Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
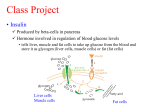
21 Adipose Tissue and Insulin Resistance Stephen E. Borst Abstract Adiposity, especially visceral adiposity, is an important risk factor for the development of insulin resistance and type 2 diabetes. In addition to its role in storing energy, adipose tissue also secretes into the circulation a number of hormones and other factors that can alter the response to insulin in distant tissues, such as liver and muscle. Many of these factors are cytokines, which have been associated with the immune system. Fat-derived hormones that can enhance insulin signaling include leptin, adiponectin, and possibly visfatin. Those impairing insulin signaling include tumor necrosis factor-F, resistin, and several of the interleukins. Obesity has also been identified as a low-grade inflammatory state. Several possible mechanisms are discussed whereby rapid growth of adipose tissue might trigger a local inflammatory response. It is suggested that this inflammatory response and associated release of cytokines may constitute the link between obesity and insulin resistance. Key Words: Tumor necrosis factor; resistin; adiponectin; interleukins; free fatty acids; subcutaneous fat; visceral fat; insulin signaling. 1. INTRODUCTION Obesity and type 2 diabetes are the most common metabolic diseases in Western society, together affecting as much as half of the adult population (1). Not only is the prevalence of these conditions high, but it also continues to increase. Insulin resistance is a prediabetic condition, characterized by a failure of target organs to respond normally to insulin. Insulin resistance includes a central component (incomplete suppression of hepatic glucose output) and a peripheral component (impaired insulin-mediated glucose uptake in skeletal muscle and adipose tissue) (2). When increased insulin secretion is no longer sufficient to prevent hyperglycemia, the subject progresses from insulin resistance to type 2 diabetes. Insulin resistance is associated with other conditions such as central obesity, hypertension, and dyslipidemia, all risk factors for cardiovascular disease. The constellation of these metabolic abnormalities has been termed metabolic syndrome. Obesity is a well-recognized risk factor for the development of insulin resistance and metabolic syndrome. In addition to the total amount of fat, distribution of adipose tissue is also important, with most studies concluding that visceral fat contributes considerably more to insulin resistance than does subcutaneous fat (3). However, one report, by Misra et al., documented a robust correlation between posterior abdominal subcutaneous fat From: Nutrition and Health: Adipose Tissue and Adipokines in Health and Disease Edited by: G. Fantuzzi and T. Mazzone © Humana Press Inc., Totowa, NJ 281 282 Part V / Adipose Tissue and Disease and insulin resistance (4). Underscoring the importance of visceral fat is the report by Klein et al. that liposuction, resulting in a substantial reduction of subcutaneous fat, did not enhance insulin responsiveness in insulin-resistant subjects (5). In rats, we (6) and others (7) have found that surgical removal of visceral fat reverses insulin resistance. Traditionally, adipose tissue has been regarded largely as a depot for stored fat. More recently, it has become clear that adipose tissue plays an active role in energy metabolism and is the source of hormones, cytokines, and metabolites that play an important role in whole-body metabolism (8). The role of these substances may be either autocrine or endocrine. Adipose tissue, especially visceral fat, is the source of a number of substances that might play a role in the development of insulin resistance. Among the latter are tumor necrosis factor (TNF)-F, adiponectin, interleukin (IL)-6, resistin, and free fatty acids. The difference in the metabolic effects of visceral versus subcutaneous fat may be attributed both to differences in the hormones secreted by the two types of fat and to the fact that hormones secreted by visceral fat reach the liver in high concentration. The latter is due to the fact that visceral fat drains into the portal circulation, whereas subcutaneous fat drains into the systemic circulation (8). This review will focus on the regulation of insulin responsiveness by adipokines and on evidence supporting the hypothesis that these hormones play a role in the pathophysiology of insulin resistance. 