Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hepatitis C wikipedia , lookup
Ebola virus disease wikipedia , lookup
Influenza A virus wikipedia , lookup
Oesophagostomum wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
West Nile fever wikipedia , lookup
Orthohantavirus wikipedia , lookup
Henipavirus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Marburg virus disease wikipedia , lookup
Potato virus Y wikipedia , lookup
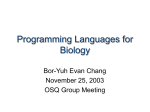
Clinical Infectious Diseases ANSWER TO THE PHOTO QUIZ Anthony Amoroso, Section Editor Progressive Right-Sided Hemiparesis in a Man With Sarcoidosis (See pages 1141–2 for the Photo Quiz.) Diagnosis: Progressive multifocal leukoencephalopathy (PML) due to John Cunningham (JC) virus. Pathologic demonstration of oligodendroglia with intranuclear inclusions, transformed astrocytes, and foamy macrophages suggested inflammatory demyelination induced by viral infection (Figure 1A). In situ hybridization of brain biopsy tissue revealed abundant JC viral DNA in oligodendroglial nuclei, and immunohistochemistry showed high expression of transforming T antigen in astrocytes (Figure 1B and 1C). These features are pathognomonic for PML and illustrate important aspects of JC viral pathophysiology. Only select cell types express the specific polysialic acid receptor for the JC virus. In the central nervous system, this receptor is found on astrocytes and oligodendroglial lineages. JC viral entry occurs via clathrin-mediated endocytosis and can also be facilitated by serotonin receptors (subtype 5HT2A). Cell entry is necessary but independently insufficient for productive viral replication. In PML, JC viral replication in glia via cellular transcription factors appears to require sequence variation (as compared to archetype virus) in the viral chromosome’s noncoding control region (NCCR), which contains promoter and enhancer elements [1]. NCCR variants permit early gene expression (including the large T antigen) in astrocytes, but preclude genes needed for viral replication. Therefore, astrocytes express high levels of the large T antigen (detected by immunohistochemistry and depicted in Figure 1C) and relatively little viral DNA (detected by in situ hybridization and depicted in Figure 1B). The expression of high levels of large T antigen overrides normal cycle checkpoints, giving the infected astrocytes a large bizarre or transformed morphology that simulates malignancy (Figure 1A and 1B). Conversely, the complement of transcription factors in oligodendroglia permits both early and late JC viral gene expression. Oligodendroglial lineage infection leads to a productive infection in which the virus replicates robustly, accumulating in the nucleus. These cells contain masses of viral DNA and label strongly by in situ hybridization (Figure 1B), whereas their expression of large T antigen is relatively weak (Figure 1C). The damage and death of oligodendroglia recruit macrophages to clear the myelin debris (Figure 1A). Diagnosis of PML is most frequently made following identification of JC virus by polymerase chain reaction (PCR) in cerebrospinal fluid (CSF) specimens from persons with compatible clinical and radiographic findings. Brain biopsy can provide confirmatory evidence when clinical and radiographic evidence is unconvincing [2] or when multiple pathologic processes are simultaneously present. In our case, plasma and CSF specimens were positive by PCR for JC virus (5393 copies/mL and 12 284 copies/mL, respectively); these results were obtained after brain biopsy was performed. Human immunodeficiency virus (HIV) antibody by immunoassay was negative. Prednisone was stopped and mirtazapine was initiated. Unfortunately, the patient’s neurologic symptoms progressed and he died 2 months after his brain biopsy was performed. Figure 1. A, Hematoxylin and eosin stain (×400 magnification) depicting oligodendroglia with intranuclear inclusions (arrowheads), transformed astrocytes (arrows), and foamy macrophages (clear cells). B, In situ hybridization depicting JC viral DNA in oligodendroglial nuclei (arrowhead); also shown is an unstained, transformed astrocyte (arrow). C, Immunohistochemical stain depicting transforming T antigen in astrocytes (arrows) and oligodendroglial cells (arrowheads). 1186 • CID 2016:62 (1 May) • ANSWER TO THE PHOTO QUIZ Persons with HIV infection and hematologic malignancies are at highest risk for PML, accounting for 90% of PML cases in one series [3]. However, in the pre-HIV era, patients with granulomatous disease—including sarcoidosis—accounted for an estimated 15% of all PML cases [4]. The theorized mechanism of immune depletion and resultant susceptibility to PML among patients with sarcoidosis involves lymphocyte sequestration, monocyte exhaustion, and regulatory T-cell dysfunction. Although iatrogenic immunosuppression likely increases the risk of PML in individuals with sarcoidosis, there are several reports of persons with sarcoidosis who developed PML in the absence of immunosuppressive therapy [5]. PML can be clinically mistaken for neurosarcoidosis, as was the case in this report. Several key characteristics distinguish the 2 conditions. Lesions due to PML tend to be subcortical and do not typically exhibit contrast enhancement, although faint enhancement can occasionally be seen along the margins of PML lesions and, when present, may suggest a more favorable prognosis. Neurosarcoid lesions can have a varied appearance, but are frequently enhancing and often involve dural and meningeal tissue. Pleocytosis and elevated protein are typically absent in patients with PML, in contrast to patients with neurosarcoidosis, whose CSF tends to be inflammatory with increased protein. This case highlights the importance of considering PML in the differential of neurosarcoidosis, and the accompanying neuropathology depicts important elements of JC viral pathogenesis. Notes Financial support. P. V. is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (award number KL2TR000146). Potential conflicts of interest. All authors: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. Alison L. Galdys,1 Hrishikesh A. Kale,2 David Lacomis,3 Pascalis Vergidis,1 and Geoffrey H. Murdoch4 1 Infectious Diseases Division, 2Radiology Department, 3Neurology Department, and 4Anatomic Pathology Division, University of Pittsburgh Medical Center, Pennsylvania References 1. Ferenczy MW, Marshall LJ, Nelson CD, et al. Molecular biology, epidemiology, and pathogenesis of progressive multifocal leukoencephalopathy, the JC virus-induced demyelinating disease of the human brain. Clin Microbiol Rev 2012; 25:471–506. 2. Berger JR, Aksamit AJ, Clifford DB, et al. PML diagnostic criteria: consensus statement from the AAN Neuroinfectious Disease Section. Neurology 2013; 80:1430–8. 3. Molloy ES, Calabrese LH. Progressive multifocal leukoencephalopathy: a national estimate of frequency in systemic lupus erythematosus and other rheumatic diseases. Arthritis Rheum 2009; 60:3761–5. 4. Richardson EP Jr. Our evolving understanding of progressive multifocal leukoencephalopathy. Ann N Y Acad Sci 1974; 230:358–64. 5. Jamilloux Y, Neel A, Lecouffe-Desprets M, et al. Progressive multifocal leukoencephalopathy in patients with sarcoidosis. Neurology 2014; 82:1307–13. Correspondence: A. L. Galdys, University of Pittsburgh Medical Center, 3601 Fifth Ave, Ste 150, Pittsburgh, PA 15213 ([email protected]). Clinical Infectious Diseases® 2016;62(9):1186–7 © The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail [email protected]. DOI: 10.1093/cid/ciw011 ANSWER TO THE PHOTO QUIZ • CID 2016:62 (1 May) • 1187