Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
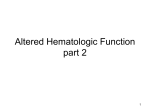
Hematopathology / HEPATOSPLENIC T-CELL LYMPHOMA IN BONE MARROW Hepatosplenic gamma/delta T-Cell Lymphoma in Bone Marrow A Sinusoidal Neoplasm With Blastic Cytologic Features Francisco Vega, MD, PhD,* L. Jeffrey Medeiros, MD, Carlos Bueso-Ramos, MD, PhD, Dan Jones, MD, PhD, Raymond Lai, MD, PhD, Rajyalakshmi Luthra, PhD, and Lynne V. Abruzzo, MD, PhD Key Words: Bone marrow; gamma/delta T-cell receptor; Hepatosplenic T-cell lymphoma; Immunophenotype Abstract We report 8 cases of hepatosplenic T-cell lymphoma (HSTCL) involving bone marrow and correlate histologic findings with disease progression. Immunophenotypic analysis demonstrated mature, aberrant gamma/delta T-cell immunophenotypes. Isochromosome 7q was identified in 4 cases; 1 case showed the t(7;14)(q34;q13). Seven of 7 cases tested had monoclonal TCR gamma gene rearrangements. The initial diagnostic bone marrow biopsy specimens were hypercellular with a frequently subtle, predominantly sinusoidal infiltrate of atypical small to medium-sized lymphoid cells. In all cases, aspirate smears at diagnosis and in subsequent specimens contained malignant cells that resembled blasts, some with fine cytoplasmic granules. With progression, the pattern of HSTCL in bone marrow biopsy specimens became increasingly interstitial, and the neoplastic cells became larger. In aspirate smears, the proportion of blasts increased. Seven patients died; 1 was lost to follow-up. Autopsy performed on 1 patient demonstrated malignant cells within vascular channels in all organs sampled, with relatively little tumor formation, resembling intravascular lymphoma at these sites. HSTCL often can be recognized in bone marrow by its unique combination of a sinusoidal pattern in core biopsy specimens and blastic cytology in aspirate smears. 410 Am J Clin Pathol 2001;116:410-419 Hepatosplenic T-cell lymphoma (HSTCL) is an uncommon form of peripheral T-cell lymphoma.1,2 In 1981 Kadin et al3 described 2 cases of an unusual T-cell lymphoma that they termed erythrophagocytic T-gamma lymphoma. These cases have many of the clinical and histologic features of HSTCL and may represent the first description of HSTCL in the literature. Patients with HSTCL usually are young men with hepatosplenomegaly, clinically significant cytopenias, and minimal or absent lymphadenopathy; they have a rapidly progressive clinical course and poor prognosis.1,2,4,5 The neoplastic cells preferentially infiltrate hepatic and bone marrow sinusoids and splenic red pulp.1,5 Immunophenotypic studies have shown that the neoplastic cells have an aberrant T-cell immunophenotype and usually have an inactive cytotoxic profile, ie, positive for TIA-1 and negative for granzyme B and perforin.5,6 Isochromosome 7q is a consistent cytogenetic abnormality.5,7-9 Because of its characteristic clinical, histologic, and immunophenotypic features, HSTCL was proposed as a provisional entity in the Revised European-American Classification of Lymphoid Neoplasms and is now recognized as a distinct clinicopathologic entity in the proposed World Health Organization classification system.10,11 Although most cases express the gamma/delta Tcell receptor (TCR), some cases reported have expressed the alpha/beta TCR.12 Bone marrow involvement in HSTCL is common,4,5 and patients often have thrombocytopenia and anemia. As a result, bone marrow biopsy and aspiration often are the first procedures performed. However, the histologic features of HSTCL in bone marrow specimens may be subtle and have not been clearly described. We report the clinicopathologic features of 8 cases of gamma/delta HSTCL involving bone marrow and emphasize the changes in histologic findings that occur with disease progression. © American Society of Clinical Pathologists Hematopathology / ORIGINAL ARTICLE Materials and Methods Six patients (cases 1-4, 7, and 8) were referred to the University of Texas M.D. Anderson Cancer Center, Houston, for evaluation and treatment. H&E-stained histologic sections and Wright-Giemsa–stained smears were prepared at the submitting institutions. Additional sections were prepared from submitted paraffin blocks of formalin-fixed tissue. Two patients (cases 5 and 6) were evaluated and treated at the University of Maryland Medical Center, Baltimore; their clinical and pathologic features have been reported previously.9 Immunohistochemical stains were performed using fixed, paraffin-embedded tissue sections, an avidin-biotinperoxidase complex method, and an automated immunostainer (Ventana-Biotech, Tucson, AZ). All tissue sections underwent heat-induced antigen retrieval. The antibodies used were specific for factor VIII–related