Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
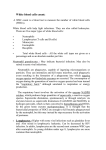
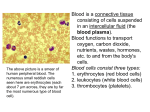
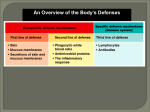
Review Monocyte and Macrophage Heterogeneity in the Heart Matthias Nahrendorf, Filip K. Swirski Abstract: Monocytes and macrophages are innate immune cells that reside and accumulate in the healthy and injured heart. The cells and their subsets pursue distinct functions in steady-state and disease, and their tenure may range between hours and months. Some subsets are highly inflammatory, whereas others support tissue repair. This review discusses current concepts of lineage relationships and crosstalk of systems, highlights open questions, and describes tools for studying monocyte and macrophage subsets in the murine and human heart. (Circ Res. 2013;112:1624-1633.) Key Words: healing ■ heart failure ■ macrophages Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 M ■ monocytes ■ myocardial infarction parenchymal cells in the heart while giving attention to other organ systems that are involved in cardiovascular disease. yocardial infarction (MI) inflicts a wound to the heart that, from the perspective of basic biology, shares many features with wounds resulting from trauma or surgery. A parallel between both is that the initial injury, whether traumatic or ischemic, initiates a general healing response of the body, which involves many organ systems in the task of restoring equilibrium and ensuring survival. Unlike many wounds resulting from trauma, MI is a form of sterile injury. Another distinction is that the wound in the heart is constantly subjected to the considerable strain of cardiac contractions. MI is one of the most frequent wounds in the United States because coronary syndromes occur once every 25 seconds.1 Certainly, it is one of the most lethal wounds. If it does not kill immediately, then MI may result in heart failure, a syndrome with high mortality.1 Increasingly, we understand that the healing process in the weeks after ischemia paves the road to either recovery or left ventricular dilation. Insufficient healing may lead to infarct expansion and trigger left ventricular remodeling. However, no therapeutic measures exist in the clinic to propagate healing and prevent heart failure. Wound healing that occurs after ischemic injury and that may result in heart failure should be explored from the perspective of the recent advances in understanding leukocyte biology. In particular, the improved knowledge of the role of monocytes, macrophages, and their subsets in steady-state and disease created new insight into heart failure evolution post-MI. Macrophages reside in the healthy heart and, although they may not be as frequent as myocytes, endothelial cells, and fibroblasts, their numbers are substantial2 and increase during disease.3,4 Their functions, especially in the steady-state and the remote zone after MI, remain elusive. Our review article focuses on these protagonist immune cells and examines their subsets, source, phenotype, fate, and function in the steady-state and disease. We discuss the potential interaction of monocytes and macrophages with Monocytes and Macrophages The existence of monocytes has been appreciated since at least the 1920s.5 The idea that monocytes derive from bone marrow precursors, circulate, and give rise to tissue macrophages was consolidated in the 1960s and has dominated much of our thinking since.6 A major characteristic of the model is that macrophage development follows a linear and spatially restricted trajectory. The model has been influential not only for what it proposes but also for what it excludes. Restricting promonocytes to the bone marrow, monocytes to the blood, and macrophages to the tissue precludes the existence of promonocytes outside the bone marrow, monocytes outside the blood, and macrophages outside tissue. Many studies, some also dating back to the 1960s, have provided evidence against these locational and ontogenic restrictions.7,8 Precursors can develop and give rise to monocytes outside the bone marrow in a process called extramedullary monocytopoiesis.9,10 The phenomenon is rare in the steady-state, increases during inflammation, and illustrates a previously unappreciated dynamic of cellular relocation. Studies also have shown that monocytes are not exclusively circulating but can reside in tissue as reservoirs for mobilization during inflammation.11 Moreover, there are vast transcriptional differences between classical macrophage populations in various tissues.12 Therefore, we may need to reexamine, at the functional level, in what ways various macrophages differ and in what ways they are similar. Recent studies show that many tissue macrophages in the steady-state do not derive from monocytes but from progenitors that have seeded