Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
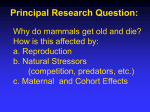
Pituitary DOI 10.1007/s11102-006-0408-5 Isolated corticotrophin deficiency Massimiliano Andrioli · Francesca Pecori Giraldi · Francesco Cavagnini Published online: 30 October 2006 C Springer Science + Business Media, LLC 2006 Abstract Isolated ACTH deficiency (IAD) is a rare disorder, characterized by secondary adrenal insufficiency (AI) with low or absent cortisol production, normal secretion of pituitary hormones other than ACTH and the absence of structural pituitary defects. In adults, IAD may appear after a traumatic injury or a lymphocytic hypophysitis, the latter possibly due to autoimmune etiology. Conversely, a genetic origin may come into play in neonatal or childhood IAD. Patients with IAD usually fare relatively well during unstressed periods until intervening events spark off an acute adrenal crisis presenting with non specific symptoms, such as asthenia, anorexia, unintentional weight loss and tendency towards hypoglycemia. Blood chemistry may reveal mild hypoglycemia, hyponatremia and normal-high potassium levels, mild anemia, lymphocytosis and eosinophilia. Morning serum cortisol below 3 µg/dl are virtually diagnostic for adrenal insufficiency. whereas cortisol values comprised between 5-18 µg/dl require additional investigations: insulin tolerance test (ITT) is considered the gold standard but— when contraindicated—high or low dose-ACTH stimulation test with serum cortisol determination provides a viable alternative. Plasma ACTH concentration and prolonged ACTH infusion test are useful in differential diagnosis between primary and secondary adrenal insufficiency. For some patients with mild, near-to-asymptomatic disease, glucocorticoid replacement therapy may not be required except during stressful events; for symptomatic patients, replacement doses i.e., mean daily dose 20 mg (0.30 mg/kg) M. Andrioli · F. P. Giraldi · F. Cavagnini () Chair of Endocrinology, University of Milan, Ospedale San Luca, Istituto Auxologico Italiano, Milan, Italy e-mail: [email protected] hydrocortisone or 25 mg (0.35 mg/kg) cortisone acetate, are usually sufficient. Administration of mineralocorticoids is generally not necessary as their production is maintained. Keywords ACTH deficicency . Hypopituitarism . Hypoglycemia . Hypophysitis Demographics and pathogenesis ACTH deficiency is usually associated with diminished GH, gonadotropin or TSH reserve, in the context of partial or total pituitary insufficiency. Isolated ACTH deficiency (IAD) is a rare disorder, first reported by Steinberg in 1954, characterized by secondary adrenal insufficiency (AI) with low or absent cortisol production, normal secretion of pituitary hormones other than ACTH and the absence of structural pituitary defects [1]. The prevalence of secondary AI, most commonly due to glucocorticoid administration, is much higher than that of primary AI, with an estimate of 150–280 cases per million [2, 3]. IAD accounts for only a small part of secondary AI and the rarity of its occurrence explains the uncertainties in its epidemiology and etiology. In adults, an autoimmune etiology is most often hypothesized, in alternative to traumatic cases. Indeed IAD may appear after a lymphocytic hypophysitis [4], especially in the peripartum period [5]. In support of this hypothesis, antibodies against a 22 kDalton pituitary protein have been detected in patients with IAD or lymphocytic hypophysitis [6, 7]. Post-traumatic ACTH deficiency is usually associated with other pituitary defects; persistent [8] or transient [9] post-traumatic IAD has been described. IAD may also be part of an atypical Sheehan’s syndrome [10], be associated to empty sella [11] and appear after radiation therapy for brain tumor [12]. Springer Pituitary Conversely, in neonatal or childhood IAD a genetic origin may be suspected. Laboratory diagnosis Blood chemistry Diagnosis Clinical diagnosis IAD has diverse clinical presentations