Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Pericardial heart valves wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Echocardiography of the Tricuspid Valve
in Congenital Left Ventricular-Right Atrial
Communication
By NAVIN C. NANDA, M.D., RAYMOND GRAMIAK, M.D.,
AND
JAMES A. MANNING, M.D.
SUMMARY
Two patients,
ages 14 and 18, with congenital left ventricular-right atrial communication through a defect
in the tricuspid valve were studied by echocardiography. Proof was obtained by angiocardiography and surgery in one and ultrasonic contrast injection and angiocardiography in the other. Both presented clinically as
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
uncomplicated ventricular septal defects. Echocardiography consistently demonstrated a high frequency,
low amplitude flutter of the tricuspid valve in systole and none in diastole. Following surgical correction of
the defect in one patient, there was complete disappearance of the systolic flutter. Systolic flutter has not
been observed with tricuspid incompetence nor with other forms of ventricular septal defects. Fistulous
communication from the aorta to the right atrium just above the tricuspid valve did not demonstrate systolic
flutter in one patient studied. Tricuspid valve systolic flutter appears to be caused by the passage of the left
ventricular jet of blood into the right atrium through a defect in the tricuspid valve. Echocardiographic
study of the tricuspid valve is of value in the recognition of the congenital left ventricular-right atrial communication.
Additional Indexing Words:
Tricuspid valve systolic flutter
Aorto-right atrial fistula
Tricuspid incompetence
Tricuspid valve prolapse
Atrial septum
Mitral valve systolic flutter
beam oscilloscope operating as a slave. Routine echocardiographic studies of the mitral, aortic and pulmonary
valves were obtained. The tricuspid valve was recorded by
directing the ultrasonic beam medially and inferiorly from
the aortic valve recording position as well as by angling the
beam medially and slightly inferiorly from the mitral valve.
VENTRICULAR SEPTAL DEFECTS which permit
communication between the left ventricle and
the right atrium are unusual but have recently been
recognized with increasing frequency. The diagnosis
is rarely made clinically and the true nature of the
defect is usually not established until catheterization
or surgery.1' 2 From the surgical point of view, some of
these defects can be repaired through the right atrium
and ventriculotomy can thus be avoided.3 It would be
useful if a noninvasive, nontraumatic technique such
as echocardiography could contribute to the diagnosis
of this condition. The purpose of this report is to
describe characteristic echocardiographic findings in
two patients who presented with this entity.
Case Reports
Case 1
This 14-year-old asymptomatic white female had been
followed since childhood with a murmur suggestive of ventricular septal defect. Physical examination showed a well
developed and well nourished child. A systolic thrill was
palpable over the precordium in the 5th intercostal space
along the left sternal border. A grade III-IV/VI pansystolic
murmur was audible over the entire precordium, loudest at
the left sternal border. The pulmonary component of the
second heart sound was slightly accentuated. The electrocardiogram was consistent with left ventricular hypertrophy. Fluoroscopy showed a moderately enlarged heart
with some increase in the pulmonary vascularity.
Echocardiographic recordings of the mitral, aortic and
pulmonic valves did not show any abnormalities. The ventricular septum exhibited a normal motion pattern. The
tricuspid valve showed high frequency, low amplitude oscillations of the systolic segment, present throughout systole
(fig. 1). This was a constant finding over many cardiac
cycles. The tricuspid systolic segment did not show any
other abnormality. In diastole, no flutter was visible but a
coarse undulating movement was occasionally observed.
Cardiac catheterization was performed in October 1973.
The pulmonary artery pressure was somewhat elevated
Methods
All echocardiographic examinations were performed
using a commercially available echograph (Picker) and a 2
MHz transducer. Continuous records were made on 35 mm
film by means of an oscilloscope record camera and a dualFrom the Departments of Medicine (Cardiology Unit), Radiology
and Pediatrics, University of Rochester School of Medicine and
Dentistry, Rochester, New York 14642.
Address for reprints: Navin C. Nanda, M.D., Cardiology Unit,
University of Rochester Medical School, Rochester, New York
14642.
Received July 29, 1974; revision accepted for publication October
9, 1974.
268
Circulation. Volume 51, February 1975
ULTRASOUND IN LV-RA FISTULA
==*
£5rli
~
or-
.