tissue from the yolk sac before the development of definitive hematopoiesis.13–17 The work not only builds on previous studies that argued for the dual development of macrophages in the spleen8 but also provides Original received April 9, 2013; revision received May 7, 2013; accepted May 8, 2013. In April 2013, the average time from submission to first decision for all original research papers submitted to Circulation Research was 13.5 days. From the Center for Systems Biology, Massachusetts General Hospital and Harvard Medical School, Boston, MA. Correspondence to Matthias Nahrendorf, Center for Systems Biology, Massachusetts General Hospital, Harvard Medical School, Simches Research Building, 185 Cambridge St, Boston, MA 02114 (e-mail [email protected]); or Filip K. Swirski, Center for Systems Biology, Massachusetts General Hospital, Harvard Medical School, Simches Research Building, 185 Cambridge St, Boston, MA 02114 (e-mail [email protected]). © 2013 American Heart Association, Inc. Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.113.300890 1624 Nahrendorf and Swirski Cardiac Macrophages 1625 Nonstandard Abbreviations and Acronyms HSC IL MI hematopoietic stem cells interleukin myocardial infarction Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 mechanistic insight, showing the specific involvement of transcription factors Pu-1 and Myb. The nonhematopoietic origins of macrophages in tissues, such as brain, liver, lung, and spleen, raise a plethora of questions. What other locations contain nonhematopoietic macrophages? Are cardiac macrophages derived from local precursors? How are the various tissue macrophages similar, and how are they different? What is the identity of the tissue precursor, and how is it maintained throughout adult life? Intense investigation of these questions will no doubt reveal answers in the next few years. Monocytes are produced in the bone marrow in the steady-state from hematopoietic precursors. The most restricted monocyte progenitor known is the macrophage dendritic cell progenitor, which is developmentally downstream of granulocyte and macrophages progenitors and which shares many phenotypic features with the common dendritic cell progenitor.18,19 Monocytes produced in the bone marrow enter the blood via CCR2.20,21 In the mouse, circulating monocytes are phenotypically and functionally heterogeneous and can be separated according to Ly-6C expression. Between 50% and 60% of mouse monocytes in the steady-state belong to the Ly-6Chigh CCR2high CX3CR1low CD62L+ subset. These inflammatory or classical monocytes have a relatively short circulating life span and accumulate preferentially in inflammatory sites where they give rise to macrophages. The remaining Ly-6Clow CCR2low CX3CR1high CD62L− subset, sometimes referred to as nonclassical, patrols the vasculature and accumulates at low numbers in the steady-state.19,22 During inflammation, the number of Ly-6Chigh monocytes increases through increased monocytopoiesis in the bone marrow and spleen, contributing to monocytosis.9,10,23,24 The function of Ly-6Clow monocytes in tissue, however, requires further study because relatively few Ly-6Clow monocytes accumulate. Evidence shows that monocyte subsets do not arise from separate progenitors, but rather convert from the Ly-6Chigh to the Ly-6Clow subset.25–27 In humans, circulating monocytes also can be separated into subsets based on the expression of CD14 and CD16.28 Phenotypic profiling indicates that CD16− CD14+ monocytes, which comprise 80% to 90% of human monocytes, are similar to Ly-6Chigh monocytes, whereas CD14dim monocytes are most similar to Ly-6Clow monocytes.29,30 A third subset in humans can be identified as CD16+ CD14++.30,31 This subset, which circulates at a frequency of 5% to 7%, was originally called inflammatory because it produces tumor necrosis factor-α in response to lipopolysaccharide. The relationship between human CD16+ CD14++ monocytes and mouse subsets had been the subject of debate. CD16+ CD14++ cells share many phenotypic features with Ly-6Clow monocytes.30 Accordingly, the expression of CD16 is the division line; CD16− monocytes are akin to Ly-6Chigh monocytes, whereas CD16+ monocytes are most similar to Ly-6Clow monocytes. The opposing view argues that CD16+ CD14++ cells, which cluster with CD16− CD14++ monocytes, are closely associated with Ly-6Chigh monocytes.29 Here, the division line is CD14; CD14++ monocytes resemble Ly-6Chigh monocytes, whereas CD14dim monocytes resemble Ly-6Clow monocytes. Functionally, the patrolling CD14dim and Ly-6Clow monocytes are vascular sentinels. In that respect, they are macrophages of the blood.22 The fate of Ly-6Chigh monocytes on tissue accumulation also has received attention. A focus of much interest in macrophage biology is the particular function that macrophages acquire