Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Jatene procedure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
PATHOPHYSIOLOGY AND NATURAL HISTORY
ELECTROPHYSIOLOGY
Inhibition in the human heart
ERIC N. PRYSTOWSKY, M.D.,
AND
DOUGLAS P. ZIPES, M.D.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
ABSTRACT Subthreshold electrotonic depolarizations have been shown to exert inhibitory actions
on impulse conduction and generation in isolated cardiac tissues. We performed this study to determine
whether inhibition occurs in human myocardium, and to investigate the effects of time and voltage, as
well as distance, on myocardial inhibition. Sixteen subjects were studied in the clinical electrophysiology laboratory by standard techniques. Atrial and ventricular pacing were performed with the use of a
quadripolar catheter. The basic drive train (S ) and premature stimulus (S2) were introduced at the distal
bipolar electrode pair through one current output generator and the subthreshold conditioning stimulus
(SC) was introduced before S2 at the distal or proximal bipolar pair through a separate current output
generator. When SC was initiated at the distal electrodes 40 msec before S2 inhibition of S2 could
always be demonstrated (atrium or ventriclej. Since SC was introduced progressively earlier than S29 Sc
inhibited the response to S2 according to a curvilinear strength-interval relationship; increasing milliamperes of S from less than 1.0 to 10.0 increased the interval at which preceded S2 and still inhibited S2.
With currents of of 10.0 mA or less, inhibited in the ventricle (n = 1 1) and atriumn (n = 5) when
and 80 to 190 msec
40 to 160 msec
85
116
Sc
SC
preceded S2 by
Sc
SC
S2
(mean msec)
(mean
msec), respectively.
Ventricular inhibition attempted with Sc at the proximal bipolar pair and S a.t the distal pair was
successful in three of nine patients. The effect of Sc on ventricular excitability threshold of S2 was
determined in three patients. For all three patients the current threshold of S2 varied directly as a
function of the magnitude of current used for S These data demonstrate that (1) subthreshold stimuli
can prevent subsequent threshold stimuli from depolarizing human atrium and ventricle, (2) inhibition
is both time and voltage dependent, and (3) inhibition is more effective if the inhibitory stimulus is
applied close to the site of the threshold stimulus. Inhibition most likely occurs by Sc electronically
affecting the response of the tissue to S29 possibly in part by modifying myocardial excitability
threshold, thereby preventing S2 from initiating an active response.
Circulation 68, No. 4, 707-713, 1983.
.
THAT AN electrical stimulus that does not completely
depolarize myocardium has the ability to interact with
a subsequent stimulus that activates myocardium has
been known for some time. Drury and Love' showed in
the frog ventricle that a subthreshold electrical stimulus initiated before a threshold stimulus could prevent
the threshold stimulus from evoking a recordable ventricular depolarization. Lewis and Drury2 made similar
observations in the dog atrium. Tamargo et al .3 demonstrated that subthreshold stimuli could inhibit threshold stimuli from activating canine ventricle.
The phenomenon of inhibition and its properties
From the Krannert Institute of Cardiology, the Department of Medicine, Indiana University School of Medicine, and from the Veterans
Administration Medical Center, Indianapolis.
Supported in part by the Herman C. Krannert Fund, Indianapolis, by
grants HL-06308, HL-07182, and HL-18795 from the National Heart,
Lung and Blood Institute, National Institutes of Health, Bethesda, and
the American Heart Association, Indiana Affiliate, and the Veterans
Administration, Indianapolis.
Address for correspondence: Eric N. Prystowsky, M.D., Clinical
Electrophysiology Laboratory, Indiana University School of Medicine,
1100 West Michigan St., Indianapolis, IN 46223.
Received Feb. 21, 1983; revision accepted June 9, 1983.
Vol. 68, No. 4, October 1983
have not been delineated in the human heart. The purpose of this investigation was to determine whether
inhibition in human atrium and ventricle occurs, and to
analyze the effects of time and voltage as well as distance on inhibition in the human ventricle.
Methods
Sixteen patients in a postabsorptive nonsedated state and with
a variety of arrhythmias (table 1) were studied in the electrophysiology laboratory. All patients gave informed written and
verbal consent before entering the study. There were 14 men
and two women in the study with a mean age of 52 + 14 years.