antigen (1:400), CD45RB (1:300, leukocyte common antigen), CD79a (1:50), CD3 (1:150), CD20 (1:700, L26), and terminal deoxynucleotidyl transferase (TdT; 1:20) (DAKO, Carpinteria, CA); CD43 (1:20, Leu22), CD34 (1:20), and CD15 (1:20, LeuM1) (Becton Dickinson, San Jose, CA); CD56 (1:15; Sanbio, Uden, the Netherlands); and cytotoxic granule–associated protein (1:25, TIA-1; CoulterImmunotech, Miami, FL). Immunophenotypic analysis by flow cytometry was performed on bone marrow aspirate specimens according to standard methods. A variable panel of antibodies was used, including those reactive with CD2, CD3, CD4, CD5, CD7, CD8, CD16, CD56, CD57, CD10, CD19, CD20, CD22, CD23, CD34, TCR alpha/beta, TCR gamma/delta, TdT, and immunoglobulin kappa and lambda light chains. In situ hybridization analysis for Epstein-Barr virus was performed on bone marrow biopsy specimens using a DAKO hybridization kit (ref Y5200) according to the manufacturer’s instructions with the appropriate positive and negative controls. Cytogenetic studies were performed on direct preparations of bone marrow at the M.D. Anderson Cancer Center (cases 1, 3, 7, and 8) and the University of Maryland (cases 5 and 6) using standard techniques. Molecular genetic studies to assess for rearrangement of the TCR gamma chain gene were performed in 7 cases using polymerase chain reaction (PCR) methods and formalin-fixed, paraffin-embedded tissue. In 2 cases (cases 5 and 6), the products were detected using standard methods.9 In 5 cases (cases 1-4 and 7), the products were analyzed by high-resolution capillary electrophoresis using a 310 Genetic Analyzer (PE/Applied Biosystems, Foster City, CA), as described previously. 13 In contrast with conventional primers, each of the 4 forward primers was © American Society of Clinical Pathologists labeled at its 5' end with 1 of 4 fluorescent dyes. The forward primer for the V-gamma-I family was labeled with tetramethyl-6-rhodamine (TAMRA). The forward primers for the V-gamma-II, V-gamma-III, and V-gamma-IV families were labeled with 6-carboxyfluorescein (FAM), hexachloro-6-carboxyfluorescein (HEX), and tetrachloro-6carboxyfluorescein (TET), respectively. The labeled fluorescent dyes and the unlabeled primers were obtained from Life Technologies (Gaithersburg, MD). An aliquot (0.25 µL) of each fluorescently labeled PCR product was incubated for 10 minutes at 95°C with 12 µL of deionized formamide and 1 µL of the internal size standard (GeneScan TAMRA-500, PE/Applied Biosystems). Another 0.25-µL aliquot of each sample was incubated with 13 µL of deionized formamide without the size standard to simplify interpretation. Subsequently, samples were loaded on a DNA sequence analyzer (PRISM 310, PE/Applied Biosystems). The samples were separated using a 30-cm capillary tube that contained a performance-optimized polymer matrix (POP4, PE/Applied Biosystems). Injection was carried out for 5 seconds at 15 kV; electrophoresis was performed at 15 kV for 24 minutes at 60°C. Fluorescence data were analyzed using GeneScan 3.1 software (PE/Applied Biosystems) and Genotyper software (PE/Applied Biosystems) to determine the size and relative abundance of each fluorescently labeled product. Results Clinical Findings The clinical features are summarized in ❚Table 1❚. Six patients were male, 2 were female, and their ages ranged from 15 to 64 years (median, 37 years). The interval from onset of symptoms to diagnosis ranged from 1 to 10 months (median, 2.8 months). Physical examination at the time of diagnosis revealed splenomegaly in all patients and hepatomegaly in 6 patients. Only 1 patient (case 6) had peripheral lymphadenopathy; axillary and inguinal lymph node biopsy specimens demonstrated reactive hyperplasia. Although CBCs were not available for some patients, most were reported to have thrombocytopenia and anemia at the time of diagnosis, and only 1 patient (case 6) was reported to have slight lymphocytosis. All patients received aggressive multiagent chemotherapy after the diagnosis of HSTCL was established. One patient (case 4) experienced a complete clinical remission for 5 months, but then experienced relapse and died 13 months after diagnosis. Seven patients (cases 2-8) had progressive disease despite therapy and died 2 to 25 months after diagnosis. One patient (case 1) was lost to follow-up. Am J Clin Pathol 2001;116:410-419 411 Vega et al / HEPATOSPLENIC T-CELL LYMPHOMA IN BONE MARROW ❚Table 1❚ Clinical Findings at Diagnosis Involvement Case No./Sex/ Age (y) 1/M/64 2/M/25 3/F/27 4/M/52 5/M/15 6/M/37 7/F/43 8/M/35 * Anemia Decreased Platelet Count Hepatomegaly Splenomegaly + + + NA + + NA + + + + + + + NA + + + + NA + + – + + + + + + + + + Lymph Node – – – – – –* – – Skin Peripheral Blood – – – – – – – – + + + NA + + NA – Outcome Lost to follow-up DOD, 10 mo DOD, 5 mo DOD, 13 mo DOD, 25 mo DOD, 7 mo DOD, 12 mo DOD, 2 mo Axillary and inguinal lymph node biopsies showed reactive hyperplasia. Histologic Findings Bone marrow core biopsy sections and aspirate smears were reviewed for all cases. The initial diagnostic bone marrow specimens were reviewed in 7 of 8 cases (cases 1-3, 5-8), and specimens obtained after diagnosis were reviewed in 8 cases. The initial biopsy sections were hypercellular and contained sinusoidal and interstitial infiltrates of atypical small to medium-sized lymphoid cells ❚Image 1A❚. The pattern of infiltration at diagnosis was predominantly sinusoidal in 6 cases (cases 2, 3, and 5-8) and predominantly interstitial in 1 case (case 1). The neoplastic cells had a tendency to almost imperceptibly percolate between normal hematopoietic cells. This pattern of infiltration was frequently subtle and difficult to detect in routine H&Estained sections but was accentuated by immunohistochem- ical stains for T-cell antigens ❚Image 1B❚ . The small neoplastic cells possessed nuclei with irregular contours and coarse chromatin. The medium-sized neoplastic cells had more open chromatin and frequently small but conspicuous nucleoli. Both the small and larger cells had a moderate amount of basophilic cytoplasm with indistinct cell borders. Scattered mitotic figures were seen in all cases. The hematopoietic bone marrow was hypercellular with trilineage hyperplasia and large hyperlobated megakaryocytes in all cases. Slight dyserythropoiesis was common, but multilineage dysplasia was not observed and ringed sideroblasts were not seen. Slight to moderate plasmacytosis was seen in 5 cases (cases 2, 3, and 6-8). In addition, all cases contained conspicuous branching and tortuous blood vessels ❚Image 2❚, and hyperlobated megakaryocytes were A B ❚Image 1❚ (Case 3) A, At diagnosis the bone marrow showed a predominantly intrasinusoidal infiltrate of small cells with coarse chromatin (H&E, original magnification ×1,000). B, Antibody to CD3 accentuated the neoplastic cells (CD3, original magnification ×400). 412 Am J Clin Pathol 2001;116:410-419 © American Society of Clinical Pathologists Hematopathology / ORIGINAL ARTICLE ❚Image 2❚ (Case 1) At the time of diagnosis the bone marrow showed numerous branching and tortuous blood vessels (factor VIII–related antigen, original magnification ×200). seen within many of these vessels. Erythrophagocytosis by histiocytes was seen in 4 cases (cases 2, 3, 4, and 8). With disease progression, the degree of interstitial infiltration ❚Image 3A❚ and ❚Image 3B❚ and the percentage of medium to large cells increased ❚Image 3C❚, although a subpopulation of small atypical cells with irregular nuclear contours and coarse chromatin were still observed ❚Table 2❚. Over the disease course, mitotic figures were found more easily. Residual foci of hematopoietic cells were indistinctly demarcated from the atypical lymphoid infiltrate. Differential nucleated cell counts (100 cells) were performed on Wright-Giemsa–stained aspirate smears. In all cases, 2 populations of atypical cells were identified: small cells and medium to large cells ❚Image 4❚. The nuclei of the small cells had irregular contours, condensed chromatin, and inconspicuous nucleoli. The medium to large cells had nuclei with irregular contours, moderately dispersed chromatin, and conspicuous nucleoli. These cells had a moderate amount of basophilic cytoplasm that occasionally contained a few fine cytoplasmic granules. Over the course of disease, the percentages of neoplastic cells and blastic cells increased (Table 2). In 1 case (case 8), the blasts formed cohesive clusters in aspirate smears. CBCs were not available for all patients, but peripheral blood smears prepared at the time of diagnosis were available for review in 6 cases (cases 1-3, 5, 6, and 8). Although only 1 patient was reported to have a slight lymphocytosis (case 6), Wright-Giemsa–stained peripheral blood smears contained neoplastic cells that were cytologically similar to those seen in the bone marrow in 5 cases (cases 1-3, 5, and 6). These cells constituted from 1% to 17% of all lymphocytes. © American Society of Clinical Pathologists One patient (case 4) developed an erythematous maculopapular rash on his upper arms and shoulders 11 months after diagnosis. A skin biopsy demonstrated an infiltrate of atypical lymphoid cells within the papillary dermis and surrounding blood vessels, with marked epidermotropism ❚Image 5A❚. Atypical lymphoid cells also were seen within the lumina of small blood vessels in the superficial and deep dermis ❚Image 5B❚. The atypical lymphocytes were medium to large with dense, clumped