on tissue accumulation. In vitro, macrophages can be generated from bone marrow precursors by various means. Macrophages generated in the presence of interferon-γ or lipopolysaccharide have been termed M1, or classically activated inflammatory macrophages. Macrophages generated in the presence of interleukin (IL)-4 or IL-10, however, have been called M2, or alternatively activated macrophages, and have a proresolution profile.32,33 Although tissue and inflammatory macrophages likely are on a continuum that lies between (and outside of) the M1 and M2 definitions, the terminology nevertheless has been helpful in efforts aimed at elucidating macrophage heterogeneity. When Ly-6Chigh monocytes infiltrate atherosclerotic lesions, for example, they differentiate to F4/80+ and Mac3+ macrophages. In lesions in which the inflammatory stimulus is persistent, these Ly-6Chigh monocyte– derived macrophages remain inflammatory by expressing IL-1β and tumor necrosis factor-α and by contributing to oxidative stress.9 In this respect, Ly-6Chigh monocyte–derived macrophages are M1 macrophages. In the context of inflammation resolution, M1 macrophages are replaced by M2 resolution–mediating macrophages. It has been proposed that this occurs through local M1 to M2 conversion.34–36 M2 macrophages also could derive from less inflammatory Ly-6Clow monocytes. Alternatively, M2 macrophages may arise through direct differentiation of Ly-6Chigh monocytes in a microenvironment that favors resolution (Figure 2). This possibility should be explored experimentally because it is enticing for several reasons. First, the macrophage turnover kinetics in the infarcted myocardium are remarkably fast. This suggests that newly recruited cells are continuously replacing old cells. Second, recent evidence indicates that Ly-6Clow monocytes function predominantly as vascular sentinels and infiltrate tissue at very low frequencies. Third, in the steady-state, Ly-6Clow monocytes derive from Ly-6Chigh monocytes, and it is not clear whether the conversion path involves intermediate stages, that is, Ly6Chigh monocyte to Ly-6Clow monocyte to M2 macrophage. Sophisticated lineage-tracing studies are therefore required to elucidate monocyte/macrophage lineage relationships during resolution of inflammation in the ischemic myocardium, testing the hypothetical options outlined in Figure 2. Infarct Healing The typical trigger of MI is plaque rupture in a coronary artery, which suddenly stops the arterial blood flow feeding downstream organ areas. Deprived of oxygen, the nonperfused myocardial tissue undergoes necrosis. Accumulation of leukocytes in the first minutes to hours after MI was 1626 Circulation Research June 7, 2013 Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 recently imaged with intravital microscopy for the first time.37,38 Surprisingly, monocyte recruitment may outpace neutrophils soon after coronary ligation.38 Nevertheless, neutrophils are the first leukocyte population to reach a robust peak of several hundred-thousand cells within the first day after onset of ischemia.3 The short-lived cells are recruited through adhesion molecules, such as E-selectin, P-selectin, and ICAM-1, and the chemokine IL-8.39 The presence of neutrophils is generally seen as detrimental because it contributes to the damage inflicted by reperfusion injury. Their main function is to defend the organism against invaders such as microbes. To fulfill this task, they carry an armamentarium of inflammatory cytokines, are phagocytic, and impose oxidative stress on the tissue in which they accumulate. Their presence in the healing infarct wanes quickly, but they may linger longer if inflammation does not resolve. Some of these cells can be found in the cardiac wound as late as 7 days after MI. The next major cell classes dominating the infarct are monocytes and macrophages. These myeloid cells can be found in high numbers, up to a million cells, in the infarct. An inflammatory phenotype (Ly-6Chigh monocytes/M1-type macrophages) dominates initially and is followed by cells with a lesser inflammatory phenotype promoting tissue repair (Ly-6Cint/low monocytes/M2-type macrophages). These cells are discussed in more detail in the following paragraphs. Other leukocytes invading the infarct include dendritic cells,40 lymphocytes,41,42 and mast cells.43 Compared with neutrophils, monocytes, and macrophages, their numbers are lower. However, they may have an important role in regulating infarct healing and the myeloid cell response. When the inflammatory activity resolves, nonleukocyte cells join the rebuilding activities in the infarct. Solicited by angiogenic factors, such as vascular endothelial growth factor, numerous vessels sprout into newly forming granulation tissue. These small capillaries can appear as early as a few days after injury, but