Three to four electrode catheters were inserted percutaneously
into the femoral and/or brachial veins and positioned under
fluoroscopic guidance to multiple areas of the heart. In all patients ventricular pacing was performed with a quadripolar catheter (USCI) with 10 mm interelectrode distance. The right ventricular catheter for all studies was positioned at the apex. Atrial
pacing was performed with a quadripolar catheter with 5 mm
interelectrode distance (USCI) that was positioned in the high
right atrial area. A second atrial catheter was positioned near the
first atrial catheter to record the bipolar atrial electrogram.
Pacing protocol. For the inhibition studies in the atrium or
ventricle, the following protocol was used. A programmable
custom-built stimulator (MECA) was used to pace the heart with
707
PRYSTOWSKY and ZIPES
TABLE 1
Patient characteristics
Patient
No.
Age
Sex
M
M
M
M
M
M
10
77
61
63
59
48
56
40
46
56
16
11
50
12
13
14
15
16
57
48
59
61
38
M
M
M
M
M
M
1
2
3
4
5
6
7
8
9
F
F
M
M
Structural
heart
disease
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
CAD
CAD
CAD
CM
CAD
None
None
None
CAD
CAD
CAD
None
MVP
CAD
CAD
CAD
Clinical
arrhythmia
VT
VT
SSS
VT
VTI/VF
VT
Bradycardia
AVN reentry
VT
VT/VF
VT
VT
VT
VT
VT/VF
VF
AVN = atrioventricular node; CAD coronary artery disease; CM
cardiomyopathy; MVP = mitral valve prolapse; SSS = sick sinus
syndrome; VF = ventricular fibrillation; VT = ventricular tachycardia.
rectangular pulses (WPI) delivered through an isolation unit for
the basic drive train (SI) and the premature stimulus (S2). The
pulse width of SI and S2 was 2.0 msec and the current used was
twice late-diastolic threshold (1.0 to 1.4 mA). A second current
output generator (WPI) that delivered 2 msec rectangular stimuli through an isolation transformer was used to introduce the
conditioning stimulus (Sc). The SI, S2, and S, stimuli were
bipolar and, regardless of whether the distal or proximal bipolar
electrode pair on the quadripolar catheter were used for stimulation, the distal pole of the pair was always the cathode and the
proximal pole the anode. Ventricular and atrial refractoriness
were determined by stimulating the myocardium with a train of
eight complexes and after each eighth complex a premature
stimulus was introduced beginning in late diastole. The SIS2
interval was shortened progressively until S2 consistently failed
to evoke a response. The longest SIS2 interval that did not result
in myocardial depolarization on two consecutive attempts was
defined as the effective refractory period of the tissue being
tested.
To test for ventricular inhibition, the stimulator delivering the
basic train and premature interval was set at a fixed SISI and
S1S2 interval. The SIS2 interval was 10 to 20 msec longer than
the effective refractory period and S2 always produced a ventricular response. Then, with the use of a separate current generator, Sc was introduced beginning 20 msec before the occurrence of S2 and within the duration of the ventricular effective
refractory period. The current of S, always was subthreshold
and by itself Sc never produced a ventricular response. As the
current of SC was increased, especially at levels of 6.0 mA or
more, SC was periodically introduced without S2 to ensure that
SC by itself did not result in myocardial depolarization. The
current level of S, was increased in 0.1 to 0.3 mA increments
until SC inhibited ventricular depolarization of S2. At this point,
the current level of SC was kept constant but the S, stimulus was
moved 10 msec earlier than the previous ScS2 interval. If SC
failed to inhibit S2 then the mA was again increased progressively until Sc inhibited S2. This process was repeated until an ScS2
interval was obtained at which an SC of 10 mA no longer inhibit708
ed S2. In 11 patients SI, S2, and S, were initiated at the distal
bipolar pair and the proximal bipolar pair was used to record the
local electrogram. In nine patients S I and S2 were initiated at the
distal bipolar electrode pair but Sc was introduced at the proximal bipolar pair. For these patients the catheter was positioned
so that late-diastolic pacing threshold was similar for the distal
and proximal bipolar pair.
For atrial inhibition a protocol similar to that detailed above
for ventricular inhibition was used. Five patients underwent this
protocol and for all five patients, SI, S2 and S, were initiated at
the distal bipolar pair. A second electrode catheter positioned
near the first catheter was used to record atrial potentials because the stimulus artifact often obscured atrial depolarization
recorded from the same catheter that delivered the stimulus.
The effect of Sc on threshold of S2 in the ventricle was investigated in patients 14 through 16. For each patient SI, S2, and Sc
were delivered at the distal bipolar electrode pair. Stimuli for SI
and S2 were initiated from a separate current output generator
than stimuli for S, (see above). Pulse width for all stimuli was
2.0 msec. The SIS2 interval was 10 to 20 msec longer than the
ventricular effective refractory period and S2 without Sc always
depolarized the ventricle. The ScS2 interval was 50 msec and did
not vary throughout the study. Initial current of S2 was twice
late-diastolic threshold. Then, as the current of Sc was increased
stepwise to inhibit S2, the current level of S2 was increased by
0.1 mA increments until S2 again produced a ventricular response. All Sc stimuli were subthreshold.
In six patients we tested for summation in the ventricle. For
all patients, SI, S2, and Sc stimuli were introduced at the distal
bipolar pair, the pulse width of S, and S2 was 2.0 msec, and the
current used was twice late-diastolic threshold. The stimulator
used for the basic train and premature interval was set at a fixed
SS5 and SIS2 interval. The SIS2 interval was always 10 msec
less than the effective refractory period and S2 never produced a
ventricular response when delivered alone. With a separate current generator, one or two subthreshold stimuli, each of 2.0
msec duration, were introduced up to 6 msec before S2. If
ventricular depolarization occurred with S2 plus the subthreshold stimuli, S2 was tested again without Sc to ensure that S2 by
itself still did not result in ventricular depolarization; similarly,
the subthreshold stimuli were introduced without S2 to ensure
that they did not institute ventricular depolarization. Summation
was considered to be present when S2 plus subthreshold stimuli
produced ventricular depolarization but S2 or subthreshold stimuli alone did not.
Data from multiple surface and intracardiac leads were recorded on an oscilloscopic recorder (Electronics for Medicine
VR12) at a paper speed of 100 mm/sec and stored on a tape
recorder (Hewlett Packard No. 3968A). Electrocardiographic
surface leads were filtered at 0.1 to 20 Hz and signals from
intracardiac leads were filtered at 30 to 500 Hz.
Results
Ventricular inhibition. Eleven patients underwent
ventricular inhibition testing and their data are listed in
table 2. When the SI, S2, and SC were applied at the
distal bipolar pair all patients demonstrated inhibition
in the ventricle. For the entire group the maximum
mean ScS2 interval at which inhibition still occurred at
10 mA or less was 85 msec, with a range of 40 to 150
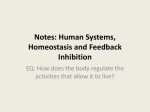
msec. Figure 1 illustrates analog data from one patient.
