Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
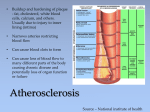
Inflammation and Cardiovascular Disease: the Missing Link? Vijay U. Rao, MD, PhD, FACC, FASE Director Inpatient Heart Failure and Cardiac Research Franciscan Physician Network, Indiana Heart Physicians Franciscan St. Francis Health Indianapolis, IN Presenter Disclosure Information Inflammation and Cardiovascular Disease: the Missing Link? Vijay Rao, MD, PhD, FACC, FASE • Speaker’s Bureau for Pfizer, Bristol Myers Squibb, Daichi Sankyo, Novartis • I will not discuss off label or investigational use in my presentation. Beyond Cholesterol: Predicting Cardiovascular Risk In the 21st Century Cardiovascular Risk Lipids HTN Diabetes Behavioral Hemostatic Thrombotic Inflammatory •On the basis of 2008 mortality rate data, more than 2200 Americans die of CVD each day, an average of 1 death every 39 seconds. •Coronary heart disease caused ≈1 of every 6 deaths in the United States in 2008. Circulation. 2012; 125: e2-e220 Genetic Inflammation: A Historical Perspective • Roman Celsus in 1st century AD: 4 signs of inflammation (rubor et tumor cum calore et dolore “redness and swelling with heat and pain”) • 2 centuries later, Galen developed the humoral view of inflammation as a beneficial response to injury (pus generation) • In 1871, Virchow: function laesa, loss of function as the 5th cardinal sign Inflammatory Cascade Outline Inflammation and CV risk – Inflammatory conditions (RA, gout, PD) – Atherosclerosis – Inflammatory biomarker: hs-CRP – Statins and the JUPITER trial – Exercise and inflammation – Anti-inflammatory medicines (NSAIDs) Rheumatoid Arthritis Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease characterized by persistent symmetric polyarthritis (synovitis) that affects the hands and feet, although any joint lined by a synovial membrane may be involved. Cardiovascular (CV) disease is the leading cause of mortality (up to 50%) in patients with rheumatoid arthritis (RA) Traditional CV risk factors do not fully explain the higher incidence of CV disease in patients with RA. RA specific risk factors (rheumatoid factor or anti-CCP antibody positivity, HLA-DR shared epitope, inflammatory markers such as CRP, joint erosions, extra-articular disease characteristics, and duration of disease) appear to have a stronger association with CV events Morbidity and mortality studies show that the incidence of CV disease is about 1.5 – 3 fold greater in RA patients than in the general population. Event rate per 1000 person-years Cardiovascular event rates among subjects with and without RA in a cohort study in British Columbia Myocardial infarction (MI), stroke, or cardiovascular (CV) death Solomon DH, et al. Ann Rheum Dis. 2006;65:1608-1612. The increased incidence of CV events in patients with RA is not explained by traditional CV risk factors alone Male Gender Current smoker Personal Hx of IHD Family Hx of IHD Hypertension Dyslipidemia RA Non-RA BMI 30 kg/m2 Diabetes mellitus BMI <20 kg/m2 Hazard Ratios and 95% CI at baseline Gonzalez. Ann Rheum Dis 2008;67:64-69. Inflammatory conditions associated with enhanced CV risk and/or premature CAD Systemic lupus erythematosis HIV Gout Periodontitis Inflammatory bowel disease Severe psoriasis Treatments (anti-TNF-alpha, IL-6 inhibitors) raise cholesterol levels; jury is still out on whether these agents will reduce CV risk, though TNF-alpha blockers were shown to be detrimental in CHF patients Inflammation and Atherogenesis Libby P. Circ J 2010; 74: 213 – 220 CRP vs hs-CRP • CRP is an acute-phase protein produced by the liver in response to cytokine production (IL-6, IL-1, tumor necrosis factor) during tissue injury, inflammation, or infection. • Standard CRP tests determine levels which are increased up to 1,000-fold in response to infection or tissue destruction, but cannot adequately assess the normal range • High-sensitivity CRP (hs-CRP) assays (i.e. Dade Behring) detect levels of CRP within the normal range, levels proven to predict future cardiovascular events. hs-CRP and Risk of Future MI in Apparently Healthy Men (Physician’s Health Study) P Trend <0.001 P<0.001 Relative Risk of MI 3 P<0.001 2 P=0.03 1 0 1 2 Quartile of hs-CRP Ridker et al, N Engl J Med. 1997;336:973–979. 3 4 hs-CRP and Risk of Future Stroke in Apparently Healthy Men P Trend <0.03 Relative Risk of Ischemic Stroke 2 P=0.02 P<0.02 3 4 1 0 1 2 Quartile of hs-CRP Ridker et al, N Engl J Med. 1997;336:973–979. hs-CRP Adds Prognostic Information at all Levels of LDL-C and at all Levels of the Framingham Risk Score <1.0 1.0-3.0 >3.0 <1.0 C-Reactive Protein (mg/L) 25 3 1.0-3.0 >3.0 C-Reactive Protein (mg/L) 15 Relative risk 10 5 0 0-1 2-4 5-9 10-20 Framingham estimate of 10-year risk (%) Ridker et al, N Engl J Med. 2002;347:1557. Multivariable relative risk 20 2 1 0 <130 130-160 >160 LDL cholesterol (mg/dL) Is there clinical evidence that inflammation can be modified by preventive therapies? Long-Term Effect of Statin Therapy on hs-CRP: Placebo and Pravastatin Groups (CARE trial) Placebo 0.25 Median hs-CRP Concentration (mg/dL) 0.24 0.23 -21.6% (P=0.004) 0.22 0.21 0.20 Pravastatin 0.19 0.18 Baseline Ridker et al, Circulation. 1999;100:230-235. 5 Years Effect of Statin Therapy on hs-CRP Levels at 6 Weeks hs-CRP (mg/L) 6 *p<0.025 vs. Baseline 5 * 4 * * 3 2 1 0 Baseline Prava Simva Atorva (40 mg/d) (20 mg/d) (10 mg/d) Jialal I et al. Circulation 2001;103:1933-1935Circulation 2001;103:1933-1935. JUPITER: Justification for the Use of statins In Primary prevention: An Intervention Trial Evaluating Rosuvastatin • Inflammation plays a crucial role in atherogenesis/plaque rupture • Inflammatory biomarker hs-CRP independently predicts vascular events and improves global classification of risk regardless of LDL-c levels • Statin therapy largely reduces hs-CRP in a manner independent of LDL-c reduction • Subgroup of AFCAPS/TexCAPS trial: no benefit of statin therapy with LDL-c < 150mg/dl and hs-CRP < 2mg/dl, whereas large clinical benefit seen when LDL-c < 150mg/dl and hs-CRP > 2mg/dl JUPITER: Primary Endpoint Ridker PM. N Engl J Med. 2008;359:2195–2207 Limitations of JUPITER • Of the approximately 90,000 individuals screened to participate in the JUPITER trial, approximately 26,000, or 28%, were excluded because their hsCRP was < 2 mg/L. • The JUPITER trial did not allow for comparison between individuals with an hsCRP < 2 mg/L to those with an hsCRP > 2 mg/L. • The JUPITER trial did not establish a particular goal of therapy for CRESTOR with respect to hsCRP levels. • Was the reduction in events driven by lowering of LDL or hsCRP? Exercise and Inflammation • Exercise induced muscle injury is thought to be responsible stimulus for IL-6 increases •IL-6 is thought to act like a hormone assisting glucose homeostasis and lipolysis From: The Effects of Physical Activity on Serum CReactive Protein and Inflammatory Markers: A Systematic Review J Am Coll Cardiol. 2005;45(10):1563-1569. doi:10.1016/j.jacc.2004.12.077 Exercise and Inflammation • Relationship between increased physical activity and lower CRP persists even after adjusting for BMI, waist-to-hip ratio, and fasting insulin concentration suggesting that other factors contribute to the exercise-related anti-inflammatory effect • Exercise training reduces CRP both directly by reducing cytokine production in fat, muscle, and mononuclear cells and indirectly by increasing insulin sensitivity, improving endothelial function, and reducing body weight. • High-intensity interval training (HIIT) vs continuous moderateintensity training (MICT), need more data about safety and outcomes J Am Coll Cardiol. 