their highest numbers are found weeks later. In nonreperfused infarcts, the highest density of neovessels is observed in the border zone, that is, next to noninfarcted tissue. Initially, new vessels only consist of endothelial cells but acquire a more mature morphology, including a pericyte coat, over time.44 Myofibroblasts produce collagen, the extracellular matrix that strengthens the emerging infarct scar. Impaired collagen deposition or accelerated degradation of collagen attributable to high matrix metalloproteinase activity45 can lead to infarct rupture and sudden death. Infarct expansion is a less drastic but still detrimental phenotype of insufficient matrix generation.46 Hence, collagen-producing cells play a major role in later stages of wound healing. Because parabosis studies linking row) is faster than recruitment of GFP+ cells in a LysMGFP/+ wild-type mice after coronary ligation with GFP+ mice have argued that circulating progenitors only give rise to leukocytes in the infarct,47 α-smooth muscle actin–positive cells may derive from local progenitors, for instance the very numerous resident cardiac fibroblasts. Monocytes in the Infarct Monocytes are among the very first cells recruited to ischemic myocardium. Intravital microscopy of the beating mouse heart37,38 allows the following of leukocyte action in the ischemic heart with high temporal and spatial resolution in vivo. Monocyte recruitment outpaced neutrophils within the first 30 minutes after the onset of ischemia (Figure 1).38 It is currently not clear which monocyte subset is recruited during the first minutes after MI or what the function of these cells entails. However, one could hypothesize that these are patrolling Ly6Clow monocytes that amplify the initial inflammatory signal. Discriminating monocyte subsets by imaging will contribute to a better understanding of their phenotype, source, and function. Two sequential phases defined by the expression of Ly-6C on monocytes/macrophages can be identified in the infarcted myocardium.3 The inflammatory Ly-6Chigh monocyte subset is recruited during the first days after MI via the chemokine monocyte chemotactic protein-1.48 Days later, when inflammation resolves in the cardiac wound, the presence of these inflammatory cells wanes. Starting at approximately day 4 after MI, the infarct tissue accumulates Ly-6Cint/low monocytes/ macrophages (Figure 2). On day 7, Ly-6Cint/low F4/80high cells outnumber Ly-6Chigh cells in the heart.3 Similar monocyte kinetics can be observed in the blood of mice after coronary ligation3 and in patients with acute MI.49 This time course corresponds to expression of M1-type markers in the tissue early after injury and M2-type macrophage markers later.50 Interestingly, the turnover of myeloid cells in the infarct is very rapid. Even days after injury, monocytes are recruited at a rather high rate and reside only for an average of 20 hours in the cardiac wound.10 Thereafter, most of them become apoptotic. Although only between 5% and 13% of the entire accumulating CD11b+ leukocyte population exits the infarct within 24 hours, some of these cells accumulate in the liver, lymph nodes, and the spleen.10 It is currently unknown whether cells that exit the site of inflammation do so actively or whether they merely perish elsewhere. Alternatively, they may have a specific function, for instance, transmitting information to sites of monocyte production. Within the first week of injury, the function of myeloid cells changes over time. During day 1 to 4 after ischemia, the milieu is highly inflammatory. Ly-6Chigh monocytes have a high payload Figure 1. Intravital microscopy of monocyte and neutrophil recruitment in the first 30 minutes after myocardial infarction in green fluorescent protein (GFP) reporter mice. Dedicated image stabilization and motion compensation techniques allowed following of this process in vivo. Interestingly, within the first 30 minutes after injury, the recruitment of monocytes in a transgenic mouse in which GFP reports on monocytes (top mouse (bottom row and graph on the right). Adapted from Jung et al.38 Nahrendorf and Swirski Cardiac Macrophages 1627 Advanced flow cytometry gating strategies, and new surface markers,12 together with a higher number of channels available in current flow cytometers, enable better discrimination between tissue monocytes and macrophages. Lineage Relationships in the Infarct Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 Figure 2. Potential lineage relationships of monocytes and macrophages after myocardial infarction. In steady-state, monocyte conversion from Ly-6Chigh to Ly-6Clow may occur in blood and bone marrow.27 It is generally accepted that Ly-6Chigh monocytes give rise to inflammatory M1 macrophages in tissue. Other lineage relationships, indicated by dashed arrows, remain