2. OBESITY AS AN INFLAMMATORY CONDITION Obesity produces a state of low-grade inflammation, characterized by elevated circulating concentrations of acute-phase proteins, such as C-reactive protein (CRP), plasminogen activator inhibitor (PAI)-1, and fibrinogen (9,10). CRP is elevated moderately in obese men and highly in obese women (11). Hak et al. reported that in a group of healthy middle-aged women, CRP was approximately threefold higher in the group whose body mass index (BMI) was in the upper half (9). The mean CRP concentration in the upperBMI group was 1.15 mg/L, around the threshold of a clinically elevated level (11). There are at least two theories as to why obesity should cause a state of inflammation. First, the growth—especially the rapid growth—of adipose tissue may cause local hypoxia due to inadequate perfusion and result in the generation of angiogenesis factors such as vascular endothelial growth factor (VEGF) and 11G-hydroxysteroid dehydrogenase type 1. Overexpression of the latter enzyme in rodents has been shown to cause adipose production of the inflammatory cytokines resistin and TNF-F, both cytokines being implicated in the development of insulin resistance (12). A second possibility is that rapid expansion of adipose tissue results in the differentiation of preadipocytes into macrophage-like cells (13). It is well-known that obesity is accompanied by an overexpression of TNF-F in adipose tissue. Weisberg et al. have recently shown that obesity is accompanied by an increased number of macrophages in adipose tissue, but not in liver or muscle (14). The overexpression of TNF-F that occurs in adipose tissue of obese humans occurs exclusively in macrophages. 3. ROLE OF LEPTIN RESISTANCE IN OBESITY AND INSULIN RESISTANCE Leptin is produced by adipocytes and secreted into the blood. In the healthy state, the circulating leptin concentration varies in proportion to adipose mass. Activation of leptin Chapter 21 / Adipose Tissue and Insulin Resistance 283 receptors in the hypothalamus decreases food intake and increases energy expenditure via uncoupling proteins (UCPs) in fat and muscle. UCPs are mitochondrial proteins that allow for oxidation of substrates with the production of heat, rather than storage of energy in the form of ATP. Thus leptin serves as part of an “adipostat” mechanism, whereby increased adiposity sets in motion responses that will eventually reduce adiposity. In 1994, Friedman et al. discovered that ob/ob mice are leptin-deficient and lose weight following leptin treatment (15). However, obese humans are typically leptin-resistant and have higher-than-normal circulating concentrations of leptin. Leptin resistance in humans has two components: impaired transport of leptin across the blood–brain barrier and impaired signaling via hypothalamic leptin receptors (16). In addition to its function as a direct regulator of adiposity, leptin is also an insulinsensitizing hormone (17,18). Thus, the reduced responsiveness to leptin that accompanies obesity and may play a role in causing obesity also plays a role in causing insulin resistance in the brain. Insulin receptors in the hypothalamus play an important role in glucose homeostasis (18). Primate studies have shown that direct delivery of insulin to the brain reduces feeding (18); rodent studies have shown that intracerebroventricular administration of insulin not only reduces food intake, but also suppresses hepatic glucose output (19,20). There is growing evidence that the link between leptin resistance and insulin resistance is suppressor of cytokine signaling (SOCS)3, a molecule that impairs signaling of both leptin and insulin (21), and one that is suppressed by leptin (22). Mice with reduced neuronal expression of SOCS have enhanced sensitivity to leptin and insulin and are protected against diet-induced obesity (23). 