Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Cardiac surgery wikipedia , lookup
Electrocardiography wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
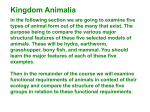
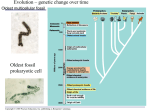
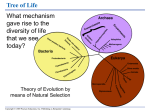
William J. Germann | Cindy L. Stanfield Principles of Human Physiology Second Edition 14 The Cardiovascular System: Cardiac Function 心血管系統:心臟的功能 PowerPoint® Lecture Slides Prepared by Cindy Stanfield, University of South Alabama Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Chapter Outline 大綱 I. Overview of the Cardiovascular System 心血管系統總覽 II. The Path of Blood Flow Through the Heart and Vasculature 在心臟及血管系統的血流路徑 III. Anatomy of the Heart 心臟的解剖構造 IV. Electrical Activity of the Heart 心臟的電生理活性 V. The Cardiac Cycle 心臟的週期 VI. Cardiac Output and Its Control 心輸出量及其控制 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. I. Overview of the Cardiovascular System 心血管系統總覽 P414 The cardiovascular system consists of three components: Heart 心臟—a muscular pump that drives the flow of blood through blood vessels Blood vessels 血管—conduits管線 through which the blood flows Blood 血液—a fluid that circulates around the body, carrying materials to and from the cells Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. The Heart 心臟 P414-415 主動脈 上腔大靜脈 右肺動脈 左肺動脈 肺動脈幹 右肺靜脈 肺動脈 半月瓣 右心房 右房室辦;三尖瓣 右心室 左肺靜脈 左心房 主動脈半月瓣 左房室瓣 腱索 心室中隔 乳頭肌 左心室 心尖 下腔大靜脈 The heart is a muscular organ whose function is to generate the force that propels blood through the blood vessels Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.1 Blood Vessels 血管 P415 Heart Arteries Arterioles Capillaries Venules Veins • Vasculature 血管系統 —the system of blood vessels that carry it from the heart to the various organs and then back to the heart again the cardiovascular system is a closed system 密閉系統 • Arteries 動脈 – relatively large, branching vessels that conduct blood away from the heart • Arterioles 小動脈 – small branching vessels with high resistance • Capillaries 微血管 – site of exchange between blood and tissue • Venules 小靜脈 – small converging vessels • Veins 靜脈 – relatively large converging vessels that conduct blood to the heart Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Blood 血液 • Erythrocytes 紅血球 – red blood cells (RBC) – • Defend body against pathogens 防禦身體對抗病源菌 Platelets 血小板 – cell fragments – • Transports oxygen and carbon dioxide 運送氧氣及二氧化碳 Leukocytes 白血球 – white blood cells (WBC) – • P416 Important in blood clotting 對血液的凝固很重要 Plasma 血漿 – fluid and solutes Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. II. The Path of Blood Flow Through the Heart and Vasculature 在心臟及血管系統的血流路徑 • Series Flow Through the Cardiovascular System 心血管系統的連續性流向 • Parallel Flow Within the Systemic or Pulmonary Circuit 體循環或肺循環內的平行性流向 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Series Flow Through the Cardiovascular System 心血管系統的連續性流向 P416-417 • Pulmonary circuit 肺循環 Figure 14.2 – Supplied by right heart – Blood vessels from heart to lungs and lungs to heart 肺靜脈 肺動脈 • Systemic circuit 體循環 主動脈 肺循環 – Supplied by left heart 下腔大靜脈 – Blood vessels from heart to systemic tissues and tissues to heart 左心房 • Exchange between blood and tissue takes place in capillaries 微血管 • Pulmonary capillaries 肺微血管 blood entering lungs = deoxygenated blood 去氧血 oxygen diffuses from tissue to blood blood leaving lungs = oxygenated blood 含氧血 右心房 右心室 左心室 體循環 • Systemic capillaries 體微血管 blood entering tissues = oxygenated blood oxygen diffuses from blood to tissue blood leaving tissues = deoxygenated blood Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Parallel Flow Patterns in the Cardiovascular System 體循環或肺循環內的平行性流向 P417-419 • Cardiovascular system = closed system 密閉系統 • Flow through systemic and pulmonary circuits are in series: left ventricle 左心室 aorta 主動脈 systemic circuit 體循環 vena cavae 下腔大靜脈 right atrium 右心房 right ventricle 右心室 pulmonary artery 肺動脈 pulmonary circuit 肺循環 pulmonary veins 肺靜脈 left atrium 左心房 left ventricle 左心室 • Aorta 主動脈 arteries 動脈 arterioles 小動脈 capillaries 微血管 venules 小靜脈 veins 靜脈 • Parallel flow 平行的流向 allows independent 獨立的 regulation of blood flow to organs & receives fully oxygenated blood • In some exceptions, blood flows in series between two capillary beds hypothalamus & anterior pituitary, intestine &liver, and kidney • The heart muscle obtains most of its nourishment 營養 from blood via the coronary arteries 冠狀動脈, which branch off the aorta near its base and run Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.3 through the heart muscle III. Anatomy of the Heart 心臟的解剖構造 • Myocardium and the Heart Wall 心肌及心臟壁 • Valves and Unidirectional Blood Flow 瓣膜及單方向的血流 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. The Location of Heart 心臟的位置 P419-420 Figure 14.4 上腔大靜脈 主動脈 右肺 肺動脈幹 左肺 心臟 肋骨 橫膈膜 心包膜 腹腔 • Located in thoracic cavity 胸腔 diaphragm 橫膈膜 separates abdominal cavity 腹腔 from thoracic cavity • Size of fist 拳頭 & weighs approximately 250 – 350 grams • Pericardium 心囊 membranous sac surrounding heart lubricates 潤滑 heart frictionInc., 摩擦 pericarditis 心囊炎 = inflammation of