to be experimentally explored in the setting of acute myocardial infarction. of inflammatory cytokines, such as tumor necrosis factor-α and proteases.3 Together with inflammatory macrophages, they form a demolition crew that digests dead cells and extracellular matrix. These cells clear the infarct of debris by phagocytosis, a prerequisite for replacing the injured tissue with granulation tissue and the evolving scar. An unresolved question is whether this debris is removed from the heart to distant organs or recycled onsite. During the following rebuilding phase, the inflammatory activity resolves and gives way to Ly-6Cint/low monocytes/macrophages. These cells have a lower content of inflammatory molecules and proteases. Instead, they release vascular endothelial growth factor and transforming growth factor-β, supporting angiogenesis and collagen production. Both healing phases are required for sufficient wound healing. If either is ablated, then the scar-building process is disturbed.3 Monocytes and macrophages may influence tissue regeneration in yet to be discovered ways. Work on the hematopoietic stem cell (HSC) niche illustrates that macrophages can have close relationships with multipotent progenitor cells.51,52 Recent insight highlights their role in regulating production of red blood cells.53 These regulatory macrophage actions are based on crosstalk with HSCs in the bone marrow. It is tempting to speculate that macrophages could act similarly in other tissues, for instance, by interacting with cells that have regenerative capacities in the injured heart. Specifically, macrophage subsets may differentially influence activity of proliferating endothelial cells, fibroblasts, endogenous cardiac progenitors, or stem cells that were transferred into the heart with the intention to rebuild myocardium after MI. The latter point may guide timing of cell therapy, because an inflammatory milieu provided by M1 macrophages could hinder survival, differentiation, and integration of therapeutically transferred cells. It is currently unclear how monocytes and macrophages share the burden of work because of the difficulties when trying to clearly separate the cell populations using surface markers. Although evidence for lineage relationship in the infarcted myocardium is rather sparse, there is considerable evidence in other tissues regarding how monocyte subsets and macrophages correspond to each other developmentally. The emerging picture is as follows: in the steady-state, the tissue is populated by resident macrophages, many of which do not rely on the bone marrow for replenishment but rather selfrenew from local progenitors or through proliferation.16 This has not yet been explored specifically for macrophages in the heart. Soon after injury, Ly-6Chigh monocytes infiltrate the infarct in large numbers.3 Many of these monocytes may not differentiate to macrophages but either exit or die in tissue. Those that differentiate acquire M1-like properties, continue to express Ly-6C, and contribute to inflammation (Figure 2). Over time, as inflammation gives way to resolution, a second Ly-6Cint/low phase emerges. We need to address experimentally whether macrophages dominating this regenerative wound healing phase arise via the differentiation of Ly-6Chigh monocytes (Figure 2) and less via differentiation of Ly-6Clow monocytes or local M1 to M2 macrophage conversion. Over time, as inflammation completely subsides, a population of F4/80high macrophages resembling steady-state macrophages returns. Future studies will determine whether these macrophages derived from a circulating or local precursor. Sources of Monocytes After MI The bone marrow is the primary site of production for blood cells. The production of leukocytes is tightly regulated by a team of housekeeping cells forming the hematopoietic niche. Key constituents include CD169+ macrophages, mesenchymal stem cells, osteoblasts, and endothelial cells. These niche cells organize HSC retention and provide signals that regulate proliferation or quiescence of HSCs via adhesion molecules (eg, selectins) and soluble cytokines (eg, CXCL12, stem cell factor).51,52 Release of monocytes from the bone marrow into the blood stream depends on the chemokine receptor CCR2,20 which also regulates recruitment to the site of inflammation.48 The infarct recruits these cells from the blood stream. Within the first 24 hours after coronary ligation in mice, approximately half of all monocytes recruited to the heart derive from a splenic reservoir.11 Reservoir monocytes reside in the subcapsular red pulp of the spleen and closely resemble their circulating counterparts, which they outnumber significantly. Upon MI, splenic monocytes increase motility, at least partially, by signaling of angiotensin-2 through the angiotensin-2 subtype-1 receptor expressed on their cell surface.11,54 The cells then intravasate into splenic veins and leave the organ (Figure 3) to accumulate at inflammatory sites. In mice, this leads to a drastic shrinkage of the spleen within the first 24 hours after MI. The organ weight declines by ≈50%, and so does the number of splenic monocytes. The bone marrow and blood pool also substantially contribute to the monocytes recruited to the infarct. 