The S,S2 interval was 270 msec and this was held
constant for the entire study. Figure 1, left demonCIRCULATION
PATHOPHYSIOLOGY AND NATURAL HISTORY-ELECTROPHYSIOLOGY
TABLE 2
Electrophysiologic parameters
Longest S S2 interval (msec) at which S
SS
Patient PCL
ERP
No. (msec) (msec) (msec)
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Ventricle
1
500
290
300
2
500
240
250
3
500
240
250
4
600
230
250
5
500
260
270
6
500
240
250
7
600
250
260
S2 at:
Sc
site
IC
1.0
IC
1.5
IC
2.0
IC
2.5
IC
3.0
IC
3.5
IC
4.0
IC
4.5
IC
5.0
IC
6.0
IC
7.0
IC
8.0
IC
9.0
IC
10.0
NI
NI
40
NI
20
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
10
NI
NI
50
NI
NI
60
30
40
60
60
40
70
90
40
70
90
40
70
90
40
80
90
50
80
90
60
80
90
60
90
90
60
120
90
80
130
100
80
140
30
50
60
60
70
80
80
80
80
80
80
80
80
20
20
20
20
20
20
20
30
30
40
40
40
40
30
20
NI
40
40
30
70
60
30
70
70
40
80
70
50
80
90
50
90
90
60
120
120
60
150
120
60
150
130
60
150
130
60
150
130
60
150
130
70
NI
NI
NI
40
NI
40
NI
30
40
NI
30
50
NI
30
50
20
40
50
20
50
50
20
50
70
90
90
-
-
-
NI
40
NI
NI
50
60
60
90
60
20
20
30
30
30
50
50
50
60
90
90
90
90
NI
10
NI
20
NI
20
NI
30
NI
30
NI
30
NI
30
NI
30
NI
50
40
50
50
50
50
50
50
60
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
NI
20
NI
20
NI
NI
20
NI
20
NI
30
30
NI
30
30
40
30
NI
30
40
40
30
NI
30
40
50
40
NI
40
50
60
40
NI
50
60
70
70
NI
50
70
80
70
70
60
80
80
80
80
190
80
80
80
80
190
80
80
80
80
190
80
8
500
230
250
9
600
220
240
500
600
220
280
240
290
D
P
D
P
D
P
D
P
D
P
D
P
D
P
D
P
D
P
D
D
600
500
500
600
600
250
210
220
260
250
270
220
230
280
270
D
D
D
D
D
10
11
Atrium
7
8
9
12
13
inhibited
IC = inhibition current (mA of S,); PCL = pacing cycle length; ERP = effective refractory period; D = distal bipolar pair; P = proximal bipolar
pair; NI = no inhibition.
strates the maximum current for each Sc 2 interval at
which the conditioning stimulus did not inhibit S2'
while figure 1, right illustrates the minimum current at
which Sc always inhibited S2. As shown, more current
is needed for SC to inhibit S2 as S, precedes S2 at increasing intervals. The current of S, required to inhibit
S2 plotted as a function of the time at which S, precedes
S2 demonstrates a curvilinear relationship; the current
required for Sc to inhibit S2 varies directly as the SCS2
interval increases (figure 2). The maximum ScS2 interval at which Sc inhibits S2 is 150 msec, achieved at a
current of 6.4 mA. Currents of 6.6 to 10 mA did not
produce any greater degree of inhibition. In fact, for
the entire group of 11 patients, the maximum mean
ScS2 interval at which Sc still inhibited S
when currents
for Sc were less than 5 mA was 56 msec, with a range
of 0 to 110 msec. Therefore, approximately two-thirds
of the maximum ScS2 interval at which SC still inhibited S2 occurred at current strengths for Sc of 5.0 mA
or less.
Vol. 68, No. 4, October 1983
In nine patients the conditioning stimulus was applied at the proximal ventricular pacing pair and the S,
and S2 stimuli were applied at the distal pair. Six patients showed no inhibition at all during this pacing
protocol, and for all nine patients the maximum mean
ScS2 interval at which inhibition occurred with up to 10
mA current strength for S, was 26 msec, with a range
of 0 to 130 msec. The maximum mean S S2 interval
obtained with currents for Sc of 5.0 mA or less was 17
msec, with a range of 0 to 90 msec. As seen in figure 2,
Sc delivered at the proximal bipolar electrode pair inhibited S2 delivered at the distal pair less effectively
than when Sc and S2 were both delivered at the distal
bipolar pair. This relationship is even more dramatically demonstrated in figure 3, in which almost the entire
strength-interval inhibition curve using the proximal
bipolar pair for Sc was shifted upward and to the right.
We compared the effectiveness of inhibition of Sc
delivered at the proximal and distal electrode pair in
the three patients in whom inhibition occurred with the
709
PRYSTOWSKY and ZIPES
SC initiated at either the proximal or distal bipolar electrode pair. The mean maximum ScS2 inhibition interval
with currents of 10 mA or less for S was 113 msec
(range 90 to 150) with Sc at the distal electrode pair vs
77 msec (range 20 to 130) with Sc at the proximal
electrode pair. When S. was 5.0 mA or less, maximum
mean S S2 inhibition interval was 83 msec (range 50 to
110) vs 50 msec (range 20 to 90) with Sc at the distal
and proximal electrode pair, respectively. Thus, inhibition was much more effective when the Sc was applied nearer to the point at which S. was delivered.
