Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
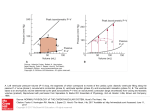
1757 Is or a Preload-Independent Measure of Isovolumetric Relaxation? Shalendra K. Varma, MD, Robert M. Owen, BA, Mark L. Smucker, MD, and Marc D. Feldman, MD Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Several studies have been performed in patients with a variety of myocardial diseases that have identified a prolongation of r. However, it is not clear whether prolongation of represents abnormal myocardial physiology or the effect of excessive load associated with a particular disease process. Accordingly, we evaluated the effect on r of an isolated decrease in preload induced by inferior vena cava occlusion before the appearance of reflex changes in six patients designated as normal by catheterization criteria. A computer-based digitization routine identified cardiac contractions in all patients early after inferior vena cava occlusion where left ventricular end-diastolic pressure decreased (18.3±6.3 to 9.3±5.8, p<0.05) while left ventric- ular systolic pressure (113.3±13.8 to 111.8+14.0, p=NS) and heart rate (66.0±10.0 to 65.9±10.3, p=NS) did not change. After this alteration in preload, no change in from baseline, as calculated by the logarithmic (TL), derivative (TD), or method of Mirsky (T1/2), was noted: TLS 47.4±6.5 to 44.6±7.6; TD, 39.3±8.1 to 39.8±8.4; T112, 33.0±+ 4.0 to 31.8+4.6; all p=NS. The baseline pressure extrapolated from isovolumetric relaxation did not change in these preload beats compared with baseline (+4.26±6.20 to -0.80±4.87, p=NS). Subsequent beats were identified where left ventricular systolic pressure showed a numeric decrease compared with baseline (113.3±13.8 to 100.8±14.3,p=NS) despite no change in heart rate (66.0±10.0 to 66.8±10.5, p=NS). The extrapolated baseline pressure decreased in these subsequent beats compared with baseline (+4.26±6.20 to -3.90±4.26, p<0.05) despite no change in r (TL, 47.4±6.5 to 41.6±8.4; TD, 39.3±8.1 to 40.8±11.1; TI,2, 33.0±4.0 to 31.7±4.2; all p=NS). Visual display of the individual natural log of left ventricular pressure versus time values used to calculate TL were consistent with exponential pressure decay as an appropriate model for isovolumetric relaxation. This study demonstrates that r is a preload independent measure of isovolumetric relaxation. (Circulation 1989;80:1757-1765) T he relaxation of isolated papillary muscle is dependent on the total load imposed on the muscle. This concept was first demonstrated by Parmley and Sonnenblickt and more recently expanded by Brutsaert et al.2 The muscle preparations used in these studies included both isometric and afterloaded isotonic contractions. Because of the nonphysiologic sequence of relaxation during an afterloaded isotonic contraction (isotonic before isometric relaxation), the load dependence of relaxation has been examined by "physiologically sequenced" relaxation. With this method the load dependence of relaxation was reconfirmed although at a temperature of 280 C.34 More recently, From the Division of Cardiology, Department of Internal Medicine, University of Virginia School of Medicine, Charlottesville, Virginia. Address for correspondence: Marc D. Feldman, MD, Division of Cardiology, Box 158, Department of Internal Medicine, School of Medicine, University of Virginia, Charlottesville, VA 22908. Received September 2, 1988; revision accepted July 27, 1989. Gaasch et al demonstrated that variable preload, with constant total load, did not produce a change in isometric relaxation.5 Relaxation of isolated papillary muscle is, therefore, independent of preload but dependent on total load. Similar observations have been extended to the intact animal heart. Karliner et al found that primary changes in afterload produced changes in the time constant of isovolumetric left ventricular pressure (LVP) decline (X-), but volume infusion did not produce such changes.6 Gaasch et al also found that modest changes in left ventricular preload did not influence i, but when volume loading was sufficient to produce an increase in aortic pressure, r increased.7 Gaasch et al recently extended this observation to an isolated increase in left ventricular preload, finding no associated change in r.5 In contrast, Raft and Glantz found that volume loading slowed r, and they concluded that this effect was a reflection of both preload and afterload.8 However, these conclusions were reached