pericardium Copyrightdecreasing © 2005 Pearson Education, publishing as Benjamin Cummings. Myocardium and the Heart Wall 心肌及心臟壁 Three layers of the heart wall: • Endocardium 心內膜 (inner) layer of endothelial cells • Myocardium 心肌 (middle) cardiac muscle • Epicardium 心外膜 (outer) external connective tissue P420-421 Figure 14.1 The greater thickness of the muscle of the left ventricle 左心室 allows it to generate the force necessary to pump blood throughout the body Although the entire heart muscle functions as a unit, atrial 心房的 muscle and ventricular 心室的 muscle are physically anchored 固定to and separated 分隔 by a layer of fibrous connective tissue called the fibrous skeleton 纖維骨架 of the heart Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.5 Valves and Unidirectional Blood Flow 瓣膜及單方向的血流 P421 • Pressure within chambers of heart vary with heartbeat cycle 心跳週期 • Pressure difference drives blood flow 壓力差驅動血流 high pressure to low pressure • Normal direction of flow: atria 心房 ventricles 心室 arteries 動脈 • Valves 瓣膜 prevent backward flow of blood all valves (four valves) open passively based on pressure gradient • Atrioventricular (AV) valves 房室瓣 permit blood to flow from the atrium to the ventricle – – – • Right AV valve = tricuspid valve 三尖瓣 Left AV valve = bicuspid valve 二尖瓣 = mitral valve 憎帽瓣 Papillary muscles 乳突肌 and chordae tendinae 腱索 keep AV valves from everting 外翻 Semilunar valves 半月瓣 (aortic valve 主動脈瓣 & pulmonary valve 肺動脈瓣) permit blood to leave the ventricles and enter the arteries Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Action of the AV Valves 房室瓣的作用 P422 a) 當心室鬆弛,血液進入心房,推動房室瓣尖端 向下進入心室 房室瓣打開 b) 當心室收縮,血液的壓力增加,壓迫瓣膜, 使房室瓣關閉。此時乳突肌收縮,使腱索拉緊, 避免房室瓣尖端被推進心房內。 乳突肌 (收縮) 右心房 血流方向 房室瓣膜 尖端 腱索 右心室 乳突肌 (鬆弛) 房室瓣打開 (心室鬆弛) Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. 房室瓣關閉 (心室收縮) Figure 14.6 Action of the Semilunar Valves 半月瓣的作用 P423 a) 當心室收縮,血液的壓力增加,壓迫半月瓣尖端, 使半月瓣打開,允許血液流入主動脈弓及肺動脈。 b) 當心室鬆弛,進入主動脈弓及肺動脈的血液,產生 的壓力壓迫半月瓣關閉。 主動脈弓 血流方向 主動脈瓣 尖端 左心室 主動脈半月瓣打開 (心室收縮) 主動脈半月瓣關閉 (心室鬆弛) Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.7 IV. Electrical Activity of the Heart 心臟的電生理活性 • The Conduction System of the Heart 心臟的傳導系統 • Spread of Excitation Through the Heart Muscle 心肌興奮性的擴散 • The Ionic Basis of Electrical Activity in the Heart 心臟電活性的離子變化 • Electrical Activity in Cardiac Contractile Cells 心臟收縮性細胞的電活性 • Recording the Electrical Activity of the Heart with an Electrocardiogram 心電圖紀錄心臟的電活性 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. The Conduction System of the Heart 心臟的傳導系統 P422 Autorhythmicity is the ability to generate own rhythm Cardiac muscle contractions are triggered by signals originating from within the muscle itself myogenic 肌源性 The ability of the heart to generate signals that trigger its contractions on a periodic 週期的 basis—that is, to generate its own rhythm—is called autorhythmicity 自動性 There are two types of autorhythmic cells: — Pacemaker cells 節拍器(節律點)細胞 that initiate action potentials and establish the heart rhythm — Conduction fibers 傳導纖維 that transmit action potentials through the heart in a highly coordinated manner Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Pacemaker Cells of the Myocardium 心肌的節律點細胞 肌肉細胞 Figure 14.8 P422-424 間盤 胞橋體 肌小節 細胞膜 空隙聯合的通道 間盤 電流 電流 細胞膜 Pacemaker cells are concentrated primarily in two specific regions of the myocardium: the sinoatrial node 竇房節 (SA node) and the atrioventricular node 房室節 (AV node) Because pacemaker cells in the SA node have a faster inherent rate of spontaneous depolarization, and because the SA node and AV node are connected by conduction fibers, the SA node drives the depolarization of the cells in the AV node and throughout the heart, thus establishing the heart rate An action potential 動作電位 generated spontaneously 自發性 in cells of the SA node spreads to adjacent muscle cells by means of electrical current 電流 passing through gap junctions 空隙聯合 Copyright © 2005 Pearsondisks Education, Inc., publishing as Benjamin Cummings. in intercalated 間盤 Conduction Fibers of the Myocardium 心肌的傳導纖維 P423,425 Conduction fibers 傳導性纖維 are specialized to quickly conduct 快速傳導 the action potentials generated by the pacemaker cells from place to place through the myocardium 心肌細胞, thus triggering heart muscle contractions • The conduction fibers include: – Internodal pathways 結間路徑 – Bundle of His 希氏束 – Purkinje fibers 浦金氏纖維 主動脈 上腔大靜脈 竇房結 左心房 房室結 右心房 希氏束 希氏束的 左右分支 左心室 右心室 浦金氏纖維 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.9 Spread of Excitation Between Cells 細胞間興奮性的擴散 胞橋體 P423-424 • Atria 心房 contract first followed by ventricles 心室 • Coordination due to presence of gap junctions and conduction pathways • Intercalated disks 間盤 – Junctions between adjacent myocardial cells 心肌細胞之間的聯合 – Desmosomes 胞橋體 to resist mechanical stress 對抗機械性壓力 – Gap junctions 空隙聯合 for electrical coupling 電的偶合 間盤 肌小節 空隙聯合 的通道 電流 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.8 Initiation and Conduction of an Impulse During a Heartbeat 在心跳時脈衝的啟動及傳導 P424-425 The sequence of electrical events that normally triggers the heartbeat occurs as follows: an action potential