chromatin; inconspicuous nucleoli; irregular (but not cerebriform) nuclear contours; and scant cytoplasm. The infiltrate lacked admixed inflammatory cells. An autopsy performed in case 3 revealed neoplastic cells within capillaries and dilated small to medium-sized blood vessels in liver, spleen, lymph nodes, and bone marrow most extensively, but also throughout the body ❚Image 6A❚ and ❚Image 6B❚ . These findings resembled intravascular lymphoma at these sites. Results of Immunophenotypic Analysis and In Situ Hybridization The results of immunophenotypic studies are summarized in ❚Table 3❚. In all cases, the neoplastic cells displayed a mature, aberrant, T-cell immunophenotype. In all cases tested, the neoplastic cells expressed CD2 (8/8), CD3 (8/8), TIA-1 (7/7), and TCR gamma (7/7). These neoplasms also were commonly positive for CD7 (7/8) and CD56 (7/8). Two cases were positive for CD8 (2/8), 1 was positive for CD5 (1/8), and all were negative for CD4 (0 of 8 positive). CD16 was positive in 3 of 6 cases assessed. All cases were negative for CD19, CD20, immunoglobulin light chains, and markers of myeloid differentiation. In situ hybridization for Epstein-Barr virus RNA was negative in all cases tested (6/6). The neoplastic cells that infiltrated the skin in patient 4 expressed CD3, CD56, and TIA-1, similar to the cells in the bone marrow. Cytogenetic Findings Cytogenetic analysis was performed on initial diagnostic bone marrow aspirates in 6 cases. Isochromosome 7q was detected in 4 cases (cases 1, 5, 6, and 8). In addition to the isochromosome 7q, trisomy 8 was identified in case 1, and loss of chromosomes 21 and Y and del(11)(q14) were found in case 6. In case 7, cytogenetic analysis identified the t(7;14)(q34;q13) and del(2)(q32;q37). All of these patients were mosaic, with a cytogenetically normal cell population and an abnormal population. In case 3, no apparent abnormal clone was identified. However, the bone marrow aspirate was diluted with peripheral blood and contained few neoplastic cells. Molecular Diagnostic Studies Molecular genetic studies for rearrangement of the TCR gamma chain gene were performed in 7 cases, and all Am J Clin Pathol 2001;116:410-419 413 Vega et al / HEPATOSPLENIC T-CELL LYMPHOMA IN BONE MARROW A B ❚Image 3❚ With disease progression the degree of interstitial infiltration and the percentage of medium to large cells increased. A (Case 1), Four months after diagnosis, the bone marrow biopsy specimen contained an extensive interstitial infiltrate composed of medium-sized cells with open chromatin (H&E, original magnification ×200). B (Case 1), Antibody to the cytotoxic granule-associated protein TIA-1 accentuated the interstitial infiltrate (TIA-1, original magnification ×400). C (Case 3), Six months after diagnosis, the infiltrate was still predominantly sinusoidal, but the neoplastic cells were large with open chromatin, conspicuous nucleoli, and many mitotic figures (H&E, original magnification ×1,000). C contained monoclonal rearrangements. Five cases (cases 1-4 and 7) had monoclonal rearrangements detected by highresolution GeneScan analysis ❚Figure 1❚. GeneScan analysis detected a monoallelic T-cell population that involved the Vgamma-I family in 3 patients (cases 1, 3, and 4). Two TCR gamma gene rearrangements that involved the V-gamma-II and V-gamma-IV families were detected in case 2, and 1 TCR gamma gene rearrangement that involved the Vgamma-II family was detected in case 7. Cases 5 and 6 contained monoclonal TCR gamma gene rearrangements detected by PCR coupled with GC clamped denaturing gradient gel electrophoresis, as reported previously.9 Discussion HSTCL is an uncommon type of peripheral T-cell lymphoma characterized by hepatosplenomegaly without 414 Am J Clin Pathol 2001;116:410-419 significant lymphadenopathy, with clinically significant cytopenias, and with an aggressive clinical course.1,2,4,5 A characteristic feature of HSTCL is the preferential localization of the neoplastic cells within the sinusoids of the liver and spleen.1,5 HSTCL also commonly involves the bone marrow, and different patterns of involvement have been reported, including exclusively sinusoidal,1,2,4,5,8,9,14,15 interstitial,7,16,17 and mixed sinusoidal and interstitial.18,19 The cytologic features of the previously reported cases have varied from case to case, although a monomorphic population is usually described for an individual tumor. The neoplastic cells have been reported to be small, 16 small to medium, 4,15,17,20 medium,1,2,8,9,15,18,21 or medium to large cells.7,18,19 We present the clinicopathologic features of 8 cases of HSTCL involving bone marrow and emphasize the changes that occur during progression of disease. The initial diagnostic