4. ROLE OF TNF-F IN LINKING OBESITY TO INSULIN RESISTANCE TNF-F was first shown by Hotamisligil et al. to be overexpressed in adipose tissue from several strains of obese rodents (24). Weisberg et al. have shown that macrophages are the main source of TNF-F in adipose tissue (14). TNF-F expression is higher in visceral fat (VF) of rodents than in subcutaneous (sc) fat (25). In addition, TNF-F has been shown to impair insulin signaling in cultured cells by three separate molecular mechanisms. TNF-F activates serine/threonine kinases that phosphorylate and impair the function of key elements in the insulin signaling pathway (26). First, TNF-F mediates a serine phosphorylation of IRS-1 (27). This alteration impairs insulin signaling by making IRS-1 resistant to subsequent insulin-stimulated tyrosine phosphorylation. Second, TNF-F phosphorylates and activates a protein tyrosine phosphatase that normally terminates insulin action, thus playing a role in the self-limiting nature of insulin signaling (28). Third, TNF-F phosphorylates and inactivates the protein phosphate PP-1 at site 2, resulting in its inactivation (29). This action of TNF-F opposes the action of insulin, whereby glucose storage is promoted by phosphorylating PP-1 at site 1 and activating it. The above findings led to the popular theory that TNF-F of adipose origin is secreted into the circulation, from where it reaches targets such as muscle and liver and causes insulin resistance. However, circulating levels of TNF-F are very low compared with the concentrations required to induce insulin resistance when infused into rats (30) and tissue levels of TNF-F are several orders of magnitude higher than circulating levels (31). Whereas some studies have shown that circulating TNF-F is elevated in obese and insulin-resistant subjects (32), others have not (33). 284 Part V / Adipose Tissue and Disease We hypothesize that locally produced TNF-F may contribute to insulin resistance in one of two ways. First, obesity may cause insulin resistance in by increasing TNF-F expression in targets such as muscle. Support for this concept is our report that diet-induced obesity in rats is accompanied by reduced insulin-stimulated glucose transport in skeletal muscle, together with an increase in muscle expression of TNF-F (34). Alternatively, obesity may increase TNF-F expression in adipose tissue, leading to the release into the circulation of other cytokines that are capable of causing systemic insulin resistance. 5. ROLE OF ADIPONECTIN IN INSULIN RESISTANCE Adiponectin is an insulin-sensitizing hormone produced exclusively by adipocytes (35). There is a strong and positive correlation between serum adiponectin and insulin responsiveness. In a group of normal and obese subjects, Weyer et al. studied the relationship between serum adiponectin and the glucose disposal rate, measured during hyperinsulinemic euglycemic glucose clamp studies (36). Serum adiponectin varied over a fivefold range, correlated positively with glucose disposal, and accounted for approx 35% of the variance in insulin responsiveness. Adiponectin increases oxidation of free fatty acids and reduces postprandial elevation of nonesterified fatty acids (NEFAs) in mice (37). Adiponectin circulates at concentrations in the low Rg/mL range, whereas most cytokines produced by adipose tissue are in the pg/mL range (35). In rodents, adiponectin expression is considerably higher in VF than in sc fat (38), and adiponectin secretion by VF has an inverse relationship with VF mass— i.e., the larger the mass of VF, the less adiponectin is secreted. Serum adiponectin is low in obese humans (39) and increases following weight loss (40). Yamauchi et al. have shown that administration of adiponectin to obese rats on a high-fat diet reduces weight gain and prevents the development of hepatic insulin resistance (41). The mechanism by which adiponectin enhances insulin responses has not been well-studied, but may involve opposing of TNF-F-induced activation of the transcription factor NFPB (42). 