Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
2015–16 Zika virus epidemic wikipedia , lookup
Gastroenteritis wikipedia , lookup
Herpes simplex wikipedia , lookup
Cryptosporidiosis wikipedia , lookup
Ebola virus disease wikipedia , lookup
Orthohantavirus wikipedia , lookup
Sarcocystis wikipedia , lookup
Trichinosis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Influenza A virus wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Hepatitis C wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Antiviral drug wikipedia , lookup
West Nile fever wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Henipavirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
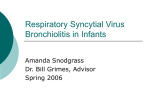
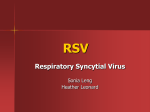
98 Infectious Disorders – Drug Targets, 2012, 12, 98-102 Respiratory Syncytial Virus Infection in Adult Populations Edward E. Walsh* and Ann R. Falsey University of Rochester School of Medicine and Dentistry, Rochester General Hospital, Rochester, New York, USA Abstract: Respiratory Syncytial Virus, generally recognized for its role as the major respiratory pathogen in newborn infants and young children, is also a significant pathogen in adults. It is a frequent cause of upper and lower respiratory illness among all age groups, although it often goes unrecognized in adults unless highly sensitive molecular diagnostic tests are used. All RSV infections in adults represent re-infection and are generally mild to moderate in severity, although persons with certain high-risk conditions are susceptible to severe disease. These include the frail elderly living at home or in long term care facilities, those with underlying chronic pulmonary disease, and the severely immunocompromised. It is estimated that between 11,000-17,000 adults die of RSV infection annually in the U.S, with ~ ten-fold more admitted to hospital with respiratory symptoms. As in infants, wheezing is often noted during RSV infections and chest radiographs are often normal despite significant lower respiratory symptoms and hypoxia. Treatment of RSV is directed at symptomatic relief, and only rarely is specific antiviral therapy recommended. Exceptions include the severely immunocompromised, in whom inhaled ribavirin has been recommended in hopes of reducing both mortality and long term pulmonary compromise, especially in lung transplant recipients. Immunity to RSV is incomplete. Although there does not appear to be a defect in humoral immunity, there is evidence that CD8+ T cell immunity may be impaired with age. Currently a vaccine for RSV is not available, and many challenges to developing a successful vaccine must be overcome. Keywords: Respiratory Syncytial Virus, Respiratory infections, Adults. INTRODUCTION Not long after a novel virus was isolated from chimpanzees in 1956, and aptly called Chimpanzee Coryza Agent, it was renamed Respiratory Syncytial Virus (RSV) reflecting the characteristic cytopathology of this virus in cell culture and in the lungs of infected infants (syncytial giant cells) and its association with respiratory illness in infants [1,2]. Frequently overlooked, however, is the fact that the first human identified as infected with this new agent was an adult handler of experimentally-infected primates. In the next few years reports by Kravetz, Johnson and Mufson, in collaboration with Chanock, described the clinical illness due to RSV in both experimentally-exposed and naturallyinfected adults [3-6]. Despite these early descriptions of illness in adults, the role of RSV in this population was largely overshadowed by its paramount importance in pediatric populations. It was not until approximately twenty years later that other investigators began to systematically describe the significant impact of RSV infection in adult populations. The high incidence and clinical significance of RSV infection in adults has been well documented in several distinct subpopulations of adults, including elderly persons residing in long term care facilities, healthy young adults, healthy elderly individuals, those with underlying cardiopulmonary disease, and in immunocompromised adults [7-13]. Each of these distinct groups display unique clinical and epidemiologic characteristics of RSV infection and present specific management problems. Undoubtedly as the population ages and the use of *Address correspondence to this author at the 1425 Portland Avenue, Rochester, New York 14621, USA; Tel: 585-922-4331; Fax: 585-922-5168; E-mail: [email protected] 2212-3989/12 $58.00+.00 immunosuppressive therapies for malignancies and inflammatory disorders increases, the overall impact of RSV infection in adults will continue to increase. LABORATORY DIAGNOSIS Unlike infants in whom primary infection is often distinctive (classically described as bronchiolitis), the clinical features of RSV infection in adults are non-specific and not readily distinguished from other common respiratory viral infections [14]. Thus, laboratory confirmation is required to be confident of a specific diagnosis of RSV infection. However, identification of RSV in adults is challenging as several studies have demonstrated that virus titers are lower in respiratory secretions and the duration of shedding shorter than in infants and young children [10,15].Typically, nasal secretions contain ~10-1000 plaque forming units (pfu) per ml of sample, which is 1000-fold lower than titers in infants. In severely ill hospitalized elderly adults viral titers, as measured by quantitative reverse transcription-polymerase chain reaction (RT-PCR) in nasal secretions, averaged 2.7 ± 1.4 pfu/ml [15]. Even in severely immunocompromised adults, Englund found that viral titers measured in cell culture ranged from <5 to 104 pfu/ml (geometric mean titer 35 pfu/ml) [16]. Due to the low levels of virus shed and the instability of viable virus, antigen detection with enzyme immunoassays or immunofluorescent tests, and cell culture are insensitive in adults, and optimal diagnosis requires RT-PCR assays or serology. In one study of 60 elderly persons diagnosed by culture, RT-PCR or serology, the sensitivity of rapid antigen detection ranged from 10-23% depending on the commercial antigen assay used [17]. In 144 RSV infected hospitalized patients, RSV was identified by culture in 39%, while RT-PCR had a sensitivity of ~73% and a specificity of 99% Fig. (1) [9,18]. Curiously, the utility of serology is age© 2012 Bentham Science Publishers Respiratory Syncytial Virus Infection in Adult Populations Infectious Disorders – Drug Targets, 2012, Vol. 12, No. 2 dependent in adults, as those >65 years of age develop more robust RSV-specific IgG responses than younger adults [19]. Although not available outside of the research laboratory, it may also be possible to diagnose infection acutely by detection of RSV-specific, antibody-secreting cells in whole blood using ELISPOT technology. Lee noted that 36 of 40 (90%) RSV RT-PCR positive adults had positive assays, although the specificity of this assay has not been evaluated [20]. # RSV Cases Method of RSV Diagnosis 200 150 100 50 0 Culture PCR Serology RSV total Fig. (1). Diagnostic yield of culture, RT-PCR and serology in 160 adults with RSV infection. EPIDEMIOLOGY, CLINICAL FEATURES AND IMPACT The number of reports describing the epidemiology and clinical impact of RSV in various adult populations has increased considerably in the past decade [21-26]. Zambon reported that of adults seen by general practitioners in the U.K. for acute respiratory illness, 20% and 15% of nasal secretions were RT-PCR positive for RSV in 45-64 and >65 year old ages groups, respectively [23]. The incidence was only slightly lower than that of influenza. During a comprehensive study of RSV infection in 294 young adults (ages 21-40), the average annual RSV attack rate was 7.4% (Falsey and Walsh, unpublished data). Although none of these young persons required hospitalization or developed severe disease, the clinical impact was significant as 10% visited a doctor and 15% were prescribed antibiotics. In another study spanning 20 years, Hall diagnosed RSV in 7% of 2960 respiratory illnesses in otherwise healthy working adults ages 18-60 [11]. Illnesses lasted 9.5 days on average and one-quarter developed lower respiratory symptoms, most notably wheezing, and 38% missed work (in contrast to 66% with influenza). Typically, nasal congestion and mild sore throat are followed several days later by lower respiratory symptoms with a productive cough. In patients with reactive airway disease wheezing often occurs. Even in previously normal young adults, RSV is associated with reactive airway disease, and pulmonary function abnormalities can be demonstrated many weeks after the illness has clinically resolved [27]. However, it is elderly adults, especially frail persons or those with underlying high-risk conditions (i.e., congestive heart failure [CHF] or chronic obstructive pulmonary disease [COPD]), that experience the most serious effects of RSV [9, 24, 28]. In a prospective cohort of 608 healthy elderly persons (mean age 75 years, each followed for two years) 46 RSV infections were identified [9]. The average illness duration was 16 days, and 32% sought medical advice via phone 99 or from a doctor. During the same study, 56 RSV infections were noted in 540 high-risk persons (mean age 70 years). Although illness duration was similar to the healthy elderly group, the use of medical care was significantly greater in the high-risk group: 51 percent called or visited the doctor, 9% visited an emergency room and 16% required hospitalization. During the four year period of the surveillance study RSV infection rates ranged from 3-7% and 4-10% in the healthy elderly and high-risk cohorts, respectively. Others have also reported that RSV is relatively common in exacerbations of COPD and asthma, although in this instance rhinovirus infections outnumber both RSV infections as well as that of the other common respiratory pathogens [29]. The incidence of RSV infection among adults hospitalized with acute respiratory symptoms has been reported by a number of investigators [9, 25, 26, 28, 30, 31]. In two of the larger studies the incidence of RSV during the winter ranged from 4.4 to 9.5% [9, 31]. Overall, RSV infection rates were only slightly lower than those for influenza and mortality was similar at 7-8%. Using statistical methods, Thompson estimated that 11,000 elderly persons die annually of RSV in the U.S., a number similar to that derived from prospective estimates based on virus-specific diagnosis [9,26]. Recent estimates using similar methodology suggest that RSVrelated hospitalizations in adults above age 50 are ~40% of those estimated for influenza [25]. Upper respiratory signs and symptoms and wheezing were common features of RSV infection in hospitalized persons [14]. Compared to patients with influenza, adults hospitalized with RSV have less fever and more frequent rhinorrhea, wheezing and dyspnea, yet in individual patients the two illnesses are indistinguishable [14]. The chest radiographic findings in RSV infected adults, even among severely ill hospitalized persons, are generally unimpressive [14]. Approximately half are clear or unchanged, while the rest generally reveal minimal basal atelectesis or small infiltrates. RSV outbreaks have long been reported among elderly residents living in congregate settings such as nursing homes and adult day care facilities [7, 32-37]. Illness is often severe in this population, with hospitalization and other morbidity due to respiratory failure noted in 10-20%. The incidence of RSV infection reported is variable, and likely dependent upon the method of diagnosis. Studies using serology or RTPCR are more apt to measure incidence rates accurately [7, 34]. An advantage of RT-PCR is that it does not underestimate incidence due to failure to obtain convalescent serum samples from patients who die. Although clinical manifestations are similar to those described in community dwelling elderly, with relatively minimal fever and high frequency of wheezing, the illness is often mistaken for influenza outbreaks unless specific viral diagnostic tests are performed. Transmission of RSV in these hospital settings appears to require close contact as infections tend to cluster on certain floors in the hospital, suggesting patient-to-patient spread by younger health care workers or by direct contact between residents. Adults with severe immunodeficiency are at particular risk of severe RSV infections [12, 13, 38-44]. A number of 100 Infectious Disorders – Drug Targets, 2012, Vol. 12, No. 2 Walsh and Falsey investigators have described the impact of RSV in patients with leukemia, hematopoietic stem cell transplant (HSCT) recipients, and solid organ transplant patients. Infection usually begins with typical upper respiratory symptoms, but in a significant number, progresses to lower respiratory disease, with mortality rates ranging from 30-70% depending upon the study. Infection is most serious in HSCT recipients during the pre-engraftment period. Illness is characterized by radiographic sinusitis in many patients, and this is a useful clue to distinguish RSV from cytomegalovirus infection [43]. In this report 6 of 8 (75%) of bone marrow transplant recipients with RSV pneumonia also had radiographic sinusitis, while reports of CMV sinusitis are rare in this population. In addition to the acute morbidity and mortality, RSV can lead to long-term detrimental effects on pulmonary function [45-47]. Attention to infection control measures is important in transplant centers, and have been demonstrated to limit RSV infections [48]. There is little information regarding RSV infection in adults with HIV infection. In HIV infected infants, virus shedding is prolonged and this may be true in adults as well, although data in this regard is lacking [49]. Interestingly, influenza virus infection does not seem to be more severe in HIV infected adults. IMMUNITY AND DISEASE PATHOGENESIS IN ADULTS Immunity to RSV is incomplete and all infections in adults represent re-infection. Most adults, including the very old, have relatively high levels of serum RSV neutralizing antibody although there is an inverse correlation between both serum and nasal antibody levels and risk of infection in elderly frail and high-risk adults [50]. Mills had demonstrated a similar relationship in an experimental RSV challenge model in young adults four decades earlier, and subsequently confirmed by others [51]. In addition, high levels of serum neutralizing antibody to RSV are associated with less severe infection in elderly adults Fig. (2) [52]. However, a fully-protective level of serum antibody has not been identified. Following infection, serum antibody titers rise rapidly, consistent with an anamnestic response, but then slowly return to pre-infection levels by 16-20 months [53]. Although long lasting immunity to RSV infection seems unlikely, we have rarely observed sequential re-infection during two consecutive years in over 1000 elderly persons suggesting that recent infection does confer temporary immunity. (E Wash & A Falsey, unpublished data). The role of cellular immunity in adults, either in protection or in disease pathogenesis is unknown. Looney found an age-related decline in interferon- production by peripheral blood mononuclear cells after in vitro RSV stimulation [54]. Lee found that the ratio of RSV-stimulated CD8+ to CD4+ T cells was diminished in all adults, regardless of age, when compared to influenza stimulation, while de Bree reported that elderly adults had lower numbers of circulating RSV tetramer positive CD8+ memory cells than younger adults [55, 56]. The importance of these findings in the incomplete immunity to RSV reinfection has not been documented. The relationship of viral load to disease severity in adults has not been extensively studied, in contrast to the situation in infants. However, one report found that elderly RSVinfected, hospitalized persons who developed respiratory failure had significantly higher RSV viral load in both nasal and pulmonary secretions than hospitalized persons who did not develop respiratory failure [15]. TREATMENT AND PREVENTION Treatment of RSV infection in adults is generally supportive, with bronchodilators and inhaled corticosteroids often prescribed for wheezing especially in asthmatics or those with COPD. For those requiring hospitalization, fluids and supplemental oxygen are often prescribed. The presence of 45 No. of subjects 40 hospitalized 35 non-hospitalized 30 25 20 15 10 5 0 <8 >8-9 >9-10 >10-11 >11-12 >12-13 >13 Log 2 serum neutralizing titer Fig. (2). Distribution of serum neutralizing antibody titers in RSV infected patients who were hospitalized (gray bars) or non-hospitalized (black bars) during their infection. As shown, RSV hospitalized persons have a lower titer distribution than ambulatory RSV infected persons, suggesting that more severe RSV disease is associated with low serum neutralizing antibody. Reproduced with permission of Oxford University Press and the Infectious Diseases Society of America original publication J. Infect Dis 2004;189:233-238. Respiratory Syncytial Virus Infection in Adult Populations bacterial co-infection should be sought in those with severe illness and with infiltrates on chest radiographs, although bacterial pathogens are often not recovered. Despite the common use of antibiotics in hospitalized persons, they may not be necessary in many cases, as radiographs only rarely demonstrate consolidation suggestive of bacterial pneumonia. Among hospitalized patients with RSV, bacterial pathogens in sputum were also identified in 15%. Ribavirin, the only licensed antiviral agent for RSV infection, is rarely used in adults, even those with respiratory failure with the exception of severely immunocompromised persons. In this latter group there are no controlled trials demonstrating benefit of inhaled ribavirin in adults infected with RSV, although anecdotal reports and expert opinion suggest that early therapy prior to the onset of lower respiratory symptoms may be beneficial [45, 57]. There remains a need for an active oral treatment, especially for immunocompromised patients and high-risk elderly persons. Currently, a vaccine for adults is not available, although several approaches have been considered. Subunit purified fusion protein vaccines have been shown to be immunogenic in a high proportion of young and older adults, including those significant frailty or COPD [58, 59]. Difficulties designing large scale efficacy trials because of low attack rates have hindered progress to a licensed vaccine. Similar to influenza, live-attenuated RSV vaccines have not been immunogenic in older adults, likely in part due to partial immunity [60]. Infectious Disorders – Drug Targets, 2012, Vol. 12, No. 3 [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] CONCLUSIONS RSV infects between 3-7 percent of adults annually, affecting all age groups. Infection is especially troublesome for those with underlying cardiopulmonary disease and frail individuals, and results in a significant burden as measured by hospitalization and mortality. Illness generally goes unrecognized as clinical features are indistinct and available diagnostics are insensitive due to low virus shedding. There remains a need in certain adult populations for effective therapeutic agents and a safe and efficacious vaccine. CONFLICT OF INTEREST [17] [18] [19] [20] [21] None declared. ACKNOWLEDGEMENTS [22] None declared. [23] REFERENCES [1] [2] [3] [4] Morris, J.A.; Blount, R.E.; Savage R.E. Recovery of cytopathic agent from chimpanzees with coryza (22538). Proc. Soc. Exper. Biol. Med., 1956, 92, 544-549. Chanock, R.; Roizman, B.; Myers R. Recovery from infants with respiratory illness of a virus related to chimpanzee coryza agent (CCA). I. Isolation, properties and characterization. Am. J. Hyg., 1957, 66(3), 281-290. Chanock, R.M.; Kim, H.W.; Vargoosko, A.J.; Deleva, A.; Johnson, K.M.; Cummings, C.; Parrott, R.H. I. Virus recovery and other observations during 1960 outbreak of bronchiolitis, pneumonia, and minor respiratory diseases in children. JAMA, 1961, 176, 647-663. Johnson, K.M.; Chanock, R.M.; Rifkind, D.; Kravetz, H.; Knight V. Respiratory syncytial virus: IV. Correlation of virus shedding serologic response and illness in adult volunteers. JAMA, 1961, 176, 663-667. [24] [25] [26] 101 Johnson, K.M.; Bloom, H.H.; Mufson, M.A.; Chanock R.M. Natural reinfection of adults by respiratory syncytial virus. possible relation to mild upper respiratory disease. N. Engl. J. Med., 1962, 267, 68-72. Mufson, M.A.; Webb, P.A.; Kennedy, H.; Gill, V.; Chanock R.M. Etiology of upper-respiratory-tract illnesses among civilian adults. JAMA, 1966, 195(1), 1-7. Falsey, A.R.; Treanor, J.J.; Betts, R.F.; Walsh E.E. Viral respiratory infections in the institutionalized elderly: Clinical and epidemiologic findings. J. Am. Geriatr. Soc., 1992, 40(2), 115-119. Falsey, A.R.; McCann, R.M.; Hall, W.J.; Criddle, M.M.; Formica, M.A.; Wycoff, D.; Kolassa, J.E. The "common cold" in frail older persons: Impact of rhinovirus and coronavirus in a senior daycare center. J. Am. Geriatr. Soc., 1997, 45(6), 706-711. Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh E.E. Respiratory syncytial virus infection in elderly and high-risk adults. N. Engl. J. Med., 2005, 352(17), 1749-1759. Hall, W.J.; Hall, C.B.; Speers D.M. Respiratory syncytial virus infection in adults: Clinical, virologic, and serial pulmonary function studies. Ann. Intern. Med., 1978, 88(2), 203-205. Hall, C.B.; Long, C.E.; Schnabel K.C. Respiratory syncytial virus infections in previously healthy working adults. Clin. Infect. Dis., 2001, 33(6), 792-796. Whimbey, E.; Couch, R.B.; Englund, J.A.; Andreeff, M.; Goodrich, J.M.; Raad, I.I.; Lewis, V.; Mirza, N.; Luna, M.A.; Baxter B. Respiratory syncytial virus pneumonia in hospitalized adult patients with leukemia. Clin. Infect. Dis., 1995, 21(2), 376-379. Englund, J.A.; Anderson, L.J.; Rhame F.S. Nosocomial transmission of respiratory syncytial virus in immunocompromised adults. J. Clin. Microbiol., 1991, 29(1), 115-119. Walsh, E.E.; Peterson, D.R.; Falsey A.R. Is clinical recognition of respiratory syncytial virus infection in hospitalized elderly and high-risk adults possible? J. Infect. Dis., 2007, 195(7), 1046-1051. Duncan, C.B.; Walsh, E.E.; Peterson, D.R.; Lee, F.E.; Falsey A.R. Risk factors for respiratory failure associated with respiratory syncytial virus infection in adults. J. Infect. Dis., 2009, 200(8), 12421246. Englund, J.A.; Piedra, P.; Jewell, A.; Baxter, B.B.; Whimbey, E.; Patel K. Rapid diagnosis of respiratory syncytial virus infections in immunocompromised adults. J. Clin. Microbiol., 1996, 34(7), 1649-1653. Casiano-Colon, A.E.; Hulbert, B.B.; Mayer, T.K.; Walsh, E.E.; Falsey A.R. Lack of sensitivity of rapid antigen tests for the diagnosis of respiratory syncytial virus infection in adults. J. Clin. Virol., 2003, 28(2) 169-174. Falsey, A.R.; Formica, M.A.; Walsh E.E. Diagnosis of respiratory syncytial virus infection: Comparison of reverse transcription-PCR to viral culture and serology in adults with respiratory illness. J. Clin. Microbiol., 2002, 40(3), 817-820. Walsh, E.E.; Falsey A.R. Age related differences in humoral immune response to respiratory syncytial virus infection in adults. J. Med. Virol., 2004, 73(2), 295-299. Lee, F.E.; Falsey, A.R.; Halliley, J.L.; Sanz, I.; Walsh EE. Circulating antibody-secreting cells during acute respiratory syncytial virus infection in adults. J. Infect. Dis., 2010, 202(11), 1659-1666. Nicholson, K.G.; Kent, J.; Hammersley, V.; Cancio, E. Acute viral infections of upper respiratory tract in elderly people living in the community: Comparative, prospective, population based study of disease burden. BMJ, 1997, 315(7115), 1060-1064. Nicholson K.G. Impact of influenza and respiratory syncytial virus on mortality in England and Wales from January 1975 to December 1990. Epidemiol. Infect., 1996, 116, 51-63. Zambon, M.C.; Stockton, J.D.; Clewley, J.P.; Fleming D.M. Contribution of influenza and respiratory syncytial virus to community cases of influenza-like illness: An observational study. Lancet, 2001, 358, 1410-1416. Griffin, M.R.; Coffey, C.S.; Neuzil, K.M.; Mitchel E.F. Jr.; Wright, P.F.; Edwards K.M. Winter viruses: Influenza- and respiratory syncytial virus-related morbidity in chronic lung disease. Arch. Intern. Med., 2002, 162(11), 1229-1236. Mullooly, J.P.; Bridges, C.B.; Thompson, W.W.; Chen, J.; Weintraub, E.; Jackson, L.A.; Black, S.; Shay D.K. Influenza- and RSVassociated hospitalizations among adults. Vaccine, 2007, 25(5), 846-855. Thompson, W.W.; Shay, D.K.; Weintraub, E.; Brammer, L.; Cox, N.; Anderson, L.J.; Fukuda K. Mortality associated with influenza and respiratory syncytial virus in the united states. JAMA, 2003, 289(2), 179-186. 102 Infectious Disorders – Drug Targets, 2012, Vol. 12, No. 2 [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] [37] [38] [39] [40] [41] [42] [43] [44] Hall, W.J.; Hall, C.B.; Speers D.M. Respiratory syncytial virus infection in adults: Clinical, virologic, and serial pulmonary function studies. Ann. Intern. Med., 1978, 88(2), 203-205. Falsey, A.R.; Cunningham, C.K.; Barker, W.H.; Kouides, R.W.; Yeun, J.B.; Menegus, M.; Weiner, L.B.; Bonville, C.A.; Betts R.F. Respiratory syncytial virus and influenza A infections in the hospitalized elderly. J. Infect. Dis., 1995, 172(2), 389-394. De Serres, G.; Lampron, N.; La Forge, J.; Rouleau, I.; Bourbeau, J.; Weiss, K.; Barret, B.; Boivin G. Importance of viral and bacterial infections in chronic obstructive pulmonary disease exacerbations. J. Clin. Virol., 2009, 46(2), 129-133. Nicholson, K.G.; McNally, T.; Silverman, M.; Simons, P.; Stockton, J.D.; Zambon M.C. Rates of hospitalisation for influenza, respiratory syncytial virus and human metapneumovirus among infants and young children. Vaccine, 2006, 24(1), 102-108. Dowell, S.F.; Anderson, L.J.; Gary H.E.Jr.; erdman, D.D.; Plouffe, J.F.; File, T.M.; Marston, B.J.; Breiman R.F. Respiratory syncytial virus is an important cause of community-acquired lower respiratory infection among hospitalized adults. J. Infect. Dis., 1996, 174(3), 456-462. Falsey A.R. Noninfluenza respiratory virus infection in long-term care facilities. Infect. Control Hosp. Epidemiol., 1991, 12(10), 602608. Mathur, U.; Bentley, D.W.; Hall C.B. Concurrent respiratory syncytial virus and influenza A infections in the institutionalized elderly and chronically ill. Ann. Intern. Med., 1980, 93, 49-52. Caram, L.B.; Chen, J.; Taggart, E.W.; Hillyard, D.R.; She, D.; Polage, C.R.; Twersky, J.; Schmader, K.; Petti, C.A.; Woods C.W. Respiratory syncytial virus outbreak in a long-term care facility detected using reverse transcriptase polymerase chain reaction: An argument for real-time detection methods. J. Am. Geriatr. Soc., 2009, 57(3), 482-485. Drinka, P.J.; Gravenstein, S.; Krause, P.; Langer, E.H.; Barthels, L.; Dissing, M.; Shult, P.; Schilling M. Non-influenza respiratory viruses may overlap and obscure influenza activity. J. Am. Geriatr. Soc., 1999, 47(9), 1087-1093. Ellis, S.E.; Coffey, C.S.; Mitchel E.F. Jr.; Dittus, R.S.; Griffin M.R. Influenza- and respiratory syncytial virus-associated morbidity and mortality in the nursing home population. J. Am. Geriatr. Soc., 2003, 51(6), 761-767. Falsey, A.R.; McCann, R.M.; Hall, W.J.; Tanner, M.A.; Criddle, M.M.; Formica, M.A.; Irvine, C.S.; Kolassa, J.E.; Barker, W.H.; Treanor J.J. Acute respiratory tract infection in daycare centers for older persons. J. Am. Geriatr. Soc., 1995, 43, 30-36. Wendt, C.H.; Hertz M.I. Respiratory syncytial virus and parainfluenza virus infections in the immunocompromised host. Semin. Respir. Infect., 1995, 10(4), 224-231. McElhaney, J.E.; Meneilly, G.S.; Lechelt, K.E.; Beattie, B.L.; Bleackley C.R. Antibody response to whole-virus and split-virus vaccines in successful aging. Vaccine, 1993, 11(10), 1055-1060. McColl, M.D.; Corser, R.B.; Bremner, J.; Chopra R. Respiratory syncytial virus infection in adult BMT recipients: Effective therapy with short duration nebulised ribavirin. Bone Marrow Transplant, 1998, 21(4), 423-425. Mazzulli, T.; Peret, T.C.; McGeer, A.; Cann, D.; MacDonald, K.S.; Chua, R.; Erdman, D.D.; Anderson L.J. Molecular characterization of a nosocomial outbreak of human respiratory syncytial virus on an adult leukemia/lymphoma ward. J. Infect. Dis., 1999, 180(5), 1686-1689. Whimbey, E.; Champlin, R.E.; Couch, R.B.; Englund, J.A.; Goodrich, J.M.; Raad, I.; Przepiorka, D.; Lewis, V.A.; Mirza, N.; Yousuf, H.; Tarrand, J.J.; Bodey G.P. Community respiratory virus infections among hospitalized adult bone marrow transplant recipients. Clin. Infect. Dis.,1996, 22(5), 778-782. Hertz, M.I.; Englund, J.A.; Snover, D.; Bitterman, P.B.; McGlave P. Respiratory syncytial virus-induced acute lung injury in adult patients with bone marrow transplants: A clinical approach and review of the literature. Medicine, 1989, 68, 269-281. Englund, J.A.; Sullivan, C.J.; Jordan, M.C.; Dehner, L.P.; Vercellotti, G.M.; Balfour H.H. Respiratory syncytial virus infection in Received: April 18, 2011 Accepted: November 30, 2011 Walsh and Falsey [45] [46] [47] [48] [49] [50] [51] [52] [53] [54] [55] [56] [57] [58] [59] [60] immunocompromised adults. Ann. Intern. Med., 1988, 109, 203208. Boeckh M. The challenge of respiratory virus infections in hematopoietic cell transplant recipients. Br. J. Haematol., 2008,143(4), 455-467. Erard, V.; Chien, J.W.; Kim, H.W.; Nichols, W.G.; Flowers, M.E.; Martin, P.J.; Corey, L.; Boeckh M. Airflow decline after myeloablative allogeneic hematopoietic cell transplantation: The role of community respiratory viruses. J. Infect. Dis., 2006, 193(12), 16191625. Kim, Y.J.; Boeckh, M.; Englund J.A. Community respiratory virus infections in immunocompromised patients: Hematopoietic stem cell and solid organ transplant recipients, and individuals with human immunodeficiency virus infection. Semin. Respir. Crit. Care Med., 2007, 28(2), 222-242. Kassis, C.; Champlin, R.; Hachem, R.Y.; Hosing, C.; Tarrand, J.J.; Perego, C.A.; Neumann, J.L.; Raad, I.I.; Chemaly R.F. Detection and control of a nosocomial respiratory Syncytial virus outbreak in a stem cell transplantation unit: The role of Palivizumab. Biol. Blood Marrow Transplant, 2010, 16,1265-1271. Medoza-Sanchez, M.C.; Ruiz-Contreras, J.; Vivanco, J.L.; Fernandez-Carrion, F.; Baro Fernandez, M.; Ramos, J.T.; Otero, J.R.; Folgueira D. Respiratory virus infections in children with cancer or HIV infection. J. Pediatr. Hematol. Oncol., 2006, 28,154-159. Walsh, E.E.; Falsey A.R. Humoral and mucosal immunity in protection from natural respiratory syncytial virus infection in adults. J. Infect. Dis., 2004, 190(2), 373-378. Mills, J.; Van Kirk, J.; Wright, P.F.; Chanock R.M. Experimental respiratory syncytial virus infection of adults. Possible mechanisms of resistance to infection and illness. J. Immunol., 1971, 107, 123130. Walsh, E.E.; Peterson, D.R.; Falsey A.R. Risk factors for severe respiratory syncytial virus infection in elderly persons. J. Infect. Dis., 2004, 189(2), 233-238. Falsey, A.R.; Singh, H.K.; Walsh E.E. Serum antibody decay in adults following natural respiratory syncytial virus infection. J. Med. Virol., 2006, 78(11), 1493-1497. Looney, R.J.; Falsey, A.R.; Walsh, E.; Campbell D. Effect of aging on cytokine production in response to respiratory syncytial virus infection. J. Infect. Dis., 2002, 185(5), 682-685. Lee FE.; Walsh EE.; Falsey AR.; liu, N.; Liu, D.; Divekar, A.; Snyder-Cappione, J.E.; Mosmann T.R. The balance between influenza- and RSV-specific CD4 T cells secreting IL-10 or IFNgamma in young and healthy-elderly subjects. Mech. Ageing Dev., 2005, 126(11), 1223-1229. de Bree, G.J.; Heidema, J.; van Leeuwen, E.M.; van Bleek, G.M.; Jonkers, R.E.; Jansen, H.M.; van Lier, R.A.; Out T.A. Respiratory syncytial virus-specific CD8+ memory T cell responses in elderly persons. J. Infect. Dis., 2005, 191(10), 1710-1718. Boeckh, M.; Englund, J.; Li, Y.; Miller, C.; Cross, A.; Fernandez, H.; Kuypers, J.; Kim, H.; Gnann, J.; Whitley R. Randomized controlled multicenter trial of aerosolized ribavirin for respiratory syncytial virus upper respiratory tract infection in hematopoietic cell transplant recipients. Clin. Infect. Dis., 2007, 44(2), 245-249. Falsey, A.R.; Walsh E.E. Safety and immunogenicity of a respiratory syncytial virus subunit vaccine (PFP-2) in ambulatory adults over age 60. Vaccine, 1996, 14(13), 1214-1218. Falsey, A.R.; Walsh, E.E.; Capellan, J.; Gravenstein, S.; Zambon, M.; Yau, E.; Gorse, G.J.; Edelwen, R.; Hayden, F.G.; McElhaney, J.E.; Neuzil, K.M.; Nickol, K.L.; Simoes, E.A.; Wright, P.F.; Sales, V.M. Comparison of the safety and immunogenicity of 2 respiratory syncytial virus (rsv) vaccines--nonadjuvanted vaccine or vaccine adjuvanted with alum--given concomitantly with influenza vaccine to high-risk elderly individuals. J. Infect. Dis., 2008, 198(9), 1317-1326. Gonzalez, I.M.; Karron, R.A.; Eichelberger, M.; Walsh, E.E.; Delagarz, V.W.; Bennett, R.; Channock, R.M.; Murphy, B.R.; Clement-Mann, M.L.; Falsey, A.R. Evaluation of the live attenuated cpts 248/404 RSV vaccine in combination with a subunit RSV vaccine (PFP-2) in healthy young and older adults. Vaccine, 2000, 18(17), 1763-1772.