on the basis of 1758 Circulation Vol 80, No 6, December 1989 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 multiple linear regression analysis and not pure preload changes. Most data in the intact animal heart favor r being independent of preload but dependent on afterload. The present study was designed to determine whether r is a preload-independent measure of isovolumetric relaxation in patients undergoing cardiac catheterization. Several studies have been performed in patients with a variety of myocardial diseases and have identified a prolongation of 7.9-13 However, it is not clear whether prolongation of r represents abnormal myocardial physiology or the effect of excessive load associated with a particular disease process. Accordingly, we evaluated the effect on r of an isolated decrease in preload induced by inferior vena cava occlusion before the appearance of reflex changes in six patients without documentable cardiac disease by catheterization criteria. Methods Study Group Inferior vena cava occlusion with simultaneous hemodynamic monitoring was performed at the time of cardiac catheterization in eight patients. One patient developed transient atrial fibrillation, and a second had simultaneous falls in preload and afterload. These two patients were excluded from data analysis. Among the remaining six patients there were five men and one woman with an age range of 29-52 years. All medications were withheld for at least 18 hours prior to catheterization. These patients all had atypical chest pain syndromes and normal physical examinations, electrocardiograms, right and left-heart pressures, cardiac outputs, coronary arteriography, and biplane left ventriculography. All patients gave written consent to a protocol approved by the Human Investigation Committee of the University of Virginia. There were no complications as a result of this study. Cardiac Catheterization and Angiography Routine left-heart catheterization was performed from the left groin and right-heart catheterization from the right groin, leaving the latter for the inferior vena cava balloon. Right-heart catheterization was performed with a 7F flow-directed, balloontipped catheter (Critikon, Tampa, Florida). Coronary angiography was performed by the Judkins technique. Left ventriculography was performed through a pigtail catheter with biplane cine recordings. Nonionic contrast (lopamidol, Squibb, New Brunswick, New Jersey) was used to minimize the myocardial depressant effects of contrast. Pressures were measured with thoroughly flushed disposable air reference transducers (Spectramed, Oxnard, California). Recordings were inscribed by means of a Honeywell Electronics-for-Medicine VR-16 Recorder. Inferior Vena Cava Occlusion Protocol After completion of coronary angiography and left ventriculography, the deflated 8F 40-mm occlusion balloon catheter (OBW 40/8/2/100, Mansfield Scientific, Mansfield, Massachusetts) was introduced percutaneously into the right femoral vein, positioned in the right atrium over an 0.035-in. guidewire, and inflated. A 7F micromanometer pigtail catheter was subsequently introduced into the left ventricle and balanced. Analog data from the electrocardiogram (ECG), micromanometer LVP, and on-line dP/dt were stored on a nine-channel cassette FM recorder (MR-40, TEAC, Montebello, California). Thirty minutes passed between the last injection of nonionic contrast and data collection. All patients were instructed on breath-holding before the catheterization, and all data were collected at midexpiration. Analog recordings of ECG, LVP, and online dP/dt were continuously made throughout the research portion of the catheterization. The 40-mm balloon was pulled to the right atrial-inferior vena cava junction. The occlusion was maintained until left ventricular systolic pressure fell no lower than 80 mm Hg, at which point the balloon was readvanced into the right atrium. The baseline systolic LVP for these six patients was 113 + 14 mm Hg, and the nadir pressure in response to inferior vena cava occlusion was 95 + 17 mm Hg. The goal of this study was to obtain a decrease in preload and not afterload; therefore, the occlusions were often released before obtaining a true maximal fall in pressure. Six occlusions were performed in each patient, of which only one was used for data analysis. The occlusions not analyzed had either ectopy, inability of the patient to hold his or her breath at midexpiration, or no preload beats. Data Analysis The analog data recorded during the inferior vena cava occlusion were played back to the computerbased digitization routine we developed. This routine digitized each waveform and stored the data to be analyzed. By handling the analog data in this manner, we eliminated the errors for off-line hand digitization of the analog signal traces. The sampling rate for digitizing the analog signals was 1-msec intervals (1 kHz), thus providing greater accuracy than the 5 -msec (200 Hz) digitization rates previously reported.5 -8,10-11,14-16 The computer-based digitization hardware consisted of an LSI 11/23+ computer with an on-board 12-bit analog-to-digital converter (Andromeda Systems ADC1 1, Orange, California), a video display, and our software. X was calculated by three methods. The first used a plot of ln(LVP) versus time, as derived by Weiss et al (TL) 17 This approach assumed that LVP during isovolumetric relaxation decays in a monoexponential manner to zero. The second method assumed a variable asymptote to LVP decay, taking into Varma et al Preload Independence of i 1759 TABLE 1. Mean Patient Data HR (beats/min) LVSP (mm Hg) LVEDP (mm Hg), visual LVEDP (mm Hg), computer derived +dP/dt (mm Hg/sec) -dP/dt (mm Hg/sec) n TL (msec) R-TL TD (msec) R TD T1J2 (msec) PB (mm Hg) Baseline 66.0±10.0 113.3±13.8 14+2 18.3±6.3 +1,576+129 -2,027+160 46.7±6.2 47.4±6.5 -0.996±0.004 39.3±8.1 -0.862±0.038 33.0±4.0 +4.26±6.20 Preload 65.9±10.3 111.8±14.0 8±2* 9.3+5.8* +1,462±80* -1,943± 196 54.2+5.5* 44.6±7.6 -0.99 ±0.005 39.8+±8.4 -0.861±+0.041 31.8+4.6 -0.80±4.87 Total load 66.8±10.5 100.8±14.3 3±3*t 6.3±6.4*t +1,399+126* -1,808+264*t 60.4±2.0*t 41.6±8.4 -0.996±0.005 40.8±+11.1 -0.857±0.042 31.7+4.2 -3.90+4.26* *p<0.05 vs. control, tp<0.05 vs. preload. HR, heart rate; LVSP, left ventricular systolic pressure; LVEDP, left ventricular end-diastolic pressure; n, number of points used to calculate r; TL, r logarithmic; TD, 1 derivative; T112, r method of Mirsky; R, correlation coefficient; PB, pressure baseline. Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 account the effects of pleural and pericardial pressure. This method, developed by Raff and Glantz, used a plot of negative dP/dt versus LVP (TD)8 and allowed calculation of extrapolated, residual LVP, assuming diastole to be infinite in duration (PB). The preload dependence of PB was therefore also determined in this study. The third method computed the time needed for LVP to fall to one half of its value from peak negative dP/dt, using the method of Mirsky (T1/2).18 T112 is similar to TL in that the latter is the time it takes for pressure to fall from maximum negative dP/dt to 1 eth that pressure, and T1,2 uses one half instead of 1 eth. The use of T1/2 advocates not going through the exercise of the exponential fit but simply determining r from the pressure fall itself. Statistical Analysis Mean values and SDs were calculated at baseline, after preload reduction, and after total load reduction. The three groups of data were compared by analysis of variance (ANOVA). Duncan's multiple-range test was used to directly compare data at baseline versus preload reduction, baseline versus total load reduction, and preload versus total load reduction. Ap value less than 0.05 was considered significant. Results Hemodynamics The mean hemodynamic data at baseline, after reduction of only preload, and after a subsequent reduction in total load (preload and afterload) with inferior vena cava occlusion are shown in Table 1. An example of hemodynamic data from a patient is shown in Figure 1. The heart rate was not altered after a reduction in preload or after a reduction in total load (66.0+10.0 to 65.9+10.3 to 66.8+10.5 beats/min, respectively; p=NS). The systolic LVP was not altered after a reduction in preload (113.3± 13.8 to 111.8±14.0 mm Hg; p=NS). Although there was a numeric decrease in systolic LVP in the total load beats from 113.3± 13.8 to 100.8± 14.3 mm Hg, statistical significance was not achieved. The left ventricular end-diastolic pressure (LVEDP) decreased after a reduction in preload and decreased further with a reduction in total load (18.3±6.3 to 9.3 + 5.8 to 6.3 ± 6.4 mm Hg, respectively; p < 0.05). Peak positive dP/dt decreased with a reduction in preload (+1,576±129 to 1,462±80 mm Hg/sec; p<0.05). With a reduction in total load, there was a numeric decrease that did not achieve statistical significance from preload (+ 1,462 ± 80 to 1, 399 + 126 mm Hg/sec, p=NS). Peak negative dP/dt was not altered with a reduction in preload (-2,027±160 to -1,943±196 mm Hg/sec;p=NS) but decreased with a reduction in total load (-1,808±264 mm Hg/sec; p<0.05 vs. baseline and preload). Effect of Preload and Total Load Changes on r TL, TD, and T1/2 are presented in Table 1 at baseline, after a reduction of only preload, and after a subsequent reduction in total load with inferior vena cava occlusion. There were 46.7±6.2 points used to calculate r at baseline. The number of points increased in the preload and total load beats (54.2±5 .5, 60.4±2.0, respectively; p<0.05). There was no change in TL with a reduction in preload or total load (47.4±6.5 to 44.6±7.6 to 41.6±8.4 msec; respectively, p=NS). The correlation coefficient (R) for TL was similar at baseline, after a reduction in preload, and after a reduction in total load (-0.996±0.004 to -0.995±0.005 to -0.996±0.005, respectively; p= NS). There was no change in TD from baseline with a reduction of only preload and after a subsequent reduction in total load (39.3±8.1 to 39.8±8.4 to 40.8± 11.1 msec, respectively;p=NS). R for TD was similar at baseline, after a reduction in preload, and after a reduction in total load (-0.862±0.038 to 1760 A~I-1.~ P/_E- ~ IXfi Circulation Vol 80, No 6, December 1989 ~~ oJ~~~~~~~~~~~~~~~~~, OE E 0~O: E F-] HO _ Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 E' __S I I ' /__'_r_ 7 I LLJ 0 I -o0 CL 4 ., .,____ > 1 Varna et al Preload Independence of r -0.861±0.041 to -0.857±0.042, respectively, p=NS), although it was less than R for TL. There was no change in T1,, from baseline with a reduction of only preload or after a subsequent reduction in total load (33.0±4.0 to 31.8+4.6 to 31.7+4.2 msec, respectively; p=NS). Effect of Preload and Total Load Changes on PB Determination of TD provided a calculation of the extrapolated residual LVP (PB). At baseline PB was +4.26±6.20 mm Hg. After a reduction in preload with inferior vena cava occlusion, there was a numeric decrease in PB that did not achieve statistical significance (-0.80±4.87 mm Hg; p==0.20 vs. baseline). With a reduction in total load, PB did decline to -3.9±4.26 (p<0.05 vs. baseline). Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Linearity of lnP Versus Time In Figure 2 the natural log of left ventricular pressure versus time is depicted for each of the six patients during inferior vena cava occlusion. The open circles represent the baseline beat, the closed circles a reduction in preload, and the closed triangles a reduction in total load. Each symbol is a lnP versus time value digitized at a frequency of 1 kHz. In all patients, there was a parallel downward shift from baseline to preload to total load beats, consistent with no change in the slope of the ln(P) versus time relation (or TL) despite a visibly evident decrease in preload and total load. In addition, the exponential nature of the pressure decline during isovolumetric relaxation is visibly evident. Bie,xponential Pressure Decay of Negative dP/dt Versus Left Ventricular Pressure In Figure 3 negative dP/dt versus LVP is depicted for each of the six patients during inferior vena cava occlusion. The open circles represent the baseline beat, the closed circles a reduction in preload, and the closed triangles a reduction in total load. Each symbol is a negative dP/dt versus P value digitized at a frequency of 1 kHz. The preload and total load values separated from the baseline values only during the first half of isovolumetric relaxation. There was the appearance of biexponential pressure decay, as previously described by Brower et al.19 Discussion This study altered preload in six patients with inferior vena cava occlusion before the appearance of reflex increases in heart rate. After this alteration in preload, no change was noted in r as calculated by the logarithmic, derivative, or method of Mirsky. Although there was a decreasing trend for PB, statistical significance was not achieved. Subsequent beats were also identified where systolic LVP decreased although without reaching statistical significance. r calculated by the three methods above still did not change, but PB decreased. Visual display of the individual ln of LVP versus time values used to calculate r by the logarithmic method were 1761 consistent with exponential pressure decay as an appropriate model for isovolumetric relaxation. A strength