6. ROLE OF RESISTIN IN INSULIN RESISTANCE Resistin is a recently discovered polypeptide that is secreted by mouse adipocytes and has been implicated in the development of insulin resistance. Resistin was first described in 2001, when a search for genes that are induced during adipocyte differentiation but downregulated in mature adipocytes during exposure to thiazolidinediones led to the discovery of a protein the investigators named resistin, for “resistance to insulin” (43). Administration of resistin in normal mice impairs glucose tolerance and insulin action. Furthermore, immunoneutralization of resistin improved blood glucose and insulin action in animal models of obesity-induced insulin resistance. In rodents, administration of thiazolidinedione drugs reverses insulin resistance. These drugs also reduce gene and protein expression of resistin in some studies (44) but not in others (45). These initial data suggested that resistin, at least in part, may explain how adiposity leads to insulin resistance and may also explain the antidiabetic effects of thiazolidinedione drugs. The molecular mechanism for the action of resistin is unknown. A recent study in mice suggested that resistin selectively impairs the inhibitory action of insulin on hepatic glucose production (44). However, the role of resistin in obesity-associated insulin resistance has become controversial because the biology of resistin is different Chapter 21 / Adipose Tissue and Insulin Resistance 285 in humans than in rodents and additional evidence has suggested that obesity and insulin resistance are associated with decreased resistin expression (45–47). Whether resistin is expressed in human adipose tissue is not clear. McTernan et al. found such expression and reported that resistin is relatively highly expressed in the omental visceral fat and the abdominal subcutaneous fat, with lower expression in subcutaneous fat on the thigh (48). This finding is in contrast to the findings of Savage et al. and Nagaev et al., who did not detect resistin in human adipose tissue (49,50). Whereas resistin is expressed mainly in adipocytes in mice (43), Fain et al. reported that most of the resistin secreted by human fat explants is derived from nonadipocytes (51). The reason for the differences in these studies is unclear. Human resistin is only 59% similar to the mouse protein, and this may portend important differences in the endocrine functions of adipocytes and resistin between rodents and humans (52). Furthermore, insulin and TNF-F, both elevated in obesity, have been found to inhibit resistin expression, which may explain the low levels of resistin found in the recent studies of obesity diabetes. The initial suggestion that resistin may be the link between obesity and insulin resistance is being challenged. The role of resistin in normal and abnormal physiology remains elusive. Studies from knockout mice and better characterization of resistin changes in humans should help determine whether this adipokine is a cause of insulin resistance or simply a bystander. Also, it will important to understand the similarities and differences between mouse and human resistin and mechanisms of obesity-related insulin resistance. 7. ROLE OF IL-6 IN INSULIN RESISTANCE IL-6 is a pleiotropic circulating cytokine that has important roles in inflammation, host defense, and response to tissue injury (53). It is one of several proinflammatory cytokines with a proposed role in the development of insulin resistance. IL-6 is secreted by many cell types, including immune cells, fibroblasts, endothelial cells, skeletal muscle, and nonadipocyte cells in adipose tissue, and circulates as a variably glycosylated 22- to 27-kDa protein (2). IL-6 is released from contracting skeletal muscle, causing the serum concentration to increase as much as 100-fold (54). IL-6 increases hepatic glucose production when administered to human subjects, and there is evidence to suggest that the release of IL-6 from exercising muscle mediates the early phase on exercise-induced hepatic glucose output. The fact that IL-6 opposes insulin action in the liver has led to speculation that its oversecretion may play a role in insulin resistance. In the liver, IL-6 causes release of NEFAs and is the primary stimulator of for production of acute phase proteins (55). Administration of IL-6 in healthy volunteers induced dose-dependent increases in blood glucose (56), probably by inducing resistance to insulin action. In vitro, IL-6 has been shown to impair insulin signaling by several distinct molecular mechanisms (57). Weight loss significantly decreases IL-6 levels in both adipose tissue and serum (58). Genetic studies have also demonstrated a high level of correlation between insulin resistance and IL-6 gene