is initiated in the SA node impulses travel to the AV node by way of internodal pathways bundle of His left and right bundle branches Purkinje fibers impulses travel through the rest of the myocardial cells 主動脈 上腔大靜脈 竇房結 左心房 房室結 右心房 希氏束 希氏束的 左右分支 左心室 右心室 浦金氏纖維 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.9 The impulse is conducted to cells of the AV node which transmit action potentials less rapidly than other cells of the conduction system delayed by about 0.1 second (the AV node delay) Control of Heart Beat by Pacemakers 節律點控制心跳 P424-425 Although the SA node and the AV node are both capable of generating spontaneous action potentials, the heartbeat is almost always triggered by impulses originating from the SA node — the SA node has a higher beat frequency (70 impulses/min) than the AV node (50 impulses/min) — the action potential originating in the SA node travel through the AV node cells in the AV node go into a refractory period 不反應期 If the SA node fails to fire an action potential or if it slows down dramatically the AV node will initiate action potential Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Spread of Excitation Through the Heart Muscle 興奮性在心肌的擴散 P425-426 AV node delay It allows the wave of excitation to spread completely through the atria before it reaches the ventricles Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.10 The Ionic Basis of Electrical Activity in the Heart 心臟電活性的離子變化 快速去極化 動作電 位 Pacemaker cells can fire action potentials in the absence of any external stimulus, and do so in a regular, periodic fashion because it does not have a steady resting potential The slow depolarizations or “ramps” that lead up to each action potential are referred to as pacemaker potentials During the initial spontaneous depolarization (orange), PK is decreasing and PNa is increasing during the latter spontaneous depolarization (yellow), PCa is increasing and PNa is decreasing During the rapid depolarization (green), PCa is increasing more during the repolarization phase (pink), PCa is decreasing and PK is increasing 再極化 閾值 節律點電位 (慢速去極化) Figure 14.11 L-type Ca2+ channel open PCa PK PNa K+ channel open PCa PK PCa PNa P426-427 Copyright Funny © 2005 Pearson Education, publishing Benjamin Cummings. channel open Inc., T-type Ca2+as channel open Electrical Activity in Pacemaker Cells 節律點細胞的電活性 P428 Ion concentrations in cardiac muscle cells are similar to those in other cells—the intracellular fluid is rich in K+ but poor in Na+ and Ca2+ compared to extracellular fluid thus the equilibrium potential are EK Cummings. = -94 mV, ENa= +60 mV, and Eca = +130 mV Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Electrical Activity in Cardiac Contractile Cells 心臟收縮性細胞的電活性 P428-429 The majority of ventricular muscle cells are unlike pacemaker cells in that they have stable resting potentials they also have longer-lasting action potential (250-300 msec) with a distinctive shape that can be divided into five phase – – – – – Phase 0 – increased permeability to Na+ Phase 1 – decreased permeability to Na+ Phase 2 – increased permeability to Ca2+, decreased permeability to K+ Phase 3 – increased permeability to K+, decreased permeability to Ca2+ Phase 4 – resting membrane potential 去極化 再極化 PNa Na+ channel inactivate 平原期 PCa PK L-type Ca2+ channel open 再極化 PNa PCa PK Ca2+ channel inactivate K+ channel open PK > Pca& PNa Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Voltage-gated Na+ channel open All ion channels are in the resting state Figure 14.12 Electrical Activity in Cardiac Contractile Cells 心臟收縮性細胞的電活性 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. P429 Table 14..2 Excitation-Contraction Coupling in Cardiac Contractile Cells 心臟收縮性細胞的興奮-收縮偶合 Figure 14.13 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. P429-430 Excitation-Contraction Coupling in Cardiac Contractile Cells 心臟收縮性細胞的興奮-收縮偶合 P429-430 Cardiac muscle is excited by the spread of depolarizing current through gap junctions The depolarization triggers the opening of Ca2+ channels in the plasma membrane and sarcoplasmic reticulum (SR) Calcium binds to troponin, enabling the crossbridge cycle to occur most of the Ca2+ that binds to troponin (95%) comes from the SR, with only 5% coming from the extracelluar fluid To terminate contraction, Ca2+ is pumped out of the cytosol into the sarcoplasmic reticulum and interstitial fluid Ca2+-ATPase located in the SR &plasma membrane and Na+-Ca2+ exchanger located in the plasma membrane • Properties similar to skeletal muscle – – – • T tubules Sarcoplasmic reticulum calcium Troponin-tropomyosin regulation Properties similar to smooth muscle – Gap junctions Copyright Pearson Education, Inc., publishing as Benjamin Cummings. – © 2005 Extracellular calcium Recording the Electrical Activity of the Heart with an Electrocardiogram 心電圖紀錄心臟的電性活性 P431 The electrocardiogram 心電圖 (ECG) is a noninvasive 非侵入性的 means for monitoring the electrical activity of the heart ECG recordings do not give information about mechanical problems of the heart unless those problems result from an electrical problem