of this study was the ability to alter loading conditions in patients before the appearance of reflex changes without the use of an intravenous drug infusion. The technique used was transient occlusion of the inferior vena cava, popularized in the animal laboratory by Rankin and coworkers.20 However, traditional muscle mechanic studies in patients have not taken advantage of this technique but, rather, have used drug infusions to alter load. For instance, Starling et al recently demonstrated that r was a load-independent measure of isovolumetric relaxation.14 They altered load by infusing methoxamine and nitroprusside while performing atrial pacing to maintain a constant heart rate. However, their study was weakened by the cardiovascular effects of these drugs. Methoxamine is a relatively specific a,-adrenoceptor agonist. Human myocardium contains a-adrenergic receptors in both the atrium21 and the ventricle.22 Methoxamine infusion has both inotropic and chronotropic effects, mediated by increased influx of calcium through calcium channels. Scholz et al confirmed these results, demonstrating an increased magnitude of the slow inward calcium current and associated inotropic effect.23 However, a decreased rate of decay of the slow inward calcium current was also noted by these same workers. Methoxamine can also increase coronary resistance, override intrinsic coronary regulatory influences, and produce ischemia in dogs with normal coronary arteries.24 The variety of cardiovascular effects mentioned above can have opposite effects on r and explain, in part, the load independence of r demonstrated by Starling et al.14 A second strength of this study was accurate calculation of r. Several hemodynamic studies performed in both the animal and cardiac catheterization laboratories determined r by reentering handtraced LVP recordings into a computer. Human error could be introduced into the raw data before computer calculation of r. We stored analog left ventricular pressure signals on a tape recorder and, with an analog-to-digital converter, reentered the pressure signal into a computer for calculation of r. Because no human error or bias was introduced when converting the analog LVP signal to a digital format, the data were digitized every 1 msec in the current study, fivefold faster than previously reported in the literature.5-8,10,11,14-16 r was calculated from a mean of 54+8 points for the logarithmic and derivative methods. In addition to its preload independence, r may be independent of total load within a physiologic range. There have been several clinical studies of hypertrophy and ischemia equating a prolongation of myocardial relaxation (or r) with abnormal left ventricular diastolic function.9-13These studies were weakened by increased systolic LVP, LVEDP, or both imposed on the myocardium when r was 1762 Circulation Vol 80, No 6, December 1989 100 80 100O 60] 80 #1 2s.. A* 40. 0 *.* A& #2 60 L *00o0 AAOO 000 00 *0 SA* 000000 .,A aA A.0@ A 000 ALAs. 00 00 . *0 0 A&&AA %. 00 0 000 000 0 LA A 40 LA00 A, ,,, 0 .. o 00 2, A0, _0 A~ CA o 0000 A 00 AA 20 000 AAAa 000 A A@0 O0 a a, .A AA 20 0000 0 * S 000o .@0*... 0 a L @ .&& A. i CE 0-1 0 20 10 i~~~~~~ 40 30 50 60 0- cn CD) 30 20 10 70 40 50 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 60 70 60 70 60 70 IOOT IOOT 80 80' #4 #3 60 60 A A& CL 0Y) LAM& AL 00 ,0.000 40. A& 40 9000 AL & 0 0 * @00 i0 A A 0. . 00 00 0 *S &ALA 20 00 A~ ALA 20 A^a ...0 . .0 ~ ~ _ 0 00~ ~~~~0 0*0 AL 0 AL0 . A 00 . 00000 -.A 00~~~~~ . A 0000 LA 0 20 10 30 @00 0 i z O 50 40 60 0 70 20 lO 40 30 50 100 80 100T 80 0?:.5o# 60 #6 00 60 *000 ALA. AA ALA.S000 * 0o 0 oft aALA 0O 40 "^ * 0000 A A 0 &* 40 *800 AAAL A A ..ooo ^ LALA0 00 ALAso0 090 A 20 A 20 AS~~ @0 LASS~~~~,. a . .. AL ._ A 0 0000 IL 0 AL 0 00~~~~. A. . 0 10 20 30 40 50 60 70 0 lO 20 30 40 SO Time (msec) FIGURE 2. Plots of In of left ventricularpressure versus time for each ofsxpatients during inferior vena cava occlusion. o, Baseline beat; *, reduction in preload; A, reduction in total load. (See text for discuission.) prolonged. Our findings support the assumptions of the above studies that alterations in r are independent of load changes. Although the goal of the current investigation was to produce pure preload beats, total number of load beats was identified as well. No change in was noted with simultaneous r falls in systolic and diastolic LVP. To avoid a reflex increase in heart rate, the total load beats produced with inferior vena cava occlusion did not achieve a significant change in left ventricular systolic pressure from baseline (113.3±13.8 to 100.8±14.3 mm Hg), although the trend was clear. However, Varma et al Preload Independence of 0. OT -5002 - 1763 r A &hi *1 a&* 10002 -500o - Io000 8 - 1500 A 00 0Q A - 1500. 