Atrial inhibition. Atrial inhibition occurred in all five
patients tested. The maximum mean S S. interval at
which Sc still inhibited S, was 102 msec, with a range
of 80 to 190 msec. The maximum mean Sc 2 interval at
which Sc still inhibited S with S of 5.0 mA or less was
36 msec (range 0 to 50). In other words, a significant
portion of inhibition (65%) could be obtained as the
milliamperes of Sc exceeded 5.0 mA, in contrast to
results for ventricular inhibition.
Analog data from a typical experiment are shown in
figure 4 in a format similar to figure 1. Figure 4, left
illustrates, for each SCS2 interval, the maximum milliamperes of SC that still did not inhibit S2 and figure 4,
right illustrates the minimum milliamperes of SC that
always inhibited S2. Inhibition in this patient occurred
up to an SC2 interval of 150 msec. Figure 5 illustrates
graphically the relationship between milliamperes of
SC and the' SS2 interval.
III
SCS2 = 30
RV
S
USc
LS2
Sc=1 Ilm
Sc = 1.4mA
Sc
RV
=1.6mA
SCS2=80
Sc=3.8mA
Sc=3.6mA
RV
SCS2=130
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Sc= 5.6mA
Sc =5.4mA
SCS2 =150
RV
Sc=6.4mA
Sc=6.2mA
FIGURE 1. Inhibition of human ventricle (patient 5). The SI S2 interval
for this patient was 270 msec. Left, For each ScS2 interval the highest S,
(mA) at which no inhibition occurred. Right, The lowest Sc (mA) at
which S2 was inhibited. As the Sc52 interval increases the current of S,
needed to inhibit S2 increases. Time line intervals are 50 msec. RV
right ventricle.
10-
*
0
9-
*
0
8-
*
0
*
0
SlS2=270 msec
7-
* Distal Sc
o Proximal Sc
0
0
S
E
a822
5.-
0
co,
0
4-
0
3-
*g
2
2-
0
i
1I
E)
%R-
X
I
I
I
170 160 150 140
I
l
130 120 110
l
I
100
90
80
70
-I
l-II
60 50 40
I
30
I
20
SCS2 (msec)
FIGURE 2. Inhibition strength-interval curve for patient 5. When the proximal bipolar electrode pair is used to initiate SC
(unfilled circles) the maximum degree of inhibition of SC is 20 msec less than when the SC is initiated at the distal bipolar pair
(filled circles). See text for details.
710
CIRCULATION
PATHOPHYSIOLOGY AND NATURAL HISTORY-ELECTROPHYSIOLOGY
10-1
0
0
9-
0
0
S1S2=300 msec
* Distal Sc
8-
o Proximal
7-
6-
E
5-
co
4-
Sc
0
0
0
*
FIGURE 3. Ventricular inhibition as a function of
the site of the inhibitory stimulus in patient 1. This
curve demonstrates an upward and rightward shift
when SC is initiated at the proximal bipolar electrode
pair (unfilled circles) compared with at the distal pair
(filled circles).
c
3-
*
0
8
*
a
OD
2-
Iv.
I*
I
1
120 110
100
I
I
I
I
I
I
I
I
I
90
80
70
60
50
40
30
20
10
0
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
SC S2 (msec)
VI
S1 SC S2
SCS2
O
HRA1
ScS2
=30
A2
N
HRA2
Sc=3.OmA
Sc=2.8mA
SC
Sc
ScS2=
80
HRA2
Sc= 4.8mA
Sc= 5.OmA
SC
SC
Effects of SC on threshold. In patients 14 through 16 the
effect of SC on threshold of S2 was investigated. For all
patients, as the current of SC was increased to 10.0 mA
or less to inhibit S29 inhibition could be overcome by
the use of higher milliamperes for S2 (figure 6). Thus,
the threshold of S2 appeared to vary directly as a function of the magnitude of current used for SC.
Ventricular summation. Summation was present in
only one of six patients. One subthreshold stimulus
plus S2 never produced ventricular depolarization. In
one patient, two subthreshold stimuli caused summation (figure 7). In figure 7, A, at an S,S2 interval of 230
msec, S2 did not result in ventricular depolarization.