1628 Circulation Research June 7, 2013 Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 Figure 3. Intravital microscopy of the spleen in a CX3CR1GFP/+ mouse soon after myocardial infarction shows intravasation and departure of a splenic monocyte. Adapted from Swirski et al.11 Because the residence time of monocytes and macrophages is short, and because recruitment to the infarct continues at levels of several hundred-thousand cells per day, the production of these cells intensifies to meet the high demand after the reservoirs exhaust. We55 and others56 observed that MI increases the activity of the hematopoietic system. In humans, increased bone marrow uptake of the positron emission tomography tracer 18F-fluorodeoxyglucose, a radiolabeled glucose analog, indicates a higher metabolic activity.56 The human bone marrow releases hematopoietic progenitors after MI.57 In mice after coronary ligation, these cells home for the spleen, where they seed the organ depending on very late antigen 4 and stem cell factor to initiate extramedullary hematopoiesis.55 This monocyte production is stimulated by signaling through the IL-1 receptor, replenishes the splenic reservoir by day 6 after MI, and continues to supply the infarct with a significant number of cells (≈50% of infarct monocytes in mice derive from the spleen on day 6 after coronary ligation).10 Sympathetic nervous signaling is a trigger of bone marrow stem cell release after MI. Treatment with a β3-specific adrenoreceptor inhibited the release of HSCs into the blood.55 These findings raise the question of whether β-blockers in clinical use with affinity to the β3-receptor subtype inhibit HSC release in patients after MI, and perhaps have an anti-inflammatory effect by reducing extramedullary production of inflammatory leukocytes. Monocytes and Macrophages in Normal and Failing Myocardium Macrophages reside in many normal tissues during steady-state. The heart is no exception.2,3 Improved detection strategies, including fluorescent reporter proteins, visualize these cells nestled within the normal myocardium in direct contact with endothelial cells and myocytes.2 During steady-state, their gene expression profile resembles noninflammatory M2 macrophages.2 The number of extravasated monocytes in the healthy heart is low. However, monocytes can be found patrolling the myocardial vasculature.38 The patrolling behavior was previously described for Ly-6Clow monocytes in other tissues.22,58 The precise function of patrolling monocytes and tissue macrophages in the heart is currently unclear. What is the role of myocardial monocytes and macrophages in disease, ie, in the failing heart? Their increased presence in the myocardium has recently been described in mice with heart failure due to pressure overload59 and in the remote zone after MI in mice and patients (Figure 4).60,61 It is wellknown that myocyte hypertrophy, myocyte death, changes in the balance of extracellular matrix production and protease activity are central in the evolution of heart failure, but the role of monocytes and macrophages within this system is not well-understood. Specifically, we lack knowledge about their origin, phenotype, and function in failing hearts. Leukocyte numbers in the remote myocardial tissue are orders of magnitude lower compared with the acutely ischemic infarct. Nevertheless, an interesting hypothesis is that monocytes and macrophages may instruct and interact with parenchymal cells in the myocardium (Figure 4). The importance of macrophages in many other diseases is well-recognized.62,63 For instance, myeloid cells digest extracellular matrix and promote tissue destruction in atherosclerosis4,64,65 and rheumatoid arthritis,66,67 and they instigate fibrosis in liver disease.68 Hence, it is conceivable that these cells have an active role in the evolution of heart failure by supplying profibrotic signals or enhancing protease activity and ventricular dilation. Inflammatory macrophages may even accelerate myocyte apoptosis in failing hearts. Alternatively, these cells may be innocent bystanders or merely dispose of apoptotic myocytes. Clinical signs of inflammation in heart failure patients, such as increased C-reactive protein, high cytokine levels,69,70 and the predictive value of the white blood count71,72 underscore the likelihood of an inflammatory component in left ventricular remodeling. Future research should