Electric activity generated in nervous or muscle tissue spreads through the body because body fluids function as conductors the more synchronized the activity, the larger the amplitude of signals that are recorded at a distance from the source A Dutch physiologist, Willem Einthoven, developed the technique of ECG recordings the procedure is based on an imaginary equilateral triangle surrounding the heart • ECG is a non-invasive technique used to test for clinical abnormalities in conduction of electrical activity in the heart • Distance & amplitude of spread depends on size of potentials and synchronicity of potentials from other cells • Heart electrical activity- synchronized Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Einthoven’s Triangle Lead I: LA (+) and RA (-) Lead II: LL (+) and RA (-) Lead III: LL (+) and LA (-) P431 Three electrodes 電極 are placed are placed on limbs to form an equilateral triangle 等三角 around the heart One electrode in each lead 導程 is designated as the positive electrode, the other as the negative Lead I detects the potential at the left arm (LA) minus that at the right arm (RA) Lead II detects the potential at the left leg (LL) minus that at the right arm (RA) Lead III detects the potential at the left leg (LL) minus that at the left arm (LA) Figure 14.14 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Standard ECG recording 標準的心電圖紀錄 P431-432 Figure 14.15b • P wave atrial depolarization 心房去極化 • QRS complex ventricular depolarization 心室去極化 • T wave ventricular repolarization 心室再極化 Atrial reploarization is generally not detected in an ECG recording because it occurs at the same time as the QRS complex The phases of ECG are due to action potentials traveling through the heart muscle reflects patterns of action potential firing in the entire populations of heart muscle Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Standard ECG recording 標準的心電圖紀錄 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. P431-432 Standard ECG recording 標準的心電圖紀錄 P431-432 The membrane potential in a ventricle contractile cell Ventricular action potential recorded from a single contractile cell in the ventricle ECG surface recording of the summed electrical activity of all cells Figure 14.15 • PQ segment AV nodal delay 房室結延遲 • QT segment ventricular systole 心室收縮 • TQ interval ventricular diastole 心室舒張 The P-Q or P-R interval occurs between the onset of the P wave and the onset of the QRS complex and is an estimate the time of conduction through the AV node The R-R interval is the time between the peaks of two QRS complex it represents the time between heartbeats Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. ECG Showing Various Cardiac Arrhythmias—Tachycardia & Bradycardia 心電圖紀錄不同型態的心律不整—心跳過快 & 心跳過慢 P432-433 正常 Abnormal electrical activity of heart, called cardiac arrhythmias Abnormal SA nodal firing can cause either a sinus tarchycardia, which is an abnormally fast resting heart rate (>100 beats/min), or a sinus bradycardia, which is an abnormally slow resting heart rate (<50 beats/min) 心跳過快 (T波反轉) • Sinus rhythm = rhythm generated by SA node • Abnormal Heart Rates: 心跳過慢 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. – Tachycardia- fast – Bradycardia- slow Figure 14.16 ECG Showing Various Cardiac Arrhythmias—Heat block 心電圖紀錄不同型態的心律不整—心阻斷 P432-433 Altered conduction through the AV can cause various degrees of heart block: Figure 14.16 - During first-degree heart block, conduction through the AV node is slowed causing a longer delay in AV nodal conduction (P-Q interval) - During second-degree heart block, conduction through the AV node does not always occur absence of QRS complex & T wave - During third-degree heart block, conduction through the AV node does not occur at all causing complete dissociation of atrial and ventricular contractions • 1st degree block = slowed conduction through AV node increases PQ segment & Increases delay between atrial and ventricular contraction • 2nd degree block lose 1-to-1 relationship between P wave and QRS complex & between atrial and ventricular contraction • 3rd degree block P wave independent of QRS complex & atrial and ventricular contractions are independent Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. ECG Showing Various Cardiac Arrhythmias—PAC & PVC 心電圖紀錄不同型態的心律不整—早熟性心房 & 心室收縮 P432-433 Sometimes the heart is depolarized by an electrical stimulus arising outside the normal conduction pathway If the depolarization occurs in an atrium, then a premature atrial contraction (PAC) occurs If the depolarization occurs in an ventricular, then a premature ventricular contraction (PVC) occurs PACs and PVCs are generally of little clinical significance unless they occurs at high frequencies Extra contraction • PAC = premature atrial contraction • PVC = premature ventricular Contraction Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.16 ECG Showing Various Cardiac Arrhythmias—Ventricular fibrillation P432-433 心電圖紀錄不同型態的心律不整—心室纖維顫動 Loss of coordination of electrical activity • Atrial fibrillation - weakness • Ventricular fibrillation - death within minutes More serious arrhythmias are fibrillation 纖維 顫動, which occur when the heart muscle no longer has synchronized depolarization In atrial fibrillation, atrial muscle fibers depolarize independently, so atrial contraction is inefficient in pumping blood to the ventricle weakness & lightheadedness due to decreased blood flow Ventricular fibrillation can cause death within minutes the ventricles can no longer efficiently pump the blood out to the tissues, including the brain ventricular muscle cells depolarized independently Clinicians must quickly defibrillate the ventricular muscle to keep the person alive defibrillation 去纖維化 can returning synchronous electrical activity to the heart Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.16 V. The Cardiac Cycle 心臟週期 • The Pump Cycle 幫浦週期 • Atrial and Ventricular Pressure 心房及心室壓 • Aortic Pressure 主動脈壓 • Ventricular Volume 心室體積(容積) • Heart Sounds 心音 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Cardiac Cycle 心臟週期 P433 Events associated with the flow of blood through the heart during a single complete heartbeat 1. The various phases in the pumping action of the heart, often called the pump cycle 幫浦週期 2. Periods of valve 瓣膜 opening and closure 3. Changes in atrial, ventricular, and aortic pressure 心房壓、心室壓及 主動脈壓, which reflect contraction and relaxation of the heart muscle 4. Changes in ventricular volume 心室容積, which reflect the amount of blood entering and leaving the ventricle during each heartbeat 5. The two major heart sounds 心音 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Cardiac Cycle 心臟週期 P433,435 The cycle can be divided into two major stages: — Systole 收縮期, the period of ventricular contraction — Diastole 舒張期, the period of ventricular relaxation For a heart beating at the normal resting rate of 72 beats/min (one beat every 0.8 second) most of the cardiac cycle (about 65%, 0.5 second) is spent in diastole, systole lasts only about 0.3 second This longer diastole gives the heart adequate time to fill with blood, which is essential for efficient pumping, and it also gives the heart muscle more time to relax, which helps prevent fatigue Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Pump Cycle 幫浦週期 P434 等容收縮期 射血期 心房收縮 等容舒張期 心室充血期 心室充血期 心室收縮期 心室舒張中-晚期 心室舒張早期 房室瓣 半月瓣 Diastole 舒張期 corresponds to phases 4 and 1, whereas systole 收縮期 corresponds to phases 2 and 3 Figure 14.17 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Four Phases of Pump Cycle 幫浦週期的四個分期 • Ventricular filling 心室充血期 – – – – – • Isovolumetric ventricular contraction 等容收縮期 – – – • Ventricle contracts pressure increases until it exceeds atrial pressure AV and semilunar valves closed 房室瓣及半月瓣關閉 No blood entering or exiting ventricle 沒有血液流入或流出心室 Ventricular ejection 射血期 – – – • Pressure atria > Pressure ventricles 心房壓力大於心室壓力 AV valves open 房室瓣打開 Passive phase - no atria or ventricular contraction Active phase - atria contract Blood moves from atria to ventricle 血液從心房流至心室 Pressure ventricles > Pressure arteries 心室壓力大於動脈壓力 Semilunar valves open 半月瓣打開 Blood moves from ventricle to aorta 血液從心室流至主動脈 Isovolumetric Ventricular Relaxation 等容舒張期 – Ventricle relaxes - decreases pressure pressure is less than aorta – AV and semilunar valves closed 房室瓣及半月瓣關閉 No blood Inc., entering orasexiting Copyright © 2005 – Pearson Education, publishing Benjamin ventricle Cummings. 沒有血液流入或流出心室 收 縮 期 (systole) (distole) 舒 張 期 P433-435 Atrial and Ventricular Pressure 心房及心室壓 心室充血期 等容收縮期 射血期 P435-436 等容舒張期 心室充血期 房室瓣 半月瓣 Ventricle contraction 心室壓 Ventricle relaxation 心房壓 Atrial contraction 心房開始收縮 心室開始收縮 The rise in atrial pressure (pink) that occurs in late diastole (phase 1) indicates the beginning of atrial contraction 心房收縮 this rise in pressure is small and short-lived In middle-diastole (phase 1), the ventricular pressure (green) occurs an abrupt but small rise is due to atrial contraction, which adds a small volume of blood to the ventricle Figure 14.17 A much larger increase in pressure that corresponds to ventricular systole 心室收縮 occurs Copyright © 20052Pearson Inc., publishing Cummings. (phase &3) &Education, the pressure fallsastoBenjamin near zero reflect relaxation of the myocardium 心室鬆弛 Aortic Pressure 主動脈壓 P436 心室充血期 The aortic valve 主動脈瓣 opens when ventricular pressure exceeds aortic pressure, and then closes when aortic pressure exceeds ventricular pressure The maximum pressure in the aorta during the cardiac cycle is the systolic pressure 收縮壓 (SP), whereas the minimum pressure during the cardiac cycle is the diastolic pressure 舒張壓 (DP) the average pressure during the cardiac cycle is the mean arterial pressure 平均動脈壓 (MAP) 等容收縮期 射血期 等容舒張期 心室充血期 主動脈 半月瓣 主動脈壓 心室壓 Figure 14.19 Aortic pressure is higher than ventricular pressure during diastole 舒張期 because the aorta 主動脈 is able to store pressure (energy) during systole 收縮期 the inward force exerted on the blood by the stretched elastic tissue in its wall As blood leaves the aorta and the pressure falls, the wall recoils 回彈 releases the energy drives the flow of blood through downstream vessels during diastole even though no