories certified for moderate complexity testing. Instructions for running the hs-CRP test will be found in the package insert in each box of hs-CRP cassettes. Please read the hs-CRP package insert before running an hs-CRP test and note the following: • Fingerstick samples are collected using a Cholestech LDX 50 µL Capillary Tube. Please note that this is a different volume/capillary tube than any other Cholestech LDX test that you might already perform. • Fingerstick samples must be applied to the cassette within 5 minutes after collection. Place the cassette into the drawer of the analyzer immediately after dispensing the sample into the well. • After pressing Run, hs-CRP results will be displayed in 6 minutes (results will be displayed in 4 minutes for serum or plasma samples). • Hematocrit levels between 30% and 55% do not affect results. Quality Control Quality control should be run routinely to show that your Cholestech LDX System is giving accurate results. Ensure that sample type is set to Serum mode in the Configuration menu. Controls must be tested: • With each new shipment of cassettes (even if cassettes are from the same lot previously received). • With each new lot of cassettes received. • As required by your laboratory’s standard Quality Control procedures. • Each day that patient samples are tested. • If your local or state regulations require more frequent testing of Quality Control material. Note that if you will be running fingerstick or whole blood samples after you have tested Quality Control materials, be sure to change the sample type in the Configuration menu to Whole Blood mode. The quality control results should be within range before testing patient samples. Refer to the Cholestech LDX User Manual if they are not. Contact Cholestech Technical Service (1.800.733.0404) prior to testing patient samples. CPT Code hs-CRP and bacterial infection in preterm infants. Eur J Pediatr 1990; 149:424-7. 6. Spector TD, Hart DJ, Nandra D, Doyle DV et al. Low-level increases in serum C-reactive protein are present in early osteoarthritis of the knee and predict progressive disease. Arthritis Rheum 1997; 40:723-7. 7. Schmidt R, Schmidt H, Curb JD, Masaki K et al. Early inflammation and dementia: a 25year follow-up of the Honolulu-Asia Aging Study. Ann Neurol 2002; 52:168-74. 8. Danesh J, Whincup P, Walker M, Lennon L et al. Low grade inflammation and coronary heart disease: prospective study and updated meta-analyses. BMJ 2000; 321:199-204. 9. Pearson TA, Mensah GA, Alexander RW, Anderson JL et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003; 107:499511. 10.Rifai N, Ridker PM. Population distributions of C-reactive protein in apparently healthy men and women in the United States: implication for clinical interpretation. Clin Chem 2003; 49:666-9. 11.Kimberly MM, Vesper HW, Caudill SP, Cooper GR et al. Standardization of immunoassays for measurement of high-sensitivity C-reactive protein. Phase I: evaluation of secondary reference materials. Clin Chem 2003; 49:611-6. 86141 References 1. Wilson PW, D'Agostino RB, Levy D, Belanger AM et al. Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97:1837-47. 12. Roberts WL, Moulton L, Law TC, Farrow G et al. Evaluation of nine automated highsensitivity C-reactive protein methods: implications for clinical and epidemiological applications. Part 2. Clin Chem 2001; 47:418-25. 2. Ridker PM. Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation 2003; 107:363-9. 3. Pepys MB. C-reactive protein fifty years on. Lancet 1981; 1:653-7. 4. Szmitko PE, Wang CH, Weisel RD, de Almeida JR et al. New markers of inflammation and endothelial cell activation: Part I. Circulation 2003; 108:1917-23. 5. Wasunna A, Whitelaw A, Gallimore R, Hawkins PN, Pepys MB. C-reactive protein Cholestech LDX is a registered trademark of Cholestech Corporation. CPT is a registered trademark of the American Medical Association. © 2005 Cholestech Corporation MKT13226 Rev. A 08/05 Printed in USA. To assist you with any further questions, please call Technical Service: 1.800.733.0404 3347 Investment Blvd. Hayward, CA 94545 U.S.A. Tel 800 733.0404 Fax 510 732.7227 www.cholestech.com