and occasionally, if unrecognized, a fatal course. Clinical findings of IAD are similar to those found in primary AI although usually less severe [13] and excepting cutaneous hyperpigmentation and electrolyte disturbances. Patients with IAD usually fare relatively well during unstressed periods until intervening events spark off an acute adrenal crisis. This serious condition is characterized by extreme fatigue, acute abdominal pain, nausea and vomiting, diarrhea, fever, severe hypotension and hypoglycemia, and, if not promptly recognized, may be irreversible. Patients with IAD usually present with non-specific symptoms, such as asthenia, anorexia, unintentional weight loss and tendency to hypoglycemia. Alabaster-colored skin may contribute to the wan appearance of patients and aid in the distinction between primary and secondary AI. Unlike primary AI, secondary AI is not associated with lack of aldosterone, thus symptoms and signs of mineralocorticoid deficiency (salt-craving, postural hypotension, electrolyte abnormalities) are usually absent. Hyponatremia may occasionally occur as a result of reduced glomerular filtration rate, increased antidiuretic hormone secretion and concomitant hypothyroidism. IAD may present with atypical manifestations, such as flexion contractures of the legs [14] or severe muscle atrophy [15]. Other unusual presentations are pericardial effusion [16], recurrent syncope [17] or cholestatic jaundice [18]. These clinical manifestations, though not typical of AI, seem to be closely related to the hypoadrenal condition because they disappear on steroid replacement therapy. Primary infertility [19], Crohn’s disease [20], myasthenia gravis [21], polycystic kidney disease [22], spinocerebellar ataxia type 3 [23] and benign endocranic hypertension [24] have also been reported in conjunction with IAD. Lastly, IAD is not infrequent in chronic alcoholism [25, 26] and, as in patients with the above-mentioned disorders, should be considered if more typical hypoadrenal symptoms are present. Likewise, IAD should also be kept in mind in patients with other autoimmune diseases: IAD due to lymphocytic hypophysitis has often been described associated with autoimmune hypothyroidism [27, 28] and, occasionally, with Graves’ disease [29], type 1 diabetes [30] and polyglandular autoimmune failure [31]. Neonatal and childhood IAD will be discussed separately (see below). Springer Blood chemistry may reveal mild hypoglycemia, hyponatremia and normal-high potassium levels, mild anemia, lymphocytosis and eosinophilia, all signs of AI. Rarely, glucocorticoid deficiency can result in hypercalcemia, due to increased intestinal absorption and decreased renal excretion of calcium [32–35]. TSH is usually mildly elevated, as the physiological inhibitory effect of cortisol on TSH is absent [36]. Endocrine parametres Diagnosis of adrenal insufficiency Morning serum cortisol is usually the first step in the diagnostic work-up, although this test is indicative only if values are extremely low, i.e., adrenal insufficiency is near to certain with values below 3 µg/dl, or it can be excluded in the upper half of the normal range [37]. In fact, cortisol concentrations greater than >19 µg/dl [38, 39] or 18 µg/dl [40, 41] virtually exclude AI. Values in the intermediate range require additional dynamic testing. Urinary free cortisol has only suboptimal sensitivity as normal values are observed in 20% of patients with AI [42]. Insulin tolerance test (ITT) (regular insulin 0.1 U/kg as iv bolus in normal weight and 0.15 U/kg in overweight subjects, with measurement of blood glucose and cortisol at 0, 30 and 60 min) is considered the gold standard for evaluation of the entire hypothalamo-pituitary-adrenal axis. Although several cut-offs for a normal cortisol response have been suggested [43], the traditional value of 18 µg/dl [38, 41, 44] allows a good separation between healthy individuals and patients with AI. It should be kept in mind, however, that not all normal subjects attain this level of response [45] and a normal cortisol rise may occur in patients with symptoms of AI [46]. For the test to be valid, glycaemia should fall below 40 mg/dl (2.22 mmol/l) and symptoms of hypoglycemia should develop. ITT is contraindicated in patients older than 60 years and in those with a history of seizures or with documented/suspected coronary artery disease. Metyrapone test (MT). When ITT is contraindicated, and where the compound is available (not in the U.S.A.) the metyrapone test (metyrapone 30 mg/kg body weight given with a snack at midnight with measurement of cortisol and 11-deoxycortisol at 8 AM of the following morning) may be performed. Metyrapone inhibits 11β-hydroxylase and, hence, the conversion of 11-deoxycortisol into cortisol, thereby reducing the negative feedback and triggering ACTH release which, in turn, increases 11-deoxycortisol Pituitary production. Serum cortisol should decrease to less than 5 µg/dl, and 11-deoxycortisol should increase above 7 µg/dl. The sum of cortisol and 11-deoxycortisol after metyrapone should exceed 16.5 µg/dl [38, 47]. Both ITT and metyrapone may precipitate an acute adrenal crisis and should therefore be performed under close medical surveillance. High dose ACTH stimulation test (250 µg synthetic ACTH 1–24, cosyntropin, tetracosactin, Synacthen, as iv bolus with measurement of serum cortisol after 30, 60 min) directly assesses the adrenal secretory reserve, which may be impaired not only in primary AI but even in long-standing ACTH deficiency. Different cut-offs have been proposed and the most reliable appears to be cortisol peak greater than 18–20 µg/dl to exclude AI [48]. Recent onset or mild forms of secondary AI may not be detected by this test and a normal cortisol response does not exclude secondary AI [49], therefore ITT may be necessary to establish the diagnosis [50, 51]. Overall, peak cortisol levels at Synacthen and ITT testing appear in excellent agreement [52] and the high dose ACTH stimulation test may replace ITT in a substantial proportion of patients with suspected secondary AI. In minimally abnormal results the test should be repeated at least once, because the result is often normal on second assessment [53]. Low dose ACTH stimulation test (1 µg synthetic ACTH 1–24, Synacthen, as iv bolus with measurement of serum cortisol after 30, 60 min) has been proposed as a sensitive test for the diagnosis of secondary AI [54]. Using the cortisol >18 µg/dl criterion, this test allows an even better identification of patients with secondary AI compared with ITT [55–57] and the high dose ACTH test [58]. The advantage of the low dose compared with the high dose test may be offset by the technical difficulties inherent to dilution of 250 µg ampoules [59]. Due to the great difference in the 1–24 ACTH injected dose, a normal response with the high dose test is less reliable than with the low dose test whereas an insufficient response with the low dose test is less reliable than with the high dose test. In conclusion, since none of the above-mentioned tests correctly classify all patients, clinical judgment remains important. Differential diagnosis between primary and secondary AI Plasma ACTH concentration off glucocorticoid replacement therapy is the best parameter for the differential diagnosis, as levels are generally above 100 pg/ml in primary AI and low-normal in secondary AI. It is worth recalling that ACTH measurements are of little use in the initial diagnostic workup given the broad overlap between normal subjects and patients with central hypoadrenalism [60]. Prolonged ACTH infusion test (250 µg synthetic ACTH 1–24 injected into 500-ml bag of normal saline and infused at a constant rate over 8 h and blood sampling for cortisol measurement performed at 6 and 8 h). This test was used to distinguish primary from secondary AI prior to the development of reliable ACTH assays. Theoretically, patients with primary AI may display a significant cortisol rise in response to an acute ACTH bolus but be unable to maintain sustained cortisol secretion. However, the sensitivity of this test in patients with hypothalamic-pituitary disease is not significantly greater than that of other ACTH tests [61]. CRH test (1 µg/kg ovine or human CRH as iv bolus with serial serum samples for cortisol measurement during the following 2 h) has been used to differentiate hypothalamic from pituitary disease in secondary AI. The lack of studies involving large numbers of patients and the high cost of CRH has greatly limited the use of this test. Diagnosis of IAD Once the diagnosis of secondary AI has been established, normal secretion of the other pituitary hormones, as well as the absence of structural pituitary defects, except for the typical changes in case of hypophysitis, have to be ascertained. ITT, GnRH and TRH tests can be used to fulfill the first requirement while MR of the hypotalamic-pituitary region is sufficient for the latter (Fig. 1). In patients with autoimmune endocrine disorders pituitary antibodies should be searched for, especially with imaging suspicious of hypophysitis. Genetic testing (see below) has so far proven to be of little use in adult IAD. Treatment Long-term replacement therapy Treatment requires replacement doses of glucocorticoids. For some patients with mild, near-to-asymptomatic disease, glucocorticoid replacement therapy may not be required except for stressful events. Administration of mineralocorticoids is generally not necessary as their production is maintained. Based on the present knowledge on cortisol production rate [62], the recommended glucocorticoid replacement dose for patients with AI is lower than in the past, and in particular for patients with secondary AI [41]: mean daily doses of 20 mg hydrocortisone (0.30 mg/Kg) or 25 mg cortisone acetate (0.35 mg/Kg) are usually sufficient, with two-thirds of the dose administered in the morning. Cortisone acetate is metabolized to cortisol by 11β-hydroxysteroid dehydrogenase and has a later onset of action and longer biologic half-life than hydrocortisone. Peak serum cortisol concentrations after steroid administration vary substantially among individuals but rapidly reach supraphysiological levels followed by a decline to initial levels 5–7 h after Springer Pituitary Isolated ACTH Deficiency BIOCHEMICAL DIAGNOSIS 8 am serum cortisol < 3 µg/dl 3-18 µg/dl highly suspicious for AI suspicious for AI >18 µg/dl ITT, Synacthen Test 1 or 250 µg >18 µg/dl Cortisol <18 µg/dl AI AI EXCLUDED Normal plasma ACTH GH, TSH, PRL, high low LH & FSH secretion Primary AI AI:adrenal insufficiency Secondary AI IAD: isolated ACTH deficiency IAD Normal Pituitary imaging Fig. 1 Proposed algorithm for the diagnosis of isolated ACTH deficiency ingestion [63, 64]. This may result in low cortisol levels in the late afternoon and impaired quality of life. Recent studies indicate that thrice-daily regimens more closely mimics the physiological steroid circadian profile [65, 66]. Long-acting glucocorticoids can also be used in equivalent doses (1 mg hydrocortisone = 1.25 mg cortisone acetate = 0.2 mg prednisolone = 0.03 mg dexamethasone) but this may result in unfavorably high nocturnal cortisol levels. Reportedly, addition of dehydroepiandrosterone to glucocorticoid replacement therapy may exert positive effects on well-being and mood in patients with adrenal insufficiency [67]. However, treatment is hampered by the lack of pharmaceutically controlled preparations and large-scale studies are needed. At the present time, dehydroepiandrosterone (50 mg administered in the morning) should be reserved for patients whose well-being is clearly impaired despite optimal glucocorticoid replacement. Monitoring of glucocorticoid replacement therapy essentially relies on clinical judgment as no laboratory parameter is fully reliable. Indeed, morning plasma ACTH as well as cortisol levels are of little use and even urinary free cortisol excretion [68] exhibits considerable interindividual variability [63], thus fine-tuning glucocorticoid therapy is often very difficult. Urinary free cortisol levels may be of use to ex- Springer clude underreplacement, e.g., non-adherence to therapy, or overtreatment, i.e. iatrogenic Cushing’s syndrome. Other therapeutic recommendations In patients with non-isolated ACTH deficiency (partial or total pituitary insufficiency), thyroid replacement therapy should not be started before glucocorticoid replacement as thyroid hormones accelerate cortisol metabolism and thus may trigger an adrenal crisis if the patient has an inadequate adrenal reserve. Supervening stressful events, such as illnesses, trauma, fever, major surgical or diagnostic procedures, mandate an increase in glucocorticoid replacement dose (two to 10fold the maintenance dosage). Vomiting or diarrhea or other causes of poor intestinal absorption call for intravenous hydrocortisone administration. Patients on drugs that increase (e.g., phenytoin, rifampin, barbiturates) or decrease (e.g., protease inhibitors) cytochrome P450 3A4 activity, a key enzyme for hepatic glucocorticoid metabolism, may need higher or lower doses of glucocorticoids [69, 70]. Pregnant women usually do not require adjustments in their replacement dose although parenteral administration Pituitary may be needed to compensate for first trimester vomiting. Labor and C-section should be approached as usual for stressful events. Acute replacement therapy Management of acute adrenal crisis requires immediate intravenous administration of 100 mg hydrocortisone, followed by 100–200 mg over the next 24 h and large volumes of saline under continuous cardiac monitoring. Neonatal and childhood IAD Neonatal or childhood IAD may have genetic causes. A defect in the ACTH precursor, proopiomelanocortin (POMC), or in its cleavage enzyme, prohormone convertase, leads to defects in POMC-derived peptides (e.g., ACTH, MSH) and, hence, IAD; moreover, due to the dual role of α-MSH in regulating food intake and hair pigmentation, the phenotype associated with a defect in POMC should include obesity, alteration in hair pigmentation and ACTH deficiency [71]. Other candidate genes are CRH and CRH receptor type 1, but no mutations in these genes have been reported to be associated with IAD. Recently, mutations in TPIT, a pituitary transcription factor crucial for correct corticotroph embryonic development, have been described in a considerable proportion of neonatal IAD [72, 73]. Diagnosis Hypoglycemia, seizures, prolonged jaundice and growth retardation are the prevalent symptoms in neonatal IAD [73] and failure to establish a timely diagnosis may be fatal. Hydrocortisone should be administered immediately after obtaining blood samples for cortisol and ACTH. Identification of TPIT mutations allows prenatal diagnosis for families at risk and early glucocorticoid therapy in order to prevent neonatal death [73]. Noninvasive prenatal diagnosis can also be performed by measurement of estriol levels in plasma or urine of a pregnant woman as decreased maternal estriol of unexplained etiology may indicate fetal adrenal insufficiency secondary to IAD [74]. In childhood, symptoms of adrenal insufficiency require further investigation especially if associated with obesity and red hair pigmentation. References 1. Steinberg A, Shechter FR, Segal HI (1954) True pituitary Addison’s disease, a pituitary unitropic deficiency;fifteen-year follow-up. J Clin Endocrinol Metab 14:1519–1529 2. Laureti S, Vecchi L, Santeusanio F, Falorni A (1999) Is the prevalence of Addison’s disease understimated? J Clin Endocrinol Metab 84:1762 3. Tomlinson JW, Holden N, Hillis RK (2001) Association between premature mortality and hypopituitarism. Lancet 357:425–431 4. Escobar-Morreale H, Serrano-Gotarredona J, Varela C (1994) Isolated adrenocorticotropic hormone deficiency due to probable lymphocytic hypophysitis in a man. J Endocrinol Invest 17:127–131 5. Richtsmeier AJ, Henry RA, Bloodworth JM, Ehrlich EN (1980) Lymphoid hypophysitis with selective adrenocoticotropic hormone deficiency. Arch Intern Med 140:1243–1245 6. Takao T, Nanamiya W, Matsumoto R, Asaba K, Okabayashi T, Hashimoto K (2001) Antipituitary antibodies in patients with lymphocytic hypophysitis. Horm Res 55:288–292 7. Kikuchi T, Yabe S, Kanda T, Kobayashi I (2000) Antipituitary antibodies as pathogenetic factors in patients with pituitary disorders. Endocr J 47:407–416 8. Scooble JE, Havard CW (1990) Anosmia and isolated ACTH deficiency following a road traffic accident. Case raport. J Neurosurg 73:453–454 9. Karavitaki N, Wass J, Henderson Slater JD, Wade D (2006) A case of post-traumatic isolated ACTH deficiency with spontaneous recovery after 9 months after the event. J Neurol Neurosurg Psychiatry 77:276–277 10. Stacpoole PW, Kandell TW, Fisher WR (1983) Primary empty sella, hyperprolactinemia, and isolated ACTH deficiency after post partum hemorrhage. Am J Med 74:905–908 11. Fernandez Vazquez G, Pico Alfonso A, Estopian V, Tovar J, Zurita P, Hurtado A (1986) Isolated deficit of adrenocorticotropin hormone (ACTH) associated with primary empty sella turcica. Med Clin (Barc) 87:465–467 12. Sakai H, Yoshioka K, Yamagami K (2002) Complete adrenocorticotropin deficiency after radiation therapy for brain tumor with a normal growth hormone reserve. Intern Med 41:453–457 13. Vallotton MB (1992) Endocrine emergencies: disorders of the adrenal cortex. Baillieres Clin End Metab 6:41–56 14. Odagaki T, Noguchi Y, Fukui T (2003) Flexion contractures of the legs as the initial manifestation of adrenocortical insufficiency. Internal Medicine 42:710–713 15. Tamaya S, Ihara C, Tduji K, Nanno M, Maekawa N, Matsumoto S, Imai T (2000) Isolated ACTH deficiency with severe muscle atrophy. Nippon Naika Gakkai Zasshi 10:983–985 16. Pecori Giraldi F, Fatti L, Cavagnini F (2005) Isolated corticotrophin deficiency presenting with pericardial effusion. J Endocrinol Invest 28:831–833 17. Mayinger B, Harsch IA, Axelos D, Hahn EG (2000) Isolated ACTH deficiency as a rare cause of recurrent syncope and hypoglycemia. Med Klin (Munich) 95:701–705 18. Otsuka F, Yamamoto K, Shimada N, Kageyama J, Ogura T, Makino H (2004) Cholestatic jaundice: an unusual symptom of isolated adrenocorticotropin deficiency in adults. J Endocrinol Invest 27:404–405 19. Atkin SL, Masson EA, White MC (1995) Isolated adrenocorticotropin deficiency presenting as primary infertility. J Endocrinol Invest 18:456–459 20. Kalambokis G, Vassiliou V, Vergos T, Christou L, Tsatsoulis A, Tsianos EV (2004) Isolated ACTH deficiency associated with Crohn’s disease. J Endocrinol Invest 27:961–964 21. Corcuff JB, Lafranque P, Henry P, Roger P (1997) Isolated corticotroph insufficiency associated to myasthenia gravis. J Endocrinol Invest 20:669–671 22. Yonemura K, Yasuda H, Fujigaki Y, Oki Y, Hishida A (2003) Adrenal insufficiency due to isolated adrenocorticotropin deficiency complicated by autosomal recessive polycystic kidney disease. Ren Fail 25:485–492 Springer Pituitary 23. Ogawa K, Suzuki Y, Oishi M, Mizutani T, Nakayama T (2002) A case of spinocerebellar ataxia type 3 (SCA3) associated with isolated ACTH deficiency. Rinsho Shinkeigaku 42:149–153 24. Aanderud S, Jorde R (1988) ACTH deficiency, hyperprolactinemia and benign intracranial hypertension. Acta Endocrinol Copenh 118:346–350 25. Kearney T, Robinson S, Johnston D (2000) Isolated corticotropin deficiency in chronic alcoholism. J R Soc Med 93:15–17 26. Steer P, Marnell R, Werk EE (1969) Clinical alcohol hypoglicemia and isolated adrenocorticotrophic hormone deficiency. Ann Intern Med 71:343–348 27. Miller MJ, Horst TV (1982) Isolated ACTH deficiency and primary hypothyroidism. Acta Endocrinol (Copenh) 99:573–576 28. Martin-Du Pan RC, Rouiller D, Goumaz M (1994) Isolated ACTH deficiency and primary thyroid insufficiency in an atopic patient: hypophisitis? Schweiz Med Wochenschr 124:806–809 29. Miyauchi S, Yamashita Y, Matsuura B, Onji M (2004) Isolated ACTH deficiency with graves’ disease: a case report. Endocrine Journal 51:115–119 30. Giustina A, Candrina R, Cimino A, Romanelli G (1988) Development of isolated ACTH deficiency in a man with type I diabetes mellitus. J Endocrinol Invest 11:375–377 31. Kojima I, Nejima I, Ogata E (1982) Isolated adrenocorticotropin deficiency associated with polyglandular failure. J Clin Endocrinol Metab 54:182–186 32. Vasikaran SD, Tallis GA, Braund WJ (1994) Secondary hypoadrenalism presenting with hypercalcemia. Clin Endocrinol (Oxf) 41:261–64 33. Saito T, Tojo K, Yamamoto H, Hosoya T, Tajima N (2002) Isolated adrenocorticotropin deficiency presenting with impaired renin-angiotensin-aldosterone system and suppressed parathyroid hormone-vitamin D axis. Intern Med 41:561–565 34. Strachan MW, Walker JD, Patrick AW (2003) Severe hypercalcaemia secondary to isolated adrenocorticotrophic hormone deficiency and subacute thyroiditis. Ann Clin Biochem 40:295– 297 35. Kato A, Shinozaki S, Goga T, Hishida A (2003) Isolated adrenocorticotropic hormone deficiency in a patient on long-term haemodialysis. Am J Kidney Dis 42:32–36 36. Hangaard J, Andersen M, Grodum E, Koldkjaer O, Hagen C (1996) Pulsatile TSH secretion in patient with Addison’s disease during variable glucocorticoid therapy. J Clin Endocrinol Metab 81:2502–2507 37. Arlt W, Alloio B (2003) Adrenal insufficiency. Lancet 361:1881– 1893 38. Nieman LK (2003) Dynamic evaluation of adrenal hypofunction. J Endocrinol Invest 26:74–82 39. Grinspoon SK, Biller BM (1994) Clinical review 62: Laboratory assessment of adrenal insufficiency. J Clin Endocrinol Metab 79:923–931 40. Oelkers W (1996) Adrenal insufficiency. N Engl J Med 335:1206– 1212 41. Salvatori R (2005) Adrenal insufficiency. JAMA 294:2481–2488 42. Snow K, Jiang NS, Kao PC, Scheithauer BW (1992) Biochemical evaluation of adrenal dysfunction : the laboratory perspective. Mayo Clinic Proc 67:1055–1065 43. Hurel SJ, Thompson CJ, Watson MJ, Harris M, Baylis PH, Kendall-Taylor P (1996) The short synacthen and insulin stress tests in the assesment of the hypotalamic-pituitary adrenal axis. Clin End (Oxf) 44:141–146 44. Nelson JC, Tindall DJ (1978) A comparison of the adrenal response to hypoglicemia, metyrapone and ACTH. Am J Med Sc 275:165–172 45. Lindholm J, Kehlet H (1987) Reevaluation of the clinical value of the 30 min ACTH test in assessing the hypotalamic-pituitaryadrenocortical function. Clin Endocrinol (Oxf) 26:53–59 Springer 46. Tsatsoulis A, Shalet SM, Harrison J, Ratcliffe WA, Beardwell CG, Robinson EL (1998) ACTH deficiency undetected by standard dynamic tests of hypotalamic-pituitary-adrenal axis. Clin Endocrinol (Oxf) 28:225–232 47. Berneis K, Staub JJ, Gessler A, Meier C, Girard J, Muller B (2002) Combined stimulation of ACTH and compound-S by single dose metyrapone test as an outpatient procedure to assess hypothalamic-pituitary-adrenal function. J Clin Endocrinol Metab 87:5470–5475 48. Hockings GI, Nye EJ, Grice JE, Jackson RV (1997) Short synacthen test versus insulin stress test for the assessment of hypothalamo-pituitary axis: controversy revisited again. Clin Endocrinol (Oxf) 46:775–776 49. Dorin RI, Qualls CR, Crapo LM (2003) Diagnosis of adrenal insufficiency. Ann Intern Med 139:194–204 50. Streeten DH, Anderson GH, Bonaventra MM (1996) The potential for serious conseqences from misinterpreting normal responses to the rapid ACTH test. J Clin Endocrinol Metab 81:285–290 51. Borst GC, Michenfelder HJ, O’Brian JT (1982) Discordant cortisol response to exogenous ACTH and insulin-induced hypoglyicemia in patients with pituitary disease. N Eng J Med 302:1062– 1064 52. Stewart PM, Corrie J, Seckl JR, Edwards CR, Padfield PL (1988) A rational approach for assessing the hypothalamo-pituitary-adrenal axis. Lancet 1:1208–1210 53. May ME, Carey RM (1985) Rapid ACTH test in practice. Am J Med 79:679–684 54. Dickstein G, Shechner C, Nicholson WE (1991) ACTH test: effect of basal cortisol level, time of day and suggested new sensitive low dose test. J Clin Endocrinol Metabol 72:773–778 55. Bangar V, Clayton RN (1998) How reliable is the short synacthen test for the investigation of the hypothalamo-pituitary-adrenal axis? Eur J Endocrinol 139:580–583 56. Amari F, Issa BG, Millward E, Scanion MF (1996) A comparison between short ACTH and ITT for assessing hypothalamopituitary-adrenal function. Clin Endocrinol (Oxf) 44:473–476 57. Tordjman K, Jaffe A, Trostanetsky Y, Greenman Y, Limor R, Stern N (2000) Low dose ACTH stimulation as a screening test for impaired hypothalamo-pituitary-adrenal axis function: sensitivity, specificity and accuracy in comparison with high dose test. Clin Endocrinol (Oxf) 52:633–640 58. Thaler LM, Blevins LS (1998) The low dose ACTH test in the evaluation of patients with suspected central adrenal insufficiency. J Clin Endocrinol Metab 83:2726–2729 59. Murphy H, Livesey J, Espiner EA, Donald RA (1998) The low dose ACTH test: a further wor of caution. J Clin Endocrinol Metab 83:712–713 60. Oelkers W, Diederich S, Bahr V (1992) Diagnosis and therapy sorveillance in Addison’s disease: rapid ACTH test and measurement of plasma ACTH, renin activity and aldosterone. J Clin Endocrinol Metab 75:259–264 61. Nye EJ, Grice JE, Hockings GI, Strakosch CR, Crosbie GV, Walters MM, Torpy DJ, Jakson RV (2001) ACTH stimulation tests in patients with hypothalamo-pituitary disease: low dose, standard high dose and 8-h infusion tests. Clin Endocrinol (Oxf) 55:625– 633 62. Esteban NV, Loughlin T, Yergey AL, Zawadzki JK, Booth JD, Winterer JC, Loriaux JL (1991) Daily cortisol production rate in man determined by stable isotope diluition/mass spectometry. J Clin Endocrinol Metab 71:39–45 63. Allolio B, Kaulen D, Deuss U, Hipp FX, Winkelmann W (1985) Comparison between hydrocortisone and cortisone acetate as replacement therapy in adrenocortical insufficiency. Akt Endokr Stoffw 6:35–39 64. Feek CM, Ratcliffe JG, Seth J, Gray CE, Toft AD, Irvine WJ (1981) Patterns of plasma cortisol and ACTH concentrations Pituitary 65. 66. 67. 68. 69. 70. in patients with Addison’s disease treated with conventional corticosteroid replacement. Clin Endocrinol (Oxf) 14:451–458 Howlett TA (1997) An assessment of optimal hydrocortisone replacement therapy. Clin Endocrinol (Oxf). 46(3):263–268 Mah PM, Jenkins RC, Rostami-Hodjegan A, Newell-Price J, Doane A, Ibbotson V, Tucker GT, Ross RJ (2004) Weight-related dosing, timing and monitoring hydrocortisone replacement therapy in patients with adrenal insufficiency. Clin Endocrinol (Oxf) 61(3):367–375 Artl W, Callies F, van Vlijmen JC (1999) Dehydroepiandrosterone replacement therapy in women with adrenal insufficiency. N Engl J Med 341:1013–1020 Howlett TA (1997) An assessment of optimal hydrocortisone replacement therapy. Clin Endocrinol (Oxf) 46:263–268 Lamberts SWJ, Bruining HA, De Jong FH (1997) Corticosteroid therapy in severe illness. N Engl J Med 337:1285–1292 Eagling VA, Back DJ, Barry MG (1997) Differential inhibition of cytochrome P450 isoform by the protease inhibitors ritonavir, sequinavir and indinavir. Br J Clin Pharmac 44:190–194 71. Krude H, Biermann H, Luck W, Horn R, Brabant G, Gruters A (1998) Severe early-onset obesity, adrenal insufficiency and red hair pigmentation caused by POMC mutations in humans. Nat Genet 19:155–157 72. Lamolet B, Pulichino AM, Lamonerie T, Gauthier Y, Brue T, Enjalbert A, Drouin J (2001) A pituitary cell-restricted T box factor, Tpit, activates POMC in transcription in cooperation with Pitx homeproteins. Cell 104:849–859 73. Vallette-Kasic S, Brue T, Pulichino AM (2005) Congenital isolated adrenocorticotropin deficiency: an understimated cause of neonatal death, explained by TPIT gene mutations. J Clin Endocrinol Metab 90:1323–1331 74. Weintrob N, Drouin J, Vallette-Kasic S, Taub E, Marom D, Lebenthal Y, Klinger G, Bron-Harlev E, Shohat M (2006) Low estriol levels in the maternal triple-marker screen as a predictor of isolated adrenocorticotropic hormone deficiency caused by a new mutation in TPIT gene. Pediatrics 117:322–327 Springer