address the mode of recruitment, whether there is local macrophage proliferation in the failing heart, the function of leukocytes in the remote myocardium, and their interaction with endothelial cells, myocytes, and fibroblasts (Figure 4). Crosstalk Between Organ Systems The heart is intimately linked to all organ systems. On the obvious side, it supplies the entire body with oxygenated blood. A decline of this function compromises the function of other organs, possibly enhancing heart failure in a vicious cycle. Renal function is a prominent example, because decreased perfusion of the kidneys causes fluid retention and increases stress on the heart due to increased loading conditions. Similar connections may exist between the cardiovascular and the metabolic, endocrine, immune, and hematopoietic systems, and these interactions may enhance heart failure. Monocytes and macrophages closely link atherosclerosis and MI with the immune and hematopoietic systems. Derailed defense functions of macrophages, which fail to remove lipid deposits from the diseased arterial wall, lead Nahrendorf and Swirski Cardiac Macrophages 1629 Tools to Study Monocytes and Macrophages in the Heart Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 Figure 4. Open questions about the phenotype, behavior, and function of monocytes and macrophages in the remote zone after myocardial infarction (MI). The lower right inset shows immunoreactive staining for CD68+ macrophages in the remote zone of a patient who died soon after MI. Adapted from Lee et al.61 to inflammatory complications of atherosclerotic plaque. Aberrant cholesterol handling enhances the production of leukocytes in the bone marrow73 and, at least in mice, initiates extramedullary myelopoiesis in the spleen.9,74 In humans, increased activity of macrophages gives rise to vulnerable plaques, plaque rupture, and MI. Thus, MI occurs in a setting of chronic inflammation, with elevated activity of the hematopoietic and immune systems. The increased availability of inflammatory leukocytes attributable to preexisting atherosclerosis changes the inflammatory response to acute infarction and modulates myocardial healing. In apolipoprotein E−/− mice with atherosclerosis, inflammatory leukocytes are recruited for a longer time and in higher numbers to the cardiac wound, disturbing the resolution of inflammation in the heart and enhancing postMI remodeling.75 There is another perspective to this interaction of chronic inflammation in the artery wall and acute inflammation in the infarct. We have long known that the first year after an ischemic event is particularly dangerous, and that many patients experience reinfarction.76,77 A systemic flare-up of inflammation in the vessel wall after MI may cause these secondary ischemic events.78 Increased activity of the sympathetic nervous system translocates leukocyte progenitors to the spleen and accelerates overall production of inflammatory leukocytes.55 These cells not only are available for recruitment to the infarct but also may increase inflammatory activity in atherosclerotic plaque. Hence, it seems reasonable to target the nervous, immune, or hematopoietic systems to either prevent reinfarction or ameliorate the evolution of post-MI heart failure. This concept is already implemented to some degree, ie, by using beta-blockers, lowering blood cholesterol levels, controlling obesity, and treating diabetes mellitus. However, current clinical therapeutics do not specifically target inflammatory feedback loops. Although the first histochemical studies reported on leukocyte and macrophage presence in acute infarcts,79 a number of newer tools enabled analysis of leukocyte subsets, increased sensitivity, resulted in quantitative data, and facilitated in vivo measurements. Flow cytometric analysis of digested infarcts was a major advance, because this approach enumerates the total cell number per unit of tissue. Multichannel capabilities allow staining for surface marker combinations, hence the identification and isolation of monocyte subsets. The use of CX3CR1GFP reporter mice improved the sensitivity of ex vivo histology.2,61 In vivo microscopy of monocytes reported on the distinct migration paths and patterns of the cell. For instance, it revealed the increased motility of splenic monocytes after MI (Figure 3). Imaging the heart with microscopic resolution has only recently been established (Figure 1), because the cardiac and respiratory motions represent major hurdles. These were overcome by using tissue stabilization in conjunction with ECG and respiratory triggering of image acquisition.37,38 Organlevel imaging modalities, including MRI,80 positron emission tomography,61 fluorescence molecular tomography,81 and hybrid approaches,82 can now follow monocyte and macrophages and their molecular function in murine