blood Copyright © 2005 ejected Pearson Education, Inc., publishing Benjamin is being from the heart atasthis timeCummings. Ventricular Volume and Stroke Volume 心室容積及心搏量 心室充血期 等容收縮期 射血期 等容舒張期 P437 心室充血期 Volume of blood in ventricle at end of diastole 舒張末期容積 Volume of blood ejected from heart each cycle 心搏量 心房開始收縮 The volume does not change Volume of blood in ventricle at end of systole 收縮末期容積 When the ventricle contracts (phase 3), it does not eject all of the blood contained within it about 60 ml of blood remains in the ventricle at the end of systole under normal resting conditions ESV ESV 收縮末期容積 is determined by a number of factors, including the force of ventricular contraction, which can be altered by autonomic neurons and hormones Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.20 Heart Sounds 心音 P437-438 Sounds occur due to turbulent flow when valves close The sounds of the beating heart that can be heard through a stethoscope are called heart sounds 心音 A soft, low-pitched “lub”, designated the first sound 第一心音, and a louder, sharper, higher-pitched “dup”, designated the second sound 第二心音 The first sound occur at the start of systole 收縮期 (phase 2), when the AV valves closes 房室瓣關閉, and the second sound occur at the start of diastole 舒張期 Copyright © 2005 Pearson Education, publishing as Benjamin Cummings. (phase 4), when theInc., semilunar valves close 半月瓣關閉 Figure 14.21 VI. Cardiac Output and Its Control 心輸出量及其調控 • Autonomic Input to the Heart 自律神經的訊息傳入心臟 • Factors Affecting Cardiac Output: Changes in Heart Rate 影響心輸出量的因素:心跳速率的改變 • Factors Affecting Cardiac Output: Changes in Stroke Volume 影響心輸出量的因素:心搏量的改變 • Integration of Factors Affecting Cardiac Output 影響心輸出量因素的整合 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Cardiac Output 心輸出量 P438-439 The rate at which a ventricle pumps blood is called the cardiac output (CO) 心輸出量, and it is usually expressed in liters per minute (liter/min) The number of contractions per minute called the heart rate (HR) 心跳速率 the CO is determined by the HR and the volume of blood that is pumped from each ventricle with every beat, which we known as the stroke volume (SV) 心搏量 Cardiac Output (CO) = Heart rate (HR) X Stroke Volume (SV) For an adult at rest, the normal resting heart rate is around 72 beats/minute and the stroke volume is 70 ml (0.07 liter) a normal resting CO is CO = 72 beats/min X 0.07 liter/beat = 5 liters/min Regulation of the heart (or any other organ or tissue) by neural input, circulating hormones, or any other factor originating from outside the organ is referred to as extrinsic control 外因性控制 When the function of an organ or tissue is regulated by factors originating from within the organ or tissue itself, the function is said to be under intrinsic control 內因性控制 known as autoregulation 自發性調控 or local regulation 局部調控) Copyright © 2005 Pearson(also Education, Inc., publishing as Benjamin Cummings. Autonomic Input to the Heart 自律神經的訊息傳入心臟 P439-440 Figure 14.22 迷走神經 (副交感神經) 竇房節 延腦 頸 椎 房室節 交感神經的 心臟神經 胸 椎 Sympathetic nerves 交感神經 travel to the SA and AV nodes as well as to the ventricular myocardium; parasympathetic nerves 副交感神經 travel mainly to the nodes The distribution of parasympathetic fibers is relatively sparse 稀少 in the ventricles 心室 the ventricular myocardium is regulated primarily by the sympathetic nervous system 腰 椎 薦 椎 尾 椎 心室的心肌細胞 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. 脊 交感神經鏈 Factors Affecting Cardiac Output: Changes in Heart Rate 影響心輸出量的因素:心跳速率的改變 P440-442 A person’s heart rate depends on many factors, including his or her age, general health, level of muscular activity, and emotional state the various factors involved in the minute-by-minute regulation of heart rate 心跳速率, which is entirely under extrinsic control — Neural control of heart rate Sympathetic nerve Parasympathetic nerve — Hormonal control of heart rate — Integration of heart rate control Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Sympathetic Control of Heart Rate 交感神經調控心跳速率 P441-442 Pacemaker cells of the SA node 竇房節 receive direct input from the autonomic nervous system increased activity in sympathetic neurons 交感神經 to the SA node increases the frequency of action potentials 動作電位的頻率in the pacemaker cells Sympathetic neurons release norepinephrine (NE), which binds to b1 adrenergic receptors on the SA nodal cells and activates the cAMP system cAMP augments the opening of funny channels and T-type calcium channels the net result is an increase in the slope of spontaneous depolarization 去極化 and a decrease in the level of repolarization 再極化 Sympathetic neurons also project to the AV node and other part of the conduction system the speed of conducted & the delay of conducted the duration of systole 收縮期 Increase in the slope Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.23a Figure 14.24 Parasympathetic Control of Heart Rate 副交感神經調控心跳速率 P441-442 Increased activity in parasympathetic neurons 副交感神經 to the SA node decreases the frequency of action potentials 動作電位的頻率in the pacemaker cells Parasympathetic neurons release acetylcholine (Ach), which binds