0 a oc2 A 0 * a a oJ:'0 A9 0 £ * -2000 -20001 -2500 -2500. -3000 10 , , 20 , 30 40 , , , I 50 60 70 80 A*. -3000 i -- lO 20 'Aus. A is 30 40 50 60 70 - 80 C) U) N. Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 E E OT -500t 0-Rgjo,-£ -500. - A 1500- - 'I" - 2000. a) $3 - 10001 10 a- 0. z 0 ., A% A 0 -2000. -2500A 4 10 20 ' 30 40 50 60 70 80 _ Xnnn ..O M M xi 0 - c _, *. %gi 10 20 30 40 80 AA -500 "%,~~ 1000 O5 - *6 a 8 1000 * o - 1500 - A* 1500 -2000 -2000 -2500+ -2500 10 20 30 40 50 60 70 80 -3000 0 0 1A * O :. -3000J 0 70 50 60 01 -500 - 1000- .4 -.. A - 1500. -2500, -3000 a Aa . 10 O 0 ., 4 50 60 70 80 FIGURE 3. Plots of negative dP/dt versus left ventricular pressure for each of six patients during inferior vena occlusion. o, Baseline beat; 0, reduction in preload; *, reduction in total load. (See text for discussion.) cava 0 20 30 40 Left Ventricular Pressure (mmHg) Starling et al produced greater alterations in load with drug infusions and confirmed the load independence of r in humans over a physiologic range in the cardiac catheterization laboratory.'4 The present investigation, in conjunction with the work of Starling et al, argues that given the physiologic constraints of hemodynamic studies performed in patients, is a load-independent measure of isovolumetric relaxation. r To determine the preload dependence of r, the current study decreased filling of the left ventricle, while work by Gaasch et a15 and Karliner et a16 used volume infusion. Occlusion of the inferior vena cava to alter preload was the opposite of these canine studies using volume infusion. In all of these studies, was found to be independent of preload. However, increasing preload enough to raise systolic LVP in the studies of Gaasch and Karliner did r 1764 Circulation Vol 80, No 6, December 1989 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 produce an increase in n. These studies imply that r may be dependent on preload only to the extent that changes in preload affect systolic loading. In the present study and the work of Starling et al,14 decreases in load sufficient to decrease systolic LVP did not change r. Thus, increasing as opposed to decreasing load may change the rate of isovolumetric relaxation. For instance, when load is increased, isovolumetric relaxation may be prolonged. Conversely, a decrease in load may have no effect. However, in the study of Starling, an increase in load did not prolong isovolumetric relaxation. These data must temper the notions of the type of systolic load (i.e., increasing load and prolonging r versus decreasing load and not affecting j). Unlike r, the baseline pressure (PB) extrapolated from isovolumetric relaxation, which represents a baseline to which pressure would fall if decay continued infinitely, was found to be load dependent in the present study. PB may reflect a basal level of diastolic myocardial tone, but its physiologic meaning has been unclear. Carroll et al, for instance, attached important physiologic significance to PB and believed that exercise-induced ischemic increases in PB represented an important influence of slowed isovolumetric relaxation on elevated pressures late in diastole.25 In contrast, Thompson et al did not demonstrate pacing-induced ischemic alterations in PB despite prolongation of isovolumetric relaxation and elevation of LVEDP. 15 The present study demonstrated a downward trend in PB with decreasing preload and a significant fall in PB with a fall in both preload and afterload (Table 1). Future studies in patients designed to examine physiology with PB in the cardiac catheterization laboratory will have to be tempered by the load dependence demonstrated in this study. In their original description Weiss et al believed r was a reflection of the "active cardiac relaxation system.'"17 Several investigators have since identified a prolongation in r in several disease states, including myocardial ischemia, cardiac hypertrophy secondary to essential hypertension and valvular heart disease, hypertrophic cardiomyopathy, and congestive cardiomyopathy. Grossman and coworkers, in particular, have related this prolongation in isovolumetric relaxation in part to abnormal calcium handling.9-11 The present study supports using r as a reflection of calcium handling by the myofilaments. As is visually evident in Figure 2, the plot of the ln of LVP versus time was linear for all baseline, preload, and total load beats. This exponential decay of pressure was consistent with mathematic models of calcium release from the myofilaments. Potter et al, for instance, used a numeric computer solution to display the exponential time course of calcium release from troponin and calmodulin.26 There were several limitations to this study. The absence of a change in r with a decrease in preload may be due to opposite physiologic effects pro- duced by the method chosen to alter load. Inferior vena cava occlusion, by unloading the right ventricle, may change the radius of curvature of the intraventricular septum. Resultant asynchronous relaxation of the left ventricle would prolong T.27 A simultaneous decrease in left ventricular preload, however, would be expected to decrease r according to isolated cardiac muscle studies.2 These two opposite effects might cancel one another and produce no change in r with alterations in preload, as seen in this study. A second limitation of this study was the inability of inferior vena cava occlusion to produce a statistically significant decrease in systolic LVP before the appearance of a reflex increase in heart rate. It is difficult, therefore, to reach firm conclusions regarding the total load dependence of r on the basis of this study. Third, although the patients chosen to participate in this study were normal by cardiac catheterization criteria, their baseline LVEDPs were elevated. This finding was an artifact of the computer digitization routine. The computer software was written to locate LVEDP at the peak of the R wave of the electrocardiogram. Reanalysis of LVEDP "by hand" defined by the atrial systolic deflection on the upstroke of LVP gave a mean LVEDP of 14±2 mm Hg. Finally, our results were not in conflict with the known load dependence of relaxation in isolated papillary muscle. It is an intrinsic property of cardiac muscle that the rate of relaxation is load dependent.1-4 Rather, in the intact human heart, when isolated reductions in preload are evaluated, - is found to be load independent over a relatively narrow physiologic range. Although we produced statistically significant reductions in preload, the magnitude of decrease in LVEDP was only over an approximately 6-9 mm Hg range. Therefore, when isolated reductions in preload are performed in patients, this method of assessment of isovolumetric relaxation as a variable of active muscle relaxation is not affected. In conclusion, this study has demonstrated that r is a preload-independent measure of isovolumetric relaxation. This conclusion is strengthened by the method used: altering load with inferior vena cava occlusion before the onset of reflex changes and recording pertinent analog signals on cassette tape for later "on-line" computer digitization. Unlike r the baseline pressure (PB) extrapolated from isovolumetric relaxation is load dependent. Because of the frequency of computer digitization used, this study lends support to exponential pressure decay as an appropriate mathematic model for isovolumetric relaxation. Finally, this study supports the use of i as a reflection of myocardial physiology because of its load independence. Acknowledgments This study could not have been completed without the support of the cardiac catheterization staff at the University of Virginia and the secretarial expertise of Jerry Curtis. Varma et al Preload Independence of r References Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 1. Parmley WW, Sonnenblick EH: Relation between mechanics of contraction and relaxation in mammalian cardiac muscle. Am J Physiol 1969;216:1084 2. Brutsaert DL, Rademakers FE, Sys SU: Triple control of relaxation: Implications in cardiac disease. Circulation 1984; 69:190 3. Sulman DL, Bing OHL, Mark RG, Burns SK: Physiologic loading of isolated heart muscle. Biochem Biophys Res Commun 1974;56:947 4. Wiegner AW, Bing OHL: Isometric relaxation of rat myocardium at end-systolic fiber length. Circ Res 1978;43:865 5. Gaasch WH, Carroll JD, Blaustein AS, Bing OHL: Myocardial relaxation: Effects of preload on the time course of isovolumetric relaxation. Circulation 1986;73:1037 6. Karliner JS, LeWinter