infarcts noninvasively (Figure 5). Noninvasive leukocyte imaging answered questions Figure 5. Noninvasive imaging of monocytes and macrophages. Left, top, Hybrid fluorescence molecular tomography/X-ray computed tomography imaging of protease activity in an apolipoprotein E−/− mice after coronary ligation (adapted from Panizzi et al75). Right, top, Positron emission tomography/MRI in a mouse with acute myocardial infarction using a macrophage-avid, copper-64–labeled cross-linked iron oxide nanoparticle (64Cu-CLIO; adapted from Majmudar and Nahrendorf95). Bottom, left, T2*-weighted MRI after injection of macrophage-avid iron oxide nanoparticles (adapted from Nahrendorf et al81). Bottom, right, Imaging of macrophages in a patient with acute MI (adapted from Yilmaz et al87). 1630 Circulation Research June 7, 2013 about how monocyte and macrophage content in the infarct influences left ventricular remodeling and the evolution of heart failure. Monocyte and macrophage imaging may rely on nanoparticles that are taken-up by these cells and that can be detected noninvasively. These include positron emission tomography isotope–labeled nanoparticles,83 fluorochromelabeled nanoparticles,81 gadolinium84–labeled or fluorine-1985– labeled liposomes, and iron oxide nanoparticles that are detectable with T2*-weighted MRI.80 First pioneered for this application in the mouse,80 iron oxide nanoparticles were recently used in 2 clinical trials focusing on macrophages in acute infarcts.86,87 These imaging tools will likely enable clinical studies that aim to translate basic findings and will follow emerging therapeutics that target monocyte and macrophage biology. Clinical Translatability Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 What is the evidence that discoveries in the mouse translate to patients with MI? A large number of clinical studies support concepts of cardiac monocyte and macrophage heterogeneity recently described in mice. Studies have shown, for example, that CD14++CD16+ monocytes predict cardiovascular events.88–90 However, seemingly conflicting data91 as well as lack of consensus regarding how human and mouse subsets correspond impede translation of mechanistic insights. Although tissue data in the heart are still lacking, a 2-phase monocyte response has been observed in the blood of patients after MI.49 Inflammatory CD14+CD16− monocytes peaked on day 3, whereas CD14+CD16+ monocytes peaked on day 5 after MI, recapitulating the temporal pattern observed for Ly-6Chigh and Ly-6Clow monocytes in mice.3 Patients with a higher blood level of inflammatory monocytes had worse myocardial salvage and lower ejection fraction 6 months after MI, measured by MRI.49 This intriguing study does not yet answer the question of causality in patients. Possibly, increased inflammatory activity leads to worse healing and outcome. Alternatively, a more extensive injury may have caused higher blood monocyte levels and lower ejection fraction 6 months later. A number of clinical studies confirm the correlation of blood leukocyte levels in heart failure with prognosis.71,72 Although many open questions persist, there are also some intriguing clues regarding the response of the hematopoietic system in patients after MI. An increased level of hematopoietic progenitors was found in the blood,57 and the metabolic activity of the bone marrow increased.56 There is also evidence for an increased progenitor activity in the spleen of patients after MI.55 Future studies will show whether there is splenic monocyte release in patients with MI, and whether biphasic monocyte recruitment can be observed in infarct tissue. The presence of macrophages in the remote myocardium after MI has been confirmed in patients by histology61 and in a macrophage imaging study.56 However, their function remains to be elucidated. Open Questions We are beginning to better understand the role of monocytes, macrophages, and their subsets in the heart, but there are more questions than answers. The role of these cells in the healthy heart is unclear. After MI, we do not yet understand what signals initiate the resolution of inflammation in the cardiac wound. Newer microscopic imaging techniques may soon better elucidate how monocytes are recruited to the injured heart, especially when the endothelium is disrupted. We have never seen a monocyte or macrophage move from the border zone into the core of an infarct, although we have found these cells there. What are their migration patterns, how do the cells move, and how fast? The high turnover of leukocytes in the infarct obviates the importance of leukocyte supply and production. Only few studies have investigated how the hematopoietic system, including the bone marrow, reacts to MI. Given the distance of organs such as the spleen and the bone marrow from the heart, it would be interesