Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
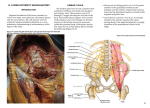
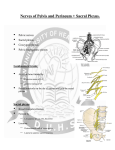
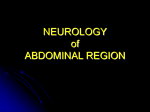
MR Imaging of Perineural Spread of Malignancy: A Case-Based Imaging Review Benjamin M. Howe M.D., Robert J. Spinner M.D., Mark A. Nathan M.D., Joel P. Felmlee Ph.D., Kimberly K. Amrami M.D. Mayo Clinic Rochester, MN Introduction: Perineural spread of malignancy is well known in head and neck tumors. It is also know to occur in gastrointestinal malignancy such as pancreatic cancer. Perineural spread of breast cancer is known to occur, but the diagnosis and MR imaging may be challenging in the setting of prior surgery and/or radiation. The post-gadolinium enhancement pattern is a critical factor when attempting to differential malignant spread along the plexus from radiation neuritis, or inflammatory neuropathies. Malignant plexus involvement is classically described on MR imaging as having a nodular appearance which is thought to represent small nodular foci of tumor along the nerves. Enhancement in radiation neuritis is typically thin smooth peripheral enhancement and in the chronic phase often has a retractile and fibrotic appearance about the plexus. In addition to the primary nerve findings, MR is an excellent modality for characterizing muscle denervation and atrophy which are more common in the setting of malignant invasion of the peripheral nerves. Thickening and enhancement of the ipsilateral perirectal fascia is an additional finding noticed in this small cohort of patients. It is possible this represents tumor cells about the inferior hypogastric and splanchnic plexus representing the pathway of disease spread. . Perineural spread of gastrointestinal and genitourinary malignancies are less frequently discussed. Local perineural involvement is known to occur in prostate and cervical cancer. In some cases, the perineural involvement can spread to involve lumbosacral plexus and the sciatic nerve. The purpose of this educational poster is to review the clinical presentation and imaging appearance of perineural spread of genitourinary malignancies to the lumbosacral plexus and sciatic nerve. We will discuss the anatomy that provides the pathway for spread and the MR imaging and clinical features that help make this diagnosis. Cases of perineural spread of pelvic malignancy will likely require a biopsy for definitive diagnosis. Perineural spread of malignancy is known to occur with “skip lesions” where normal segments of nerve are located between areas of tumor deposition. MRI is a useful tool to identify the point of maximal nerve abnormality in hopes of increasing the diagnostic yield of the biopsy. Anatomy: The lumbosacral trunk is formed by the L4 and L5 nerves. The lumbosacral trunk converges with the sacral plexus (S1-S4) to form the lumbosacral plexus. The parasympathetic innervation of the pelvic organs occurs via the splanchnic nerves from S2-S4. These splanchnic nerves coalesce with the hypogastric nerves to form the inferior hypogastric plexus. The inferior hypogastric plexus provides the innervation of the rectum and bladder. It forms the uterovaginal plexus in females and the prostatic plexus in males. The hypogastric plexus is a paired structure that lies along the perirectal fascia. Pathology: Local perineural invasion is well described in colorectal, cervical, and prostate cancer. Bastacky et al. reported perineural invasion in 20% of prostate needles biopsies and reported a relatively high specificity (96%) and low sensitivity (27%) in predicting extracapsular extension of disease (The American journal of surgical pathology 17.4 (1993): 336-341) . Subsequent studies of endorectal coil MR imaging have demonstrated improved prediction of extracapsular disease when compared to clinical and pathologic features alone. (Radiology 2004; 232:133–139) The evaluation of localized extension of disease is important in planning for nerve sparing operations for both prostate cancer and malignancies of the uterus and cervix. The vast majority of malignant disease in the pelvis with neurologic involvement occurs from direct invasion from the tumor or local mass affect. Rarely tumor can extend along the peripheral nerves and propagate proximal and distal to the site of the initial tumor. In rare cases, the tumor can spread to involve the lumbosacral plexus and sciatic nerve. Perineural spread of malignancy of rectal and genitourinary malignancies can propagate to involve the entire lumbosacral plexus and sciatic nerve. The proposed pathway to the sciatic nerve is: Prostatic/utero vaginal/vesical /rectal plexus Inferior hypogastric plexus Splanchnic plexus (S2S4) Lumbosacral plexus Sciatic nerve b. a. Case 1: A 61 year old man with perineural prostate cancer of the right sciatic nerve. Fat saturated coronal oblique and axial SPGR images demonstrate thick peripheral nerve enhancement (arrow) and ipsilateral perirectal fascial thickening (arrowheads). Schematic of proposed pathway of perineural spread of prostate cancer to the sciatic nerve. By permission of Mayo Foundation for Medical Education and Research. All rights reserved. Clinical Presentation: In addition to common clinical conditions such as lumbar spine disease and inflammatory neuropathies, the differential diagnosis in cancer patients with neuropathy includes radiation neuritis, chemotherapy induced neuropathy, and neuropathy associated malignancy (extrinsic mass with compression or perineural spread of disease). Radiating pain and weakness are clinical features that raise suspicion for malignant involvement of the peripheral nerves. Jaeckle et al. reviewed 85 patients with lumbosacral plexopathy secondary to a pelvic tumor and found that pain was the dominant clinical symptom (91%) and weakness the dominant clinical sign (86%). (Neurology 35.1 (1985): 8-8) The clinical signs and symptoms of perineural spread of malignancy in our small cohort of patients are similar to larger studies of malignant lumbosacral plexopathy associated with local direct invasion of the nerves by the primary tumor, such as described by Jaeckle et al. In contrast to malignant disease, radiation induced plexopathy classically presents with progressive sensory symptoms. (Radiotherapy and Oncology Volume 105, Issue 3, December 2012, Pages 273–28 ) MR Imaging: MR imaging of the lumbosacral plexus is preferred at 3 Tesla utilizing an 8 channel torso array coil. For the evaluation of potential perineural spread of malignancy, the MR exam is performed without and with intravenous gadolinium contrast. The noncontrast portion of the exam consists of T1 and T2-weighted fat-saturated images performed in the axial plane and a coronal oblique plane to the body of the sacrum. The axial image is performed with a field of view to cover the entire pelvis while the coronal oblique images are performed with a smaller field of view (24cm) from posterior to the sacrum to anterior to the sciatic notch. Post gadolinium spoiled gradient recall images with fat saturation are performed in the axial and coronal oblique planes. Case 2: A 61 year old woman with perineural cervical cancer of the left sciatic nerve. Fat saturated coronal oblique SPGR image demonstrate thick peripheral nerve enhancement (arrow) and ipsilateral perirectal fascial thickening (arrowheads). Cases/Conclusion: Five patients with gadolinium contrast pelvic MRI and perineural malignancy on a sciatic nerve biopsy were reviewed (Table). All patients had MR neural enhancement patterns suggesting an infiltrative process. Four of the five patients had ipsilateral perirectal fascial thickening which may represent the direct pathway of spread from the pelvic tumor to the sciatic nerve. MRI is a useful modality for identifying worrisome nerve enhancement patterns and for planning is cases where biopsy is indicated. Pain was the primary clinical symptom in these 5 patients. Perineural spread of malignancy may occur many years after initial therapy as demonstrated in our small cohort of patients. Case 3: A 71 year old man with perineural prostate cancer of the left sciatic nerve. Fat saturated axial SPGR image demonstrates thick peripheral nerve enhancement (arrow) and ipsilateral perirectal fascial thickening (arrowheads). Biopsy proven cases of sciatic perineural spread of pelvic malignancy Presentation after initial surgery Recurrent/Residual tumor in operative bed on MRI Cancer type Presentation Prostate Pain followed by progressive weakness and numbness Prostate Pain followed by numbness and tingling 9 yrs. No Prostate Pain and weakness 5 yrs. Yes Prostate Pain followed by weakness 16 yrs. Yes Cervical Pain and weakness 3 wks. Yes 13 yrs. No Metastatic disease Gadolinium enhancement Ipsilateral perirectal fascial thickening None (WB-BS, Skel. Survey) Nodular peripheral Yes None (C-11 choline CT/PET) None (C-11 choline CT/PET) Yes (C-11 choline PET/CT and WE-BS) Unknown (advanced local disease) Thick irregular peripheral Yes Fusiform Yes Thick peripheral Yes Thick peripheral Yes