Figure 7, B shows no summation after two subthreshold stimuli initiated 6 msec (SIS3 224 msec) and 8 msec
(SIS4 222 msec) before S2' Summation is illustrated in
figure 7, C and it occurred when the second subthreshold stimulus was moved 1 msec closer to S2 (SIS4 223
msec).
HRA1
Sc
SCS2=120
HRA2
SC
Sc
Sc= 7.5mA
Sc=7.7mA
SC
SC
HRAl
ScS2= 150
HRA2
I
c
Sc= 9.8mA
Vol. 68, No. 4, October 1983
Sc= 10.0mA
Discussion
In this study we demonstrate that subthreshold stimuli can prevent subsequent threshold stimuli from depolarizing human atrium and ventricle, as noted earlier
in animal investigations." We further show that inhibition is both time and voltage dependent, and is markedly more effective if the inhibitory stimulus is delivered at the same site as the S2' These properties of
FIGURE 4. Inhibition of human atrium in patient 12. The format is;
similar to that of figure 1. Since Sc occurs progressively earlier before S2
more current is required for S2 to inhibit the atrium. HRA = high right
atrium.
711
PRYSTOWSKY and ZIPES
10-
.
9-
S1S2= 240 msec
80
0
7-
60-1.
E
0
5-
0
0
0
co,
40
3-
0
0
0
0
21-
0
fl.
I
I
I
I
I
I
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
170 160 150 140 130 120 110
.
I
I
I
100 90
I
80
I
70
60
50
-|
I
I
40
I
30
20
SCS2 (msec)
FIGURE 5. Inhibition strength-interval relationship in atrium of patient 12. Please note that in addition to an increased current of
SC required to inhibit S2 as the ScS2 interval progressively increases, a significant amount of inhibition occurs with currents for Sc
of more than 5 mA.
inhibition may be explained by several mechanisms
but are cc insistent with the possibility that S, electronically affe cts the response of the tissue to S2, thereby
preventin g S2 from initiating an active response.
Severa 1 studies5-'0 have shown that subthreshold
electrotor Pic depolarizations can exert inhibitory actions on iimpulse conduction as well as impulse generation in is(olated cardiac tissues. The inhibitory effects
on impulsse generation include the ability of subthreshold depol .arization to delay the scheduled discharge of
a spontanieous pacemaker' and the ability to annihilate or terminate pacemaker cycling.8 In a more recent
study'0 it was demonstrated that electrotonic interac4.0Patient Number
0
A
3.0-
14
16
a*16
CO)
-
E
2.0 -
1.0
.
10.0
8.0
6.0
mA
4.0
2.0
0
(Sc)
FIGURE 6. Threshold of S2 as a function of current for Sc. For each
patient, the points plotted represent the milliamperes of S2 needed to
depolarize tI he ventricle at various milliamperes of Sc. See text for more
detail.
712
tions resulting from a nonconducted response could
impair the transmission of an impulse arriving later in
time at a zone of depressed conductivity. Electrotonic
depolarizations exerted a graded voltage and time-dependent inhibitory effect on the conduction of subsequent beats. Specifically, a subthreshold stimulus
more effectively inhibited a threshold stimulus from
producing a response if it occurred closer in timing to
the threshold stimulus. At a fixed ScS2 interval, higher
voltage of the Sc stimulus caused more effective inhibition. Our observations in human myocardium parallel
these results. As noted in table 2 and figures 2, 3, and
5, the current of SC required to inhibit S2 is related to the
ScS2 interval. Furthermore, at a constant ScS2 interval,
the amount of current of S2 needed to depolarize the
ventricle increases as the milliamperes of SC increase.
Thus, it appears that S, inhibits S2 in part by modifying
myocardial excitability threshold.