polymorphism (59). Besides its glucoregulatory effect, IL-6 increases circulating free fatty acids (FFA) from adipose tissue with their well-described adverse effects on insulin sensitivity (60). Because visceral depots drain into the portal circulation, the metabolic effects of IL-6 on the liver become important. Indeed, there is 286 Part V / Adipose Tissue and Disease evidence to suggest that IL-6 inhibits insulin receptor signal transduction in hepatocytes that is mediated, at least in part, by induction of SOCS3 (61). IL-6 may also exert its adverse effects, at least in part, by decreasing adipose secretion adiponectin (62). Although much evidence implicates IL-6 in insulin resistance, there is some conflicting evidence. In a recent study, acute IL-6 administration did not impair glucose homeostasis in healthy individuals (63). Moreover, IL-6-deficient mice were not protected from development of obesity and glucose intolerance (64). Circulating IL-6 is elevated approximately twofold in obese, insulin-resistant subjects, but although the association is statistically significant, the relationship is not a strong one, accounting only for approx 7% of the variance in insulin responsiveness (33,65,66). Although VF produces two- to threefold more IL-6 than does sc fat, adipose tissue is the source for only about 30% of circulating IL-6 in humans (38), with the majority of adipose tissue-derived IL-6 coming from stromal immune cells and not adipocytes (67). In summary, a body of evidence indicates that IL-6 of adipose origin may play a role in systemic insulin resistance, although there is also some evidence to the contrary. 8. OTHER POSSIBLE MEDIATORS OF INSULIN RESISTANCE Visfatin is a recently discovered adipokine that is produced by adipocytes (68), and is expressed in visceral fat at much higher levels than in subcutaneous fat (69). Serum visfatin increases with VF, but not sc fat, in humans and mice. Visfatin has been shown to have insulin-sensitizing properties when administered to insulin-resistant mice. Mice that are heterozygous for a targeted mutation in the visfatin gene display a small impairment in glucose tolerance, whereas homozygous mice die in utero. Visfatin binds to the insulin receptor and activates downstream signaling, but does not compete for binding with insulin. Visfatin has the ability to stimulate glucose transport in cultured muscle and adipose cells and to inhibit glucose output in cultured hepatocytes. Apart from cytokines, the most important candidate for linking obesity to insulin resistance is circulating nonesterified (or free) fatty acids. Reaven et al. reported that type 2 diabetes is associated with elevations in both fasting and postprandial NEFAs (70). Boden et al. have shown that both acute infusion and chronic elevations of NEFAs can decrease insulin-stimulated glucose disposal in humans (71). It is proposed that increased hydrolysis of NEFAs leads to increased diacyl glycerol, which in turn activates isoforms of protein kinase C (PKC). Although activation of PKC-_ is a part of normal insulin signaling, activation of PKC-V has been shown to impair insulin signaling (72). Muscle biopsies from insulin-resistant subjects display serine/threonine phosphorylation of the insulin receptor, an impairment that TNF-F does not cause in cultured cells (73). Current evidence suggests that serine/threonine phosphorylation of IRs is mediated by the theta isoform of protein kinase C, an enzyme that may be activated by an increase in serum FFA (74). Additionally, Bjorntorp has hypothesized that increased visceral fat causes hepatic insulin resistance by a “portal” mechanism, where a higher concentration of NEFAs reach the liver from omental fat (75). 