to muscarinic cholinergic receptors on the SA nodal cells and augments the opening of potassium channels and suppresses the opening of funny channels and T-type calcium channels the net result is an decrease in the slope of spontaneous depolarization 去極化 and a hyperpolarization 過極化 of the membrane potential Parasympathetic neurons also project to the AV node and other part of the conduction system the speed of conducted & the delay of conducted the duration of systole 收縮期延長 Decrease in the slope Figure 14.23b Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.24 Hormonal Control of Heart Rate 荷爾蒙調控心跳速率 P442 Although the function of the heart can be affected by a number of hormones, epinephrine 腎上腺素 is significant in the minute-to-minute regulation of cardiac function The effects of epinephrine , which is secreted by adrenal medulla 腎上腺髓質 in response to increased sympathetic activity, are similar to those exerted by sympathetic activity action potential frequency; the velocity of conduction HR Other hormones that directly affect cardiac function include the thyroid hormones 甲狀腺素, which are secreted by the thyroid gland, and insulin 胰島素 and glucagon 昇醣素, which are secreted by the pancreas These hormones primary increase the force of myocardial contraction, but glucagon also promotes increased heart rate Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Integration of Heart Rate Control 心跳速率調控的整合 P442 The heart rate is determined entirely by the frequency of action potential firing by the SA node, which is in turn regulated primarily by the following: — activity in sympathetic neurons projecting to the SA node HR — activity in parasympathetic neurons projecting to the SA node HR — levels of circulating epinephrine HR • SA node intrinsic firing rate = 100/min – • No extrinsic control on heart, HR = 100 SA node under control of ANS & hormones – Rest: Parasympathetic dominates, HR = 75 – Excitement: Sympathetic takes over, HR increases Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Factors Affecting Cardiac Output: Changes in Stroke Volume P443 影響心輸出量的因素:心搏量的改變 The second important determinant of cardiac output 心輸出量 is stroke volume 心搏量 can vary from moment to moment and depends to several factors — ventricular contractility 心室收縮力—a measure of the ventricles’ capacity for generating force Sympathetic control Hormonal control — end-diastolic volume 舒張末期容積 — afterload 後負荷—the pressure that the ventricles have to work against as they pump blood out of the heart Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Sympathetic Nervous Control of Ventricular Contractility 交感神經調控心室的收縮力 P443-444 Ventricular contractility, like heart rate, is almost entirely regulated by the sympathetic nervous system as sympathetic activity increase, ventricular contractility increases, which tends to raise cardiac output Action potentials trigger the release of NE binds to b1 receptors cAMP cAMP activates protein kinases that have four distinct effects: — phosphorylation of L-type Ca2+ channels in the plasma membrane Ca2+ — phosphorylation of Ca2+ channels in the sarcoplasmic reticulum membrane Ca2+ — phosphorylation of myosin increases the rate of myosin ATPase the speed of cross-bridge cycling Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.25 — phosphorylation of the Ca2+-ATPase on the sarcoplasmic reticulum membrane Ca2+ reuptake the rate of relaxation Sympathetic & Hormonal Control of Ventricular Contractility 交感神經及荷爾蒙調控心室的收縮力 P443-444 The net result is that under sympathetic influence, contractile cells contract faster and more strongly Ventricular contractility is affected by a number of hormones, including insulin, glucagon, and thyroid hormones, but most importantly it is regulated by epinephrine Sympathetic neural activity or epinephrine: Like norepinephrine, epinephrine increases myocardial contractility promoting increases in stroke volume and cardiac output Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. • increases strength of contraction • increases rate of contraction • increases rate of relaxation Figure 14.26 The Influence of End-Diastolic Volume on Stroke Volume 舒張末期容積對心搏量的影響 P443-444 When the rate at which blood flows into the heart from the veins (that is, venous return 靜脈回流) changes, the heart automatically adjusts its output to match the inflow Starling’s low 史達林定律 of the heart an intrinsic control 內因性調控 The physiological basis for the Starling effect is related to the fact that increases in end-diastolic volume (EDV) 舒張末期容積 cause muscle fibers in ventricular myocardium to lengthen Such stretching of the muscle fibers causes an increase in the force of contraction 收縮力增加 by two mechanism: — cardiac muscle has an optimum length that is much greater than its resting length and that is never reached in a healthy heart — stretching of muscle fibers induces an increase in the affinity of troponin for calcium binding between troponin and calcium number of crossbridges Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. The Starling Curve 史達林曲線 P444-445 The Starling curve is basically a length-tension