bone marrow specimens were available for review in 7 © American Society of Clinical Pathologists Hematopathology / ORIGINAL ARTICLE ❚Table 2❚ Bone Marrow Morphologic Features Case No./Bone Marrow Biopsy Cellularity (%) Tumor Load (%)* Infiltration† Major Cell Morphologic Features (Size/Chromatin/Nucleolus) 1 Diagnosis 4 mo 90 90 60 95 I/S I/S Medium/granular/inconspicuous Medium/open/large Diagnosis 10 mo 70 35 14 62 I/S I/S Medium/open/small Medium/open/small Diagnosis 1 mo 2 mo 6 mo 75 75 85 70 20 20 30 30 I/S I/S I/S I/S Small/coarse/inconspicuous Small/coarse/inconspicuous Large/coarse and open/small Large/coarse and open/small Diagnosis 12 mo NA 95 NA 92 NA I/S NA Medium/open/small Diagnosis 23 mo 60 90 28 80 I/S I/S Small/coarse/inconspicuous Medium/open/small Diagnosis 1 mo 95 95 30 30 I/S I/S Small/coarse/inconspicuous Small/coarse/inconspicuous Diagnosis 1 mo 75 60 5 5 I/S I/S Small/coarse/inconspicuous Small/coarse/inconspicuous Diagnosis 2 mo 60 50 20 25 I/S I/S Medium/open/small Medium/open/small 2 3 4 5 6 7 8 I/S, interstitial/sinusoidal. * Based on aspirate smears. † Predominant pattern in bold. of 8 cases. The core biopsy specimens were hypercellular with a subtle infiltrate of atypical cells. The pattern of infiltration was predominantly sinusoidal in 6 cases and predominantly ❚Image 4❚ (Case 1) Small, medium, and large atypical cells were identified in all aspirate smears. The larger cells had a blastic appearance (Wright-Giemsa, original magnification ×1,000). © American Society of Clinical Pathologists interstitial in 1 case. However, interstitial infiltrates were identified in cases with a predominantly sinusoidal pattern, and a sinusoidal infiltrate was identified in a case with a predominantly interstitial pattern. Immunohistochemical stains for T-cell antigens accentuated both the sinusoidal and interstitial components. Similarly, immunohistochemical stain for factor VIII–related antigen accentuated the sinusoidal component. The discrepancy between the incidence of interstitial bone marrow involvement reported in the literature and our cases may be due to the observation that interstitial infiltration is often subtle and difficult to recognize without immunohistochemical stains early in the disease course. Thus, interstitial bone marrow infiltration by HSTCL may be more common than is currently reported in the literature. Interestingly, the neoplastic cells in HSTCL had a tendency to percolate between normal hematopoietic cells. In the initial diagnostic aspirate smears, the infiltrate was composed of atypical small to medium lymphoid cells. Predominantly small cells with occasional scattered medium-sized cells were seen in 4 cases, and predominantly medium-sized cells were seen in 3 cases. The small cells possessed nuclei with irregular contours and coarse chromatin. The medium-sized cells resembled blasts, with more open chromatin and frequently small but conspicuous nucleoli. However, in all cases, aspirate smears at the time of Am J Clin Pathol 2001;116:410-419 415 Vega et al / HEPATOSPLENIC T-CELL LYMPHOMA IN BONE MARROW A B ❚Image 5❚ (Case 4) Hepatosplenic gamma/delta T-cell lymphoma involving skin. A, The neoplastic cells showed prominent epidermotropism (H&E, original magnification ×100). B, Neoplastic cells were also seen within some dermal blood vessels (H&E, original magnification ×400). diagnosis had at least a small population of medium-sized cells that resembled blasts, some with fine cytoplasmic granules. We observed a change in the histologic and cytologic features of HSTCL over the disease course. With progression, the pattern in bone marrow biopsy specimens became increasingly interstitial, and the neoplastic cells became larger and blastic. In aspirate smears, the proportion of blastic cells increased. Similarly, the number of mitotic figures increased with time. Blastic transformation of HSTCL has been described in some reports, but almost always during the terminal phase of disease.7,8,14,16,20 In our cases, a subpopulation of blastic cells was present in the initial diagnostic specimens. These cells were identified more easily in the aspirate smears than in the core biopsy specimens. Although the increasing number of blastic cells raises the possibility of a secondary acute leukemia, the immunophenotype of the neoplastic cells was unchanged or very similar over time. The core biopsy sections in all cases contained conspicuous blood vessels that appeared branched and tortuous. These vessels bear some resemblance to the vessels that are A B ❚Image 6❚ (Case 3) Autopsy examination revealed extensive intravascular involvement by lymphoma throughout the body, including brain (A, H&E, original magnification ×400) and lung (B, H&E, original magnification ×200). 