9. CONCLUSIONS Table 1 lists candidate adipokines that may potentially link obesity with insulin resistance. Such candidates should meet several criteria. The adipokine should have a 287 Enhancement Leptin Elevated in rodent models of genetic and diet-induced obesity May be elevated in human obesity and insulin resistance Dramatic elevation in obese humans (54) Serum adiponectin is low in obese humans (37) and increases following weight loss (39) Increased in human visceral adiposity (64) High in obese humans, because of leptin resistance Change in blood concentration Adipocytes (2) Adipocytes (68) Adipose tissue macrophages (14), liver and muscle (26) Non-adipocyte fat cells, immune cells, skeletal muscle (2) Adipocytes (37) Mouse adipocytes (43), human non-adipocyte fat cells (51) Tissue expression Higher in SCF of humans (8) Higher in VF of humans (66) Higher in VF of rodents (38) Higher in VF of humans (38) Markedly higher in VF of rodents (25). Equal in VF and SCF of humans (48) Higher in VF of rodents (25) Expression in VF vs SCF aCandidate proteins should meet the following criteria: (1) the hormone should have an effect on insulin responses, (2) blood levels should be appropriately elevated of reduced in obesity and insulin resistance, (3) a significant fraction of circulating hormone should derive from adipose tissue and (4) production of the hormone should be higher in visceral fat (VF) than in subcutaneous fat (SCF). Enhancement Impairment IL-6 Visfatin Impairment TNF-F Enhancement Impairment Resistin Adiponectin Effect on insulin response Adipokine Table 1 Circulating Proteins Secreted by Adipose Tissue and That May Link Obesity to Insulin Resistance and Diabetes 288 Part V / Adipose Tissue and Disease major effect on insulin responsiveness; the circulating level should correlate to insulin responsiveness and increase or decrease appropriately in animal models and experimental conditions. A significant fraction of the circulating cytokine should be of adipose origin and expression should be higher in visceral fat than in subcutaneous fat. Based on these criteria, there is strong evidence in favor of adiponectin as a link between obesity and insulin resistance. Adiponectin is an insulin-sensitizing hormone that is produced almost exclusively in fat, with higher expression in visceral fat. Serum adiponectin is strongly and inversely correlated to insulin resistance and fat mass and increases after weight reduction. There is evidence both for and against the role of IL-6 in linking obesity to insulin resistance. IL-6 has the ability to impair insulin responses and is elevated in obesity, but circulating levels correlate only weakly to insulin responsiveness. The case for resistin is strong in rodents, but weaker in humans. Resistin is preferentially expressed in visceral fat of mice and is elevated in rodent models of genetic and diet-induced obesity. However, resistin biology may be different in humans, and some studies suggest that it is not expressed in human adipose tissue. Leptin is an insulinsensitizing hormone that is elevated in serum of obese subjects owing to leptin resistance. This phenomenon is similar to the elevation of insulin in insulin resistance. Leptin plays a prominent role in the development of obesity. Leptin resistance may also underlie insulin resistance in the brain. TNF-F is overexpressed in tissues of obese and insulin-resistant animals. TNF-F circulates at low levels; some studies have found serum levels to be elevated in insulin-resistant subjects, while others have not. TNF-F impairs insulin responses in muscle fat and liver by well-established molecular mechanisms. Most evidence suggests that TNF-F plays a paracrine or autocrine role in linking obesity to insulin resistance. Visfatin is a recently discovered insulin-sensitizing hormone that increases with visceral fat mass. Although less is known about visfatin than other adipokines, the latter finding argues against its role as a link between obesity and insulin resistance. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. Must A, Spadano J, Coakley EH, et al. JAMA 1999;282:1523–1529. Pittas AG, Joseph NA, Greenberg AS. J Clin Endocrinol Metab 2004;89:447–452. Pieris AN, Struve MF, Mueller RA, et al. J Clin Endocrinol Metab 1988;67:760–767. Misra A, Garg A, Abate N, et al. Obes Res 1997;5:93–99. Klein S, Fontana L, Young VL, et al. N Engl J Med 2004;350:2549–2557. Borst SE, Conover CF, Bagby GJ. Cytokine 2005;32:39–44. Gabriely I, Barzilai N. Curr Diab Rep 2003;3:201–206. Kershaw EE, Flier JS. J Clin Endocrinol Metab 2005;89:2548–2556. Hak EA, Stenhouer CD, Bo KH, et al. Aterioscler Thromb Vasc Biol 1999;19:1986–1991. Tataranni PA, Ortega E. Diabetes 2005;54:917–927. Visser M, Bouter LM, McQuillan GM, et al. JAMA 1999;282:2131–2135. Mazusaki H, Peterson J, Shinyama H, et al. Science 2001;294:2166–2170. Charriere