curve長度-張力的曲線 such as the one shown in Figure 13.18 for skeletal muscle The EDV 舒張末期容積 is measure of the length of the muscle fiber as EDV increases, the muscle fibers are stretched to a longer length The stroke volume 心搏量 is a measure of cardiac muscle tension as the force of contraction increases, stroke volume increases The main difference between the length-tension curve for cardiac muscle compared to skeletal muscle is that cardiac muscle is always operating at lengths less than optimum thus the continuing positive slope to the curve Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 13.18 Figure 14.27 The Starling Curve 史達林曲線 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. P444-445 Family of Starling Curves 史達林曲線家族 P445 Normally, an increase in venous return 靜脈回流 causes an increase in EDV, which triggers an increase in stroke volume according to the Starling effect Because changes in either sympathetic activity or EDV affect the force of ventricular contraction, but by different mechanisms It is possible to alter stroke volume either by changing sympathetic activity without changing EDV, or by changing EDV without changing sympathetic activity cardiac function is therefore described not by a single Starling curve but instead by a family of curves In actuality, EDV and contractility can change simultaneously 同時 At any given EDV, a rise in sympathetic activity induces an increase in the stroke volume, which is reflected as an upward shift in the Starling curve Under the same conditions, a decrease in sympathetic activity induces a decrease in the stroke volume, which is reflected as a downward shift Upward or downward shifts in Starling curves reflect increases or decreases, respectively, in ventricular contractility 心室收縮力 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.28 Significance of Starling’s Law 史達林定律的意義 P445-446 If venous return were suddenly to increase but stroke volume did not (assume that heart rate is constant) with each beat, the heart would accumulate more blood which would eventually cause it to expand far beyond its normal size Starling’s law take on a new significance by adjusting stroke volume so that cardiac output matches venous return, the heart regulates its size If a ventricle contains a large volume of blood, the muscle of the wall has to exert greater tension to generate a given pressure Laplace’s Law 拉 佩斯定律 (張力與容器的直徑大小及內在壓力成正比) Certain pathological conditions can lead to chronic enlargement of the heart if the ventricles get too big, they become unable to generate enough pressure to maintain adequate cardiac output such an inability is called heart failure 心衰竭 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Factors Affecting End-Diastolic Volume & Stroke Volume 影響收縮末期容積及心搏量的因素 P446-447 EDV is primarily determined by end-diastolic pressure, sometimes referred to as preload 前負荷 because it places tension (or load) on the myocardium before it begins to contract The EDV of a ventricle is determined by the pressure of the blood inside it at the end of diastole (preload) as preload (end-diastole pressure) increases, EDV increases, and stroke volume increases according to Starling’s law Preload is determines by a number of factors — — — filling time 充血時間, which depends on heart rate atrial pressure 心房壓, which is determined by venous return and the force of atrial contraction central venous pressure 中央靜脈壓, the pressure of blood contained in the large veins that lead into the heart is affected by blood volume, muscular activity, and even changes in posture The most important influence of venous return is central venous pressure as central venous pressure rises, venous return increases because the increased pressure forces more blood to flow into the atria Stroke volume depends not only on how much force the ventricular muscle develops, but also on how large a force it has to work against when the heart ejects blood, the ventricular muscle works against arterial pressure Because arterial pressure places a load on the myocardium after contraction starts, it is called afterload 後負荷 increases in arterial pressure (afterload) tend to cause stroke Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. volume to decrease Summary of Factors Influencing Stroke Volume 簡略影響心搏量的因素 P447 • End-diastolic pressure = preload 前負荷 – Filling time 充血時間 – Atrial pressure 心房壓 – Central venous pressure 中央靜脈壓 • Afterload 後負荷 = pressure in aorta during ejection Stroke volume is influenced by three major factors: — ventricular contractility 心室收縮力, which is regulated by sympathetic activity and epinephrine — EDV 舒張末期容積, which is influenced primarily by preload — afterlod 後負荷, which depends on arterial pressure Figure 14.29 Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Integration of Factors Affecting Cardiac Output 影響心輸出量因素的整合 P447 Increases in sympathetic activity are typically accompanied by decreases in parasympathetic activity as a result, heart rate and stroke volume tend to increase, which raises cardiac output Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings. Figure 14.30