416 Am J Clin Pathol 2001;116:410-419 © American Society of Clinical Pathologists Hematopathology / ORIGINAL ARTICLE ❚Table 3❚ Immunophenotypic Findings Case No. CD2 CD3 CD4 CD5 CD7 CD8 CD16 CD56 CD57 CD19 CD20 CD25 CD34 CD52 CD38 TCR gamma/delta TCR alpha/beta TdT TIA-1† 1 2 3 4 5 6 7 8 + + – – + – – + – – – ND – – + + – – + + + – + – – + + – – – – – – + + – – + + + – – + + ND +* ND – – ND – + ND + – – + + + – – + + ND + ND – – – – + + + – – + + + – – + – + + – – – – ND ND + + – – + + + – – + – + + – – – ND ND ND ND ND ND ND + + + – – + – – – – – – – – ND + + – ND ND + + – – + – – + – – – ND ND ND ND + – – + ND, not determined; TCR, T-cell receptor; TdT, terminal deoxynucleotidyl transferase. * Positive by flow cytometric analysis and negative by immunohistochemical analysis. † By immunohistochemical analysis. seen in solid tumors and in the bone marrow of patients with chronic myeloproliferative disorders.22 The immunophenotypic findings in our cases are similar to those previously reported by other investigators.2,4,5,7 All cases expressed a mature, aberrant, gamma/delta T-cell immunophenotype. Seven of 8 cases also expressed the natural killer (NK) cell–associated antigen CD56, and 3 of 6 cases tested coexpressed CD16. Six cases were negative for both CD4 and CD8, the most common immunophenotype observed in HSTCL.2,4,5 However, 2 cases expressed CD8. Only 1 case was positive for CD5. These findings are consistent with previous reports. 4,5,7 Seven of 7 cases tested expressed the cytotoxic granule–associated protein TIA-1, a granule membrane protein whose expression is restricted to cytotoxic cells, regardless of their activation status.23,24 TIA1 expression has been reported frequently in the cases of gamma/delta T-cell lymphoma regardless of the site of localization, ie, hepatosplenic or nonhepatosplenic.5,6,25 The differential diagnosis of HSTCL includes other lymphoproliferative processes that may show sinusoidal bone marrow involvement, such as intravascular lymphoma and splenic marginal zone B-cell lymphoma.26-28 The B-cell lineage of the neoplastic cells should easily distinguish these processes from HSTCL. Rare cases of intravascular lymphoma have been reported to be of T-cell lineage.26,29-36 Most of these cases have not been evaluated for expression of the alpha/beta or gamma/delta TCR. It is conceivable that some intravascular T-cell lymphomas previously reported were examples of HSTCL. Moreover, an autopsy performed © American Society of Clinical Pathologists on one of our patients demonstrated malignant cells within small to medium-sized blood vessels in all organs, with relatively little tumor formation, resembling intravascular lymphoma. The differential diagnosis of HSTCL also includes large granular lymphocyte leukemia (LGL), aggressive NK cell leukemia/lymphoma, lymphoblastic lymphoma/leukemia, and myelodysplastic syndrome. Patients with LGL are usually older adults who often have an autoimmune disease such as rheumatoid arthritis. Two subsets of LGL have been reported, one of T-cell lineage (CD3+, CD5+[dim], TCR alpha/beta positive, CD56–) and the other of NK-cell lineage (CD3–, TCR alpha/beta negative, CD57+/–).37 The clinical setting, immunophenotype, and the presence of large intracytoplasmic granules help to distinguish LGL from HSTCL. Aggressive NK-cell leukemia/lymphoma often involves the liver and spleen, may have blastic cytologic features, and may be difficult to distinguish from HSTCL. Its clinical course is usually fulminant, with the patients dying shortly after diagnosis of multiorgan failure.38 The neoplastic cells in aggressive NK-cell leukemia/lymphoma show cytoplasmic azurophilic granules. Although they are immunophenotypically similar to HSTCL (CD2+, CD56+, CD16+), they express all cytotoxic protein markers (granzyme B and perforin) and lack surface CD3 and TCR. In addition, the TCR genes are in the germline configuration.38 Precursor Tcell lymphoblastic lymphoma/leukemia also shares some of the clinicopathologic features of HSTCL. It typically occurs in older children and adolescents. The malignant cells are blasts Am J Clin Pathol 2001;116:410-419 417 Vega et al / HEPATOSPLENIC T-CELL LYMPHOMA IN BONE MARROW aspirate smears may allow recognition of HSTCL early in the disease course. Size in Base Pairs * A SS SS SS SS SS SS SS SS From the Department of Hematopathology, University of Texas M.D. Anderson Cancer Center, Houston. * * B SS SS SS SS SS SS * SS SS SS SS SS SS SS SS SS SS C V-gamma-I V-gamma-III V-gamma-II V-gamma-IV ❚Figure 1❚ T-cell receptor (TCR) gamma chain gene rearrangements were identified by high resolution GeneScan (TAMRA-500, PE/Applied Biosystems, Foster City, CA) analysis. A, Case 