MM, Mahler F, Engler R, O'Rourke RA: Pharmacologic and hemodynamic influences on the rate of isovolumetric left ventricle relaxation in the normal conscious dog. J Clin Invest 1977;60:511 7. Gaasch WH, Blaustein AS, Andrias CW, Donahue RP, Avitall B: Myocardial relaxation: II. Hemodynamic determinants of rate of left ventricular isovolumic pressure decline. Am J Physiol 1980;239(Heart Circ Physiol 8):H1 8. Raff GL, Glantz SA: Volume loading slows left ventricular isovolumic relaxation rate: Evidence of load-dependent relaxation in the intact dog heart. Circ Res 1981;48:813 9. Mann T, Goldberg S, Mudge GH Jr, Grossman W: Factors contributing to altered left ventricular diastolic properties during angina pectoris. Circulation 1979;59:14 10. Paulus WJ, Lorell BH, Craig WE, Wynne J, Murgo JP, Grossman W: Comparison of the effects of nitroprusside and nifedipine on diastolic properties in patients with hypertrophic cardiomyopathy: Altered left ventricular loading or improved muscle inactivation? JAm Coil Cardiol 1983;2:879 11. Feldman MD, Alderman JD, Aroesty JM, Royal HD, Ferguson JJ, Owen RM, Grossman W, McKay RG: Depression of systolic and diastolic myocardial reserve during atrial pacing tachycardia in patients with dilated cardiomyopathy. J Clin Invest 1988;82:1661 12. Eichhorn P, Grimm J, Koch R, Hess 0, Carroll J, Krayenbuehi HP: Left ventricular relaxation in patients with left ventricular hypertrophy secondary to aortic valve disease. Circulation 1982;65:1395 13. Shapiro LM, McKenna WJ: Left ventricular hypertrophy: Relation of structure to diastolic function in hypertension. Br Heart J 1984;51:637 1765 14. Starling MR, Montgomery DG, Mancini GBJ, Walsh RA: Load independence of the rate of isovolumic relaxation in man. Circulation 1987;76:1274 15. Thompson DS, Waldron CB, Juul SM, Naqvi N, Swanton RH, Coltart DJ, Jenkins BS, Webb-Peploe MM: Analysis of left ventricular pressure during isovolumic relaxation in coronary artery disease. Circulation 1982;65:690 16. Walsh RA, O'Rourke RA: Direct and indirect effects of calcium entry blocking agents on isovolumic left ventricular relaxation in conscious dogs. J Clin Invest 1985;75:1426 17. Weiss JL, Frederiksen JW, Weisfeldt ML: Hemodynamic determinants of the time-course of fall in canine left ventricular pressure. J Clin Invest 1976;58:751 18. Mirsky I: Assessment of diastolic function: Suggested methods and future considerations. Circulation 1984;69:836 19. Brower RW, Meij S, Serruys PW: A model of asynchronous left ventricular relaxation predicting the bi-exponential pressure decay. Cardiovasc Res 1983;17:482 20. Rankin JS, Arentzen CE, McHale PA, Ling D, Anderson RW: Viscoelastic properties of the diastolic left ventricle in the conscious dog. Circ Res 1977;41:37 21. Schumann HJ, Wagner J, Knorr A, Reidemeister JC, Sadony V, Schramm G: Demonstration in human atrial preparations of alpha-adrenoceptors mediating positive inotropic effects. Naunyn Schmiedebergs Arch Pharnacol 1978;302:333 22. Bruckner R, Meyer W, Mugge A, Schmitz W, Scholz H: a-adrenoceptor-mediated positive inotropic effect of phenylephrine in isolated human ventricular myocardium. Eur J Pharmacol 1984;99:345 23. Scholz H, Bruckner R, Mugge A, Reupcke C: Myocardial alpha-adrenoceptors and positive inotropy. J Mol Cell Cardiol 1986;18(suppl 5):79 24. Maturi MF, Green R, Donohue B, Dorsey LMA, Green MV, Bacharach SL, Vitale D, Patterson RE: Functional consequences and intracoronary localization of alpha-adrenergic stimulation of the canine coronary circulation. J Am Coll Cardiol 1986;8:885 25. Carroll JD, Hess OM, Hirzel HO, Krayenbuehl HP: Exerciseinduced ischemia: The influence of altered relaxation on early diastolic pressures. Circulation 1983;67:521 26. Potter JD, Robertson SP, Johnson JD: Magnesium and the regulation of muscle contraction. Fed Proc 1981;40:2653 27. Blaustein AS, Gaasch WH: Myocardial relaxation: VI. Effects of 3-adrenergic tone and asynchrony on LV relaxation rate. Am J Physiol 1983;244(Heart Circ Physiol 13):H417 KEY WORDS * * vena cava * occlusion Is tau a preload-independent measure of isovolumetric relaxation? S K Varma, R M Owen, M L Smucker and M D Feldman Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Circulation. 1989;80:1757-1765 doi: 10.1161/01.CIR.80.6.1757 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1989 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/80/6/1757 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/