G, Cousin B, Arnaud E, et al. J Biol Chem 2003;278:9850–9855. Weisberg SP, McCann D, Desai M, et al. J Clin Invest 2003;112:1796–1808. Zhang Y, Proenca R, Maffei M, et al. Nature 1994;372:425–432. Erratum in Nature 1995;374:479. Scarpace PJ, Tumer N. Physiol Behav 2001;74:721–727. Lazar MA. Science 2005;307:373–375. Chapter 21 / Adipose Tissue and Insulin Resistance 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 289 Schwartz MW, Porte D Jr. Science 2005;307:375–379. Zimmet P, Thomas CR. J Intern Med 2003;254:114–125. O’Rahilly S, Farooqi IS, Yeo GS, et al. Endocrinology 2003;144:3757–3764. Frisch RE, McArthur JW. Science 1974;185:949–951. Welt CK, Chan JL, Bullpen J, et al. N Engl J Med 2004;351:987–997. Hales CN, Barker DJ. Diabetologia 1992;35:595–601. Hotamisligil GS, Shargill NS, Spiegelman BM. Science 1993;259:87–91. Das M, Gabriely I, Barzilai N. Obes Rev 2004;5:13–19. Borst SE. Endocrine 2004;23:1771–1782. Hotamisligil GS, Peraldi P, Budavari A, et al. Science 1996;271:665–668. Ahmad F, Goldstein BJ. J Cell Biochem 1997;64:117–127. Ragolia L, Begum N Mol Cell Biochem 1998;182:49–58. Lang CH, Dobrescu C, Bagby GJ. Endocrinology 1992;130:43–52. Borst SE, Bagby GJ. Cytokine 2004;26:217–222. Tsigos C, Papanicolaou DA, Kyrou I, et al. J Clin Endocrinol Metab 1997;82:4167–4170. Kern PA, Ranganathan S, Li C, et al. Am J Physiol Endocrinol Metab 2001;280:E745–E751. Borst SE Conover CF. Life Sci 2005;77:2156–2165. Gil-Campos M, Canete RR, Gil A. Clin Nutr 2004;23:963–974. Weyer C, Funahashi T, Tanaka S, et al. J Clin Endocrinol Metab 2005;86:1930–1935. Fruebis J, Tsao TS, Javorschi S, et al. Proc Natl Acad Sci USA 2001;13:2005–2010. Aldhahi W, Hamdy O. Curr Diab Rep 2003;3:293–298. Argiles JM, Lopez-Soriano J, Almendro V, et al. Med Res Rev 2005;25:49–65. Yang WS, Lee WJ, Funahashi T, et al. J Clin Endocrinol Metab 2001;86:3815–3819. Yamauchi T, Kamon J, Waki H, et al. Nat Med 2001;7:941–946. Ouchi N, Kihara S, Arita Y, et al. Circulation 2000;102:1296–1301. Steppan CM, Bailey ST, Bhat S, et al. Nature 2001;409:307–312. Rajala MW, Obici S, Scherer PE, et al. J Clin Invest 2003;111:225–230. Way JM, Gorgun CZ, Tong Q, et al. J Biol Chem 2001;276:25,651–25,653. Milan G, Granzotto M, Scarda A, et al. Obes Res 2002;10:1095–1103. Juan CC, Au LC, Fang VS, et al. Biochem Biophys Res Commun 2001;289:1328–1333. McTernan PG, McTernan CL, Chetty R, et al. J Clin Endocrinol Metab 2002;87:2407–2410. Savage DB, Sewter CP, Klenk ES, et al. Diabetes 2001;50:2199–2202. Nagaev I, Smith U. Biochem Biophys Res Commun 2001;285:561–564. Fain JN, Cheema PS, Bahouth SW, et al. Biochem Biophys Res Commun 2003;300:674–678. Steppan CM, Lazar MA. Trends Endocrinol Metab 2002;13:18–23. Papanicolaou DA, Wilder RL, Manolagas SC, et al. Ann Intern Med 1998;128:127–137. Febraio MA, Pedersen BK. FASEB J 2002;16:1335–1347. Gabay C, Kushner I. N Engl J Med 1999;340:448–454. Fernandez-Real JM, Ricart W. Endocr Rev 2003;24:278–301. Senn JJ, Klover PJ, Nowalk IA, Mooney RA. Diabetes 2002;51:3391–3399. Bastard JP, Jardel C, Bruckert E, et al. J Clin Endocrinol Metab 2000;85:3338–3342. Vozarova B, Fernandez-Real JM, Knowler WC, et al. Hum Genet 2003;112:409–413. Boden G, Shulman GI. Eur J Clin Invest 2002;32:14–23. Senn JJ, Klover PJ, Nowak IA, et al. J Biol Chem 2003;278:13,740–13,746. Fasshauer M, Kralisch S, Klier M, et al. Biochem Biophys Res Commun 2003;301:1045–1050. Steensberg A, Fischer CP, Sacchetti M, et al. J Physiol 2003;548:631–638. Wallenius V, Wallenius K, Ahren B, et al. Nat Med 2002;8:75–79. Vozarova B, Weyer C, Hanson K, et al. Obes Res 2001;9:414–417. Pradhan AD, Manson JE, Rifai N, et al. JAMA 2001;286:327–334. Fried SK, Bunkin DA, Greenberg AS. J Clin Endocrinol Metab 1998;83:847–850. Hammarstedt A, Pihlajamaki J, Sopasakis VR, et al. J Clin Endocrinol Metab 2006;91:1181–1184. Hug C, Lodish HF. Science 2005;307:366–367. Reaven GM, Hollenbeck C, Jeng CY, et al. Diabetes 1988;37:1020–1024. Boden G. Diabetes Care 1996;19:394–395. 290 72. 73. 74. 75. Part V / Adipose Tissue and Disease Itani SI, Pories WJ, Macdonald KG, et al. Metabolism 2001;50:553–557. Kanety H, Feinstein R, Papa MZ, et al. J Biol Chem 1995;270:23,780–23,784. Dohm GL, Tapscott EB, Pories WJ, et al. J Clin Invest 1988;8:486–494. Bjorntorp P. Arteriosclerosis 1990;10:493–496.