3 showed a monoallelic T-cell population that involved the V-gamma-I family (red). B, Case 2 displayed two TCR gamma chain gene rearrangements that involved the V-gamma-II (blue) and V-gamma-IV (green) families. C, Negative control. *, clonal peaks detected by GeneScan; SS, internal size standard. of T-cell lineage that often involve bone marrow.39 Precursor T-cell lymphoblastic lymphoma can be distinguished from HSTCL by the presence of TdT. Virtually all lymphoblastic malignant neoplasms express TdT, while HSTCLs are TdT negative. The presence of cytopenias and increased numbers of blasts in the bone marrow raises the possibility of a myelodysplastic syndrome, such as refractory anemia with excess blasts or refractory anemia with excess blasts in transformation. Cytochemical stains for myeloperoxidase and nonspecific esterase are negative in HSTCL but positive in myelodysplastic syndromes and acute myeloid leukemia. A useful feature to recognize HSTCL in bone marrow is the apparent morphologic discordance between bone marrow core biopsy sections and aspirate smears. The neoplastic cells appear less blastic in biopsy sections than in aspirate smears. In addition, the pathologic findings in HSTCL evolve over the disease course. In biopsy sections, the pattern of infiltration evolves from predominantly sinusoidal to predominantly interstitial. In aspirate smears, the percentage of larger cells and blasts increases. These observations suggest that the histologic differences between cases reported in the literature may, in part, reflect disease progression. The combination of a sinusoidal pattern in bone marrow biopsy sections and blastic cytologic features in 418 Am J Clin Pathol 2001;116:410-419 Dr Vega is a postdoctoral fellow at the University of Texas M.D. Anderson Cancer Center. He is supported by a grant from “Fundacion Pedro Barrie de la Maza,” Galicia, Spain. Address reprint requests to Dr Abruzzo: Dept of Hematopathology, Box 72, University of Texas M.D. Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030. Acknowledgments: We thank Judith Brody, MD, North Shore University Hospital, Manhasset, New York, for providing additional materials. References 1. Farcet JP, Gaulard P, Marolleau JP, et al. Hepatosplenic T-cell lymphoma: sinusal/sinusoidal localization of malignant cells expressing the T-cell receptor gamma/delta. Blood. 1990; 75:2213-2219. 2. Gaulard P, Bourquelot P, Kanavaros P, et al. Expression of the alpha/beta and gamma/delta T-cell receptors in 57 cases of peripheral T-cell lymphomas: identification of a subset of gamma/delta T-cell lymphomas. Am J Pathol. 1990;137:617628. 3. Kadin ME, Kamoun M, Lamberg J. Erythrophagocytic Tgamma lymphoma: a clinicopathologic entity resembling malignant histiocytosis. N Engl J Med. 1981;304:648-653. 4. Wong KF, Chan JK, Matutes E, et al. Hepatosplenic gamma delta T-cell lymphoma: a distinctive aggressive lymphoma type. Am J Surg Pathol. 1995;19:718-726. 5. Cooke CB, Krenacs L, Stetler-Stevenson M, et al. Hepatosplenic T-cell lymphoma: a distinct clinicopathologic entity of cytotoxic gamma/delta T-cell origin. Blood. 1996;88:42654274. 6. Boulland ML, Kanavaros P, Wechsler J, et al. Cytotoxic protein expression in natural killer cell lymphomas and in alpha/beta and gamma/delta peripheral T-cell lymphomas. J Pathol. 1997;183:432-439. 7. Wang CC, Tien HF, Lin MT, et al. Consistent presence of isochromosome 7q in hepatosplenic T gamma/delta lymphoma: a new cytogenetic-clinicopathologic entity. Genes Chromosomes Cancer. 1995;2:161-164. 8. Francois A, Lesesve JF, Stamatoullas A, et al. Hepatosplenic gamma/delta T-cell lymphoma: a report of two cases in immunocompromised patients, associated with isochromosome 7q. Am J Surg Pathol. 1997;21:781-790. 9. Alonsozana ELC, Stamberg J, Kumar D, et al. Isochromosome 7q: the primary cytogenetic abnormality in hepatosplenic gamma/delta T cell lymphoma. Leukemia. 1997;11:1367-1372. 10. Harris NL, Jaffe ES, Stein H, et al. A revised EuropeanAmerican classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group. Blood. 1994;84:1361-1392. 11. Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the clinical advisory committee meeting, Airlie House, Virginia, November 1997. J Clin Oncol. 1999;17:3835-3849. © American Society of Clinical Pathologists Hematopathology / ORIGINAL ARTICLE 12. Lai R, Larratt LM, Etches W, et al. Hepatosplenic T-cell lymphoma of alpha/beta lineage in a 16-year-old boy presenting with hemolytic anemia and thrombocytopenia. Am J Surg Pathol. 2000;24:459-463. 13. Vega F, Medeiros LJ, Jones D, et al. A novel 4-color PCR assay to assess T-cell receptor gamma gene rearrangements in lymphoproliferative lesions. Am J Clin Pathol. 2001;116:17-24. 