2005;45(10):15631569. doi:10.1016/j.jacc.2004.12.077 Elevated CRP Levels in Obesity: NHANES 1988-1994 Percent with CRP 0.22 mg/dL 25 20 15 10 5 0 Normal Overweight Visser M et al. JAMA 1999;282:2131-2135. Obese Effects of Weight Loss on CRP Concentrations in Obese Healthy Women 83 women (mean BMI 33.8, range 28.2-43.8 kg/m2) placed on very low fat, energy-restricted diet (6.0 MJ, 15% fat) for 12 weeks Baseline CRP positively associated with BMI (r=0.281, p=0.01) CRP reduced by 26% (p<0.001) Average weight loss 7.9 kg, associated with change in CRP Change in CRP correlated with change in TC (r=0.240, p=0.03) but not changes in LDL-C, HDL-C, or glucose At 12 weeks, CRP concentration highly correlated with TG (r=0.287, p=0.009), but not with other lipids or glucose Heilbronn LK et alArterioscler Thromb Vasc Biol 2001;21:968-970sc Biol 2001;21:968-970. NSAIDS and CV risk (estimated 30 million people worldwide use every day) AHA 2007 statement: celecoxib should be used "as a last resort on patients who have heart disease or a risk of developing it” Elevated risks occur because COX-2 inhibitors suppress prostacyclin—a vasodilator and platelet inhibitor with heart-protecting properties—in vascular cells (Yu Y et al. Sci Transl Med. 2012;4[132]:132ra54) How big a CV risk does NSAID use pose? Are certain NSAIDs safer than others? From: Cardiovascular Risk and Inhibition of Cyclooxygenase: A Systematic Review of the Observational Studies of Selective and Nonselective Inhibitors of Cyclooxygenase 2 JAMA. 2006;296(13):1633-1644. doi:10.1001/jama.296.13.jrv60011 Putting it all together • Inflammatory conditions (eg RA) have increased CV risk not fully explained by traditional CV risk factors • 50% of CHD occurs in people with below average total cholesterol • Inflammation (as measured by hs-CRP) is a powerful marker of enhanced CV risk • JUPITER study (inflammation and/or lipid reduction) makes a strong argument for increased statin usage to prevent CV events • Exercise and weight loss lower inflammation • NSAIDs are not innocuous; consider naproxen and ibuprofen as first line NSAIDs Future Directions • IL-1 beta mAb, p38MAPK inhibitor in phase III trials for ACS (reduce infarct size and prevent re-infarction) • Vaccination with anti-inflammatory peptides (target innate immune response, ? Which target) • Low-dose methotrexate in DM2 or metabolic syndrome with hx of vascular disease (CIRT trial) • Rationale, design, and governance of Prospective Randomized Evaluation of Celecoxib Integrated Safety versus Ibuprofen Or Naproxen (PRECISION), a cardiovascular end point trial of nonsteroidal antiinflammatory agents in patients with arthritis. Any questions? Back-Up slides How do JUPITER results affect my practice? • CLASS IIa (ACC/AHA 2010 guidelines), Evidence B – In men ≥ 50 yo or women ≥ 60 yo with LDL cholesterol < 130 mg/dL – not on lipid-lowering, hormone replacement, or immunosuppressant therapy; – without clinical CHD, diabetes, chronic kidney disease, severe inflammatory conditions, or contraindications to statins, measurement of hs-CRP can be useful in the selection of patients for statin therapy When should I check a hs-CRP? • Class IIb (ACC/AHA 2010 guidelines), Evidence B • In asymptomatic intermediate-risk men ≤50 yo or women ≤ 60 yo measurement of hs-CRP may be reasonable for cardiovascular risk assessment Class III: No benefit to hs-CRP measurement for CV risk assessment • Asymptomatic high risk individuals • Low-risk men<50yo or women<60yo Clinical Application of hs-CRP for Cardiovascular Risk Prediction 1 mg/L Low Risk 3 mg/L Moderate Risk 10 mg/L High Risk >100 mg/L Acute Phase Response Ignore Value, Repeat Test in 3 weeks Measurements of hs-CRP: • Should be performed twice (2 weeks apart) • Results averaged, expressed as mg/L • Fasting or nonfasting in metabolically stable patients (any time of day) • Cost: $60-150 depending upon lab Ridker PM. Circulation 2003;107:363-9; AHA/CDC panel recommendations for hs-CRP testing