Inhibition has also been demonstrated in branched
Purkinje fibers, the branch points of which were encased in high-K agar. II Under these conditions, excitation of the branch by a wave front arriving from one
end of the preparation could be inhibited by appropriately timed stimulation of the opposite end of the preparation. To explain this phenomenon of spatial inhibition it was suggested that stimulation of the inhibitory
end gives rise to an action potential that may invade
and die out in
some
fibers of the bundle. Those fibers
would then be unable to participate in the excitatory
response to which they would normally have contribut-
CIRCULATION
PATHOPHYSIOLOGY AND NATURAL HISTORY-ELECTROPHYSIOLOGY
c
B
VI'
HBE'
RV-
i
I {E I
I
11 1
FIGURE 7. Summation in the ventricle. Premature interval (S1S2) of 230 msec never by itself resulted in ventricular depolarization (A). Subthreshold stimuli 6 msec (SIS3) and 8 msec (S S4) before S2 plus S2 do not cause ventricular depolarization (B), but
when SIS4 is moved 1 msec closer to S2 ventricular activation occurs.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
ed. This mechanism, however, cannot adequately explain our observations since Sc stimuli well within the
refractory period of the myocardium tested were able
to inhibit S2 (figures 1 and 4). Under these conditions,
electrotonic displacement of membrane potential by Sc
is more likely than active invasion of surrounding tissue. Further work is needed to define the mechanism(s) responsible for electrotonic inhibition in myocardium. Additionally, our patients had a variety of
arrhythmias and most, but not all, had structural heart
disease; it is not known whether the results of this
study can be extrapolated to the general population.
Although inhibition occurred in all patients tested,
summation could be demonstrated in only one patient.
In this patient a total of three stimuli were necessary to
evoke a ventricular response, a finding noted earlier by
Tamargo et al.3
The findings in this study suggest potential clinical
applications for the use of subthreshold stimuli to prevent tachyarrhythmias in humans. It is possible that
atrial or ventricular arrhythmias may be prevented by
applying subthreshold stimuli to one or more areas of
the heart after a threshold depolarization (induced or
spontaneous) has occurred. For example, a patient
with a tachyarrhythmia may have the arrhythmogenic
focus identified during epicardial or endocardial mapping. A single electrode or an array of electrodes could
then be permanently placed at or near the focus, and a
pacemaker generator could deliver one or more subthreshold stimuli at a predetermined time after normal
Vol. 68, No. 4, October 1983
and/or premature complexes. Other investigators4 have
demonstrated a protective zone for ventricular fibrillation. In their studies a second stimulus delivered during a critical interval after a fibrillatory stimulus was
shown to protect against ventricular fibrillation. Our
data suggest that a similar protective zone may precede
the precipitating event.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Drury AN, Love WS: The supposed lengthening of the absolute
refractory period of frog's ventricular muscle by veratrine. Heart
13: 77, 1926
Lewis T, Drury AN: Revised views of the refractory period in
relation to drugs reputed to prolong it, and in relation to circus
movement. Heart 13: 95, 1926
Tamargo J, Moe B, Moe GK: Interaction of sequential stimuli
applied during the relative refractory period in relation to determination of fibrillation threshold in the canine ventricle. Circ Res 37:
534, 1975
Verrier RL, Lown B: Prevention of ventricular fibrillation by use
of low-intensity electrical stimuli. Ann NY Acad Sci 382: 355,
1982
Weidman S: Effect of current flow on membrane potential of cardiac muscle. J Physiol (Lond) 115: 227, 1951
Wennemark JR, Ruesta VJ, Brody DA: Microelectrode study of
delayed conduction in the canine right bundle branch. Circ Res 23:
753, 1968
Jalife J, Moe GK: Effect of electrotonic potentials on pacemaker
activity of canine Purkinje fibers in relation to parasystole. Circ
Res 39: 801, 1976
Jalife J, Antzelevitch C: Phase resetting and annihilation of pacemaker activity in cardiac tissue. Science 206: 695, 1979
Antzelevitch C, Moe GK: Electrotonically mediated delayed conduction and reentry in relation to "slow responses" in mammalian
ventricular conducting tissue. Circ Res 49: 1129, 1981
Antzelevitch C, Moe GK: Electrotonic inhibition of impulse transmission across inexcitable segments of cardiac tissue. Circulation
66 (suppl II): 11-358, 1982 (abst)
Cranefield PF, Hoffman BF: Conduction of the cardiac impulse. II.
Summation and inhibition. Circ Res 28: 220, 1971
713
Inhibition in the human heart.
E N Prystowsky and D P Zipes
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Circulation. 1983;68:707-713
doi: 10.1161/01.CIR.68.4.707
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1983 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/68/4/707.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/