14. Garcia-Sanchez F, Menarguez J, Cristobal E, et al. Hepatosplenic gamma-delta T-cell malignant lymphoma: report of the first case in childhood, including molecular minimal residual disease follow-up. Br J Haematol. 1995;90:943-946. 15. Charton-Bain MC, Brousset P, Bouabdallah R, et al. Variation in the histological pattern of nodal involvement by gamma/ delta T-cell lymphoma. Histopathology. 2000;36:233-239. 16. Mastovich S, Ratech H, Ware RE, et al. Hepatosplenic T-cell lymphoma: an unusual case of a gamma/delta T cell lymphoma with a blast-like transformation. Hum Pathol. 1994;25:102-108. 17. Weirich G, Sandherr M, Fellbaum C, et al. Molecular evidence of bone marrow involvement in advanced case of Tgamma/delta lymphoma with myelofibrosis. Hum Pathol. 1998;29:761-765. 18. Gaulard P, Zafrani ES, Mavier P, et al. Peripheral T-cell lymphoma presenting as predominant liver disease: a report of three cases. Hepatology. 1986;6:864-868. 19. Ohshima K, Haraoka S, Harada N, et al. Hepatosplenic gamma/delta T-cell lymphoma: relation to Epstein-Barr virus and activated cytotoxic molecules. Histopathology. 2000;36:127-135. 20. Dommann-Scherrer CC, Baumann S, Zimmermann DR, et al. Occult hepatosplenic T-gamma/delta lymphoma: value of genotypic analysis in the differential diagnosis. Virchows Arch. 1995;426:629-634. 21. Nosari A, Oreste PL, Biondi A, et al. Hepato-splenic gamma/delta T-cell lymphoma: a rare entity mimicking the hemophagocytic syndrome. Am J Hematol. 1999;60:61-65. 22. Lundberg AG, Lerner R, Sundelin P, et al. Bone marrow in polycythemia vera, chronic myelocytic leukemia, and myelofibrosis has an increased vascularity. Am J Pathol. 2000;157:15-19. 23. Medley QG, Kedersha N, O’Brien S, et al. Characterization of GMP-17, a granule membrane protein that moves to the plasma membrane of natural killer cells following target cell recognition. Proc Natl Acad Sci U S A. 1996;93:685-689. 24. Anderson P, Nagler-Anderson C, O’Brien C, et al. A monoclonal antibody reactive with a 15-kDa cytoplasmic granuleassociated protein defines a subpopulation of CD8+ T lymphocytes. J Immunol. 1990;144:574-582. 25. Arnulf B, Copie-Bergman C, Delfau-Larue MH, et al. Nonhepatosplenic gamma/delta T-cell lymphoma: a subset of cytotoxic lymphomas with mucosal or skin localization. Blood. 1998;9:1723-1731. © American Society of Clinical Pathologists 26. Sheibani K, Battifora H, Winberg CD, et al. Further evidence that “malignant angioendotheliomatosis” is an angiotropic large cell lymphoma. N Engl J Med. 1986;314:943-948. 27. Estalilla OC, Koo CH, Brynes RK, et al. Intravascular large Bcell lymphoma: a report of five cases initially diagnosed by bone marrow biopsy. Am J Clin Pathol. 1999;112:248-255. 28. Labouyrie E, Marit G, Vial JP, et al. Intrasinusoidal bone marrow involvement by splenic lymphoma with villous lymphocytes: a helpful immunohistologic feature. Mod Pathol. 1997;10:1015-1020. 29. Glass J, Hochberg FH, Miller DC. Intravascular lymphomatosis. Cancer. 1993;71:3156-3164. 30. Sepp N, Schuler G, Romani N, et al. “Intravascular lymphomatosis” (angioendotheliomatosis): evidence for a Tcell origin in two cases. Hum Pathol. 1990;21:1051-1058. 31. Au Win Y, Shek WH, Nicholls J. T-cell intravascular lymphomatosis (angiotropic large cell lymphoma): association with Epstein-Barr viral infection. Histopathology. 1997;31:563567. 32. Tateyama H, Eimoto T, Tada T, et al. Congenital angiotropic lymphoma (intravascular lymphomatosis) of the T-cell type. Cancer. 1991;67:2131-2136. 33. Lakhani SR, Hulman G, Hall JM, et al. Intravascular malignant lymphomatosis (angiotropic large-cell lymphoma): a case report with evidence for T-cell lineage with polymerase chain reaction analysis. Histopathology. 1994;25:283-286. 34. Ko YH, Han JH, Go JH, et al. Intravascular lymphomatosis: a clinicopathological study of two cases presenting as an interstitial lung disease. Histopathology. 1997;31:555-562. 35. Kanda M, Suzumiya J, Ohshima K, et al. Intravascular large cell lymphoma: clinicopathological, immuno-histochemical and molecular genetic studies. Leuk Lymphoma. 1999;34:569580. 36. Shimokawa I, Higami Y, Sakai H, et al. Intravascular malignant lymphomatosis: a case of T-cell lymphoma probably associated with human T-cell lymphotropic virus. Hum Pathol. 1991; 22:200-202. 37. Loughran T. Clonal diseases of large granular lymphocytes. Blood. 1993;82:1-14. 38. Chan JK, Sin VC, Wong KF, et al. Nonnasal lymphoma expressing the natural killer cell marker CD56: a clinicopathologic study of 49 cases of an uncommon aggressive neoplasm. Blood. 1997;89:4501-4513. 39. Nathwani BN, Diamond LW, Winberg CD, et al. Lymphoblastic lymphoma: a clinicopathologic study of 95 patients. Cancer. 1981;48:2347-2357. Am J Clin Pathol 2001;116:410-419 419