269
LISW.4
" M4
--:zw
v
r-
..
qh,^ -4
-WMMN**-
1
M~
TV
PRO,
rtne
W"-rn-
N-
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
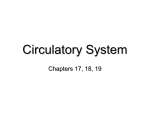
Figure 1
Tricuspid systolic fluitter (case 1). The tricuspid calve echlocardiogram shows a low amplitude, high frequiency systolic flutter
and an undulating movement in diastole. (Average frequency of
fluitter 65 cycleslsec, average amplitude 3.5 mm.) The structure
posterior to the tricuspid valve is probably the interatrial septum.
TV= tricuspid valve; PIO phonocardiogram; ECG
electrocardiogram.
=
(36/12, mean 20 mmHg). Oximetry showed a step up in the
oxygen saturation in the right atrium (82%) with a further
step up in the right ventricle (87%) and pulmonary artery
(87%). The systemic mixed venous value was 76%o. The
pulmoniic-to-systemic blood flow ratio was 3:1. Left ventricuilar angiography showed immediate shunting of the
contrast material from the left ventricle into the right ventricle and right atrium. Both chambers seemed to fill
simultaneously. The outflow tract below the crista appeared
to fill first and then the body of the right ventricle,
suggesting a membranous septal defect.
Surgery using cardiopulmonary bypass was performed on
March 12, 1974. At operation, a systolic thrill could be
palpated over the right atrium. There was enlargement of
the right ventricle with a coarse systolic thrill over it. The
left atrium and the left ventricle were also slightly enlarged.
The septal leaflet of the tricuspid valve was fused to some
extent to the underlying ventricular septum. The anterior
leaflet was free but its distal two thirds was thickened and
scarred. The posterior leaflet was essentially normal. The
ventricular septal defect was approximately 8 mm at its
greatest diameter. There was thick scar tissue about it,
probably caused by trauma produced by the jet of blood.
The defect was closed with horizontal mattress sutures on
teflon pledgets through the right atrium, and ventriculotomy was not performed. The postoperative course of
the patient was uneventful except for postpericardiotomy
syndrome characterized by a moderately large pericardial
effusion.
Postoperative tricuspid valve echograms showed complete absence of the systolic flutter (fig. 2).
Case 2
This 1 8year-old asymptomatic white male had been
followed since the age of five when a clinical diagnosis of a
Circutlation, Voluime 5/ February 197.5
Figure 2
Postoperative tricuispid calve echocardiogram (case 1). Note the
absence of systolic flutter. TV = trncuispid valve; PHO = phonocardiogram; ECG = electrocardiogramn.
small ventricular septal defect was made. Physical examination during the present visit to the clinic revealed a well
developed young man in no obvious distress. The apex beat
was in the mid clavicular line in the 5th intercostal space
and was somewhat sustained. The second heart sound
showed physiological splitting. A grade III/VI pansystolic
murmur was heard best along the left sternal edge in the 3rd
and 4th intercostal spaces and it radiated to the apex as well
as, to some extent, to the base. No diastolic murmur and no
gallops were heard. The electrocardiogram, which had been
normal so far, showed inverted T waves in leads 1II and aVF
as well as biphasic T waves in the left precordial leads
stuggestive of left ventricular hypertrophy. Fluoroscopy
revealed the heart size to be within normal limits. The
pulmonary vascularity was minimally increased and the left
ventricle was slightly enlarged.
Echocardiographic studies showed normal mitral and aortic valve records. No abnormality of the ventricular septum
was detected. The anterior leaflet of the tricuspid valve was
easily recorded. Fragments from the septal leaflet were also
observed. The most prominent feature was the high frequency, low amplitude vibrations of the systolic segment of
the tricuspid valve (fig. 3). There was no diastolic flutter.
At cardiac catheterization, all pressures were found to be
normal. Oximetry demonstrated increased oxygen saturation in the right atrium (83%) as compared to the mixed
venous blood (80%). There was a further step up in the oxygen saturation in the right ventricle (86%) and pulmonary
artery (86%c). The pulmonic-to-systemic blood flow ratio was
calculated to be 1.9:1. Echocardiographic studies were also
performed during cardiac catheterization (fig. 4). Mitral
valve recordings obtained during injection of indocyanine
green into the left ventricle showed dense echoes in the
right ventricle anterior to the ventricular septum confirming
the presence of a ventricular septal defect. Indocyanine
green was also injected into the left atrium during recording
of the atrial septum which was detected by placing the
transducer to the right of the sternum in the 4th intercostal
space, and directing the ultrasonic beam medially and
cephalad. A cloud of echoes appeared in the left atrium in
diastole and in the right atrium during the next ventricular
systole consistent with a communication between the left
ventricle and the right atrium. Absence of initial diastolic
270
NANDA, GRAMIAK, MANNING
TYMrs'.
g m-
PHO
ECG
Figure 3
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
(
Tric 11spid
systolic fflutter
le 1tniottstrat,e flitte,r of the
P10O=
iplho)ioccardiograoi,;
(case 2). T1w triwotsp)id ualve echWoes
syjstolic segrtent.
ECLc
TV = triwuispid calue;
el(,wocardiogr(amni
echoes in the right atritum suggested an intact atrial septutm.
Selective left ventricuilar angiography, in steep LAO,
revealed immediate shunting of the contrast material into
the right ventricle with some opacification of the right
atriuim as w ell. A repeat injection in shallow RAO showed an
immediate ptuff of regurgitanrt contrast into the right atrium
frorn the left ventricle. It was felt that the patienit had a
membranous defect ielow the crista communicating with
the right venitricle and with the right atrium, presumablv
through the septal leaflet of the tricuspid valve.
Discussion
The usefulness of echocardiographic studies of the
mitral and aortic valves in the evaluation of various
cardiovascular entities is well established.5 B The
tricuspid valve, on the other hand, has not been well
studied and has had limited clinical usefulness. This is
partly because of technical difficulties involved in its
recording. It requires steep transducer angulation and
hence high sensitivity settings for its detection. Also,
considerable time varied gain is needed to minimize
the nonstructural signals which clutter the anterior
region. Complete recordings of the tricuspid valve are
more easily obtained in young subjects and in patients
with right heart enlargement. Tricuspid valve studies
have been used in the diagnosis of tricuspid stenosis7
and Ebstein's disease.8 9 Diastolic flutter of the
tricuspid valve has been observed in pulmonary incompetence5 and is probably due to the regurgitant
jet abutting against the open leaflet. We have also
noted it in large atrial septal defects as well as in
transposition of the great vessels especially following
balloon septostomy or Blalock-Hanlon procedure,
probably related to the increased flow across the valve.
Systolic abnormalities have also been recorded in our
1
PHO
ECG
Figure 4
Ultrasonic contrast injetions iusing
inclocyaicnine
green (case 2).
pancl: Conrtrast injection irnto thle lcft atriumi in diastole
(arrow ) prodnc es dentse echoes in the right atriumn durinrg the soh
.scqn1ccit uentricnliar. systole consistent with left ventricdlar-right
1. ppcr
cotrast rnaterial irn the righlt atrilorn duiratrial comnnioinicatioi. o(0o
inig the initial cdiastole indicates absence of atn atrial septal defect.
lower panel/ (Contrast injection inlto thle left Ventricle in diastole
(arrow) shows fillinig of the left venttricuilar oIftflow tract wit/ sill)sc quen11t leakage inito the right ventricle dnring ventricular slistole
iidic'atice (f a venitricilcir septal ciefccit. tA= right atri tciri;
XS = atrial septumi; LA = leff atrioiii; fiRV = right ventricle;
VS
nentricnlar sleptiitni; M\V= mitral volic,; PI
phonocar=
cliograin; ECG
=
=
electroccirdiogram.
laboratorv (fig. 5). Sagging as well as straight downhill slopes of the trictuspid systolic segments have been
dlemonstrated in patients with right he,art clilatation
and tricuispicl incompetence. A sharp, mid to late
systolic posterior displacement of the valve similar to
that observed in the mitral valve echograms in patients with prolapsing mitral valves has also been
observed recenitlv by us and may represent tricuspid
valve prolapse (fig. 5)
The mechanism for the production of the tricuspid
valve systolic flutter noted in the two patients in the
present study is not clear. It has not been reported
previously and we have not observed it in any other
condition. It may be caused by the passage of the left
ventricular jet of blood into the right atrium through a
C'irculllationl S o12rln.5,
i5(l)brinarl 1975
ULTRASOUND IN LV-RA FISTULA
271
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
deficiency in the tricuspid valve, the margins of which
are deformed by fibrosis and fused to some extent to
the membranous septal defect. Following surgical correction of the defect in one patient (case 1), there was
complete disappearance of the systolic flutter. We
specifically studied the tricuspid valve in patients with
atrial septal defect (20 cases), ventricular septal defect
(14 cases, 4 with proven membranous defects not
associated with shunting into the right atrium),
pulmonary hypertension and tricuspid incompetence
of various etiologies (21 cases), and in 12 normal
children, but failed to find evidence of systolic flutter.
Fistulous communication from the aorta to the right
atrium just above the tricuspid valve (confirmed at
surgery) did not demonstrate tricuspid valve systolic
flutter in one patient studied by us. Systolic flutter
would thus not be expected to occur in the
supravalvar type of left ventricular-right atrial com-
TV
77.n * 17r
___,,
ccG
-
-.
#w..p..
munications in which the shunt opens into the right
atrium superior to the tricuspid valve.9 We have so far
not studied patients with cleft tricuspid valves by ultrasound. Four patients having partial atrioventricular
canal defects and cleft but not obviously deformed
mitral valves at surgery did not show echocardiographic evidence of mitral systolic flutter. It would,
therefore, appear unlikely that the presence of a simple cleft would result in systolic oscillations of an
atrioventricular valve. Thus although it is conceivable
that patients with endocardial cushion defects and
cleft tricuspid valves may exhibit the same echocardiographic findings, absence of mitral valve systolic
flutter in patients with cleft mitral valves makes this
unlikely. We have to date observed mitral systolic
flutter in only three patients, all of whom had echocardiographic findings of mitral valve prolapse and
previous subacute bacterial endocarditis (fig. 6). Thus
it would appear reasonable to suggest that the requirements for systolic flutter of the tricuspid or the
mitral valve include flow through an irregular defect
and sufficient local flexibility to produce fluttering.
Echocardiographic studies during cardiac
catheterization utilizing indocyanine green as a contrast agent have been used to validate the anatomy of
various structures observed and to verify abnormal
flows occurring with shunts or valvar regurgitation.4
In case 2, ultrasonic recordings obtained during injection of the green dye into the left side of the heart
demonstrated evidence of shunting into the right ventricle and into the right atrium together with an intact
atrial septum.
U
.r
Om
TVq
M
-' -
-'-
,
.-
Fec-
-
--
__M
PHO
1
-
--
--
1-
1- _.
-
.
M.
p
Figure 5
Of/eir systolic abtiorrrialities of the tricuspid valve. Upper panel:
Tricuispid valve echocardiogratr in a patient with/ trictuspid iiconilpeteuce duie to right heart dilatation. The systolic segments
s/to w s traiight down/tihill slopes without obvious flutter. Lower panel:
Tricutspid valve echtoc.ardiograni front a patient with typical
echlocardiograph/ic fecatures of mitral valve prolapse. The tricuispid
valve executes a sharp) posterior mtovemrient in rniidsystole raising the
possibility of (associated trictuspid valve prolapse. TV= tricuspid
valve; PI10 phonocardiograum; ECG = electrocardiograni.
=
Circtl{ationt, vohumic.51. lel)riai/ 5197,5
E
Figure 6
Mlitr(al valve systolic flitter. A magnified, highi speed (37.5 'trnt/Isecu)
recorditng of the mitral valve in a patienit witli mitral valve prolapse
whohJas had suibacutte bacterial endocarditis. The)appearance of thle
fltitter coincides with the onset of the valve prolapse. (AXveragefrequiccyt of flutter 90 cycleslsec, average amplitude 4.5 nini)
MY'
=
mitral valve; P10 phonocardiograni; S,
= clect rocardiogra nit.
soutid; ECLG
=
first heart
NANDA, GRAMIAK, MANNING
272
Although our experience is limited, it appears that
systolic flutter of the tricuspid valve is a rare echocardiographic finding which is of diagnostic value in
cases of congenital left ventricular-right atrial communication associated with a defect involving the
tricuspid valve. Systolic segments of the tricuspid
valve should be carefully studied for the presence of
tricuspid valve flutter in all patients with clinical
evidence of ventricular septal defect to exclude this
anomaly.
Acknowledgment
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
Figure 7
Schematic representation of the type of left ventricular-right atrial
communication observed in the present study.
The left ventricle is directly related to the right
atrium over an area of the membranous ventricular
septum which extends superior to the septal attachment of the tricuspid valve. Two major types of communications have been demonstrated between the left
ventricle and the right atrium. 10-2 In the first, the
defect in the membranous portion of the ventricular
septum opens directly into the right atrium above the
tricuspid valve. In the second, the defect which lies
lower in the membranous part of the septum opens
first into the right ventricle behind the septal leaflet of
the tricuspid valve and thence into the right atrium
through a second deficiency in the tricuspid valve,
usually the septal leaflet, which has, in turn, become
partially adherent to the septum (fig. 7). The shunt
may thus be either solely from the left ventricle to the
right atrium or at both ventricular and atrial levels.
Both the cases studied by us appear to belong to the
latter group.
The incidence of left ventricular-right atrial communications has been estimated to be about 0.08% of
all congenital lesions.`3 With increasing awareness of
this entity and with more refined and precise methods
of cardiac investigation by means of cardiac
catheterization and angiocardiography, further cases
have been diagnosed preoperatively and have been
successfully operated." Also, acquired defects have
been reported with increasing frequency and are due
to a multitude of etiological factors including bacterial
endocarditis, chest trauma and following replacement
of a heavily calcified mitral valve.'4
We are thankful to Dr. Paul Yu and the staff of the cardiac
catheterization laboratory for help with the ultrasonic contrast injections. We are grateful to Mrs. Frances Cook and Mrs. Adele
Khuzami for secretarial help, and Mr. David Tuttle for assistance in
the preparation of illustrations.
References
1. RIEMENSCHNEIDER TA, Moss AJ: Left ventricular-right atrial
communication. Am J Cardiol 19: 710, 1967
2. BRAUNWALD E, MORROw G: Left ventricular-right atrial
communication. Am J Med 28: 913, 1960
3. GERBODE F, HULTGREN H, MELROSE D, OSBORN J: Syndrome of
left ventricular-right atrial shunt: Successful surgical repair
of defect in five cases, with observation of bradyeardia on
closure. Ann Surg 148: 433, 1958
4. GRAMIAK R, SHAH PM, KRAMER DH: Ultrasound cardiography:
Contrast studies in anatomy and function. Radiology 92:
939, 1969
5. GRAMIAK R, SHAH PM: Cardiac ultrasonography: A review of
current applications. Radiol Clin North Am 9: 469, 1971
6. FEIGENBAUM H: Echocardiography. Philadelphia, Lea and
Febiger, 1972
7. JOYNER CR, HEY EB, JOHNSON J, REID JM: Reflected ultrasound
in the diagnosis of tricuspid stenosis. Am J Cardiol 19: 66,
1967
8. LUNDSTROM NR, EDLER I: Ultrasound cardiography in infants
and children. Acta Paediat Scand 60: 117, 1971
9. KOTLER MN, TABATZNIK B: Recognition of Ebstein's anomaly
by ultrasound technique. Circulation 44 (suppl II): 11-34,
1971
10. PERRY EL, BURCHELL HB, EDWARDS JE: Congenital communication between the left ventricle and the right atrium:
Co-existing ventricular septal defect and double tricuspid
orifice. Proc Staff Meet Mayo Clin 24: 198, 1949
11. BARCLAY RS, REID JM, COLENsA\ EN, STEVENSON JG, WELSH
TM, MCSWAN N: Communication between the left ventricle
and right atrium. Thorax 22: 473, 1967
12. TAGUCHI K, MATSUURA Y, YOSHIZAKI E, TAMURA M: Surgery of
atrioventricular septal defects with left ventricular-right
atrial shunt. Report of 23 cases. J Thorac Cardiovasc Surg
56: 265, 1968
13. LAURICHESSE J, FERRANE J, SCEBAT L, LENEGRE J: Communication entre le ventricule gauche et loreillette droite.
Arch Mal Coeur 57: 703, 1964
14. SEABRA-GOMES R, Ross DN, GONZALEZ-LAVIN L: latrogenic left
ventricular-right atrial fistula following mitral valve replacement. Thorax 28: 235, 1973
Circulation, Volume 51, February 1975
Echocardiography of the tricuspid valve in congenital left ventricular-riht atrial
communication.
N C Nanda, R Gramiak and J A Manning
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
Circulation. 1975;51:268-272
doi: 10.1161/01.CIR.51.2.268
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1975 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/51/2/268
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not
the Editorial Office. Once the online version of the published article for which permission is being
requested is located, click Request Permissions in the middle column of the Web page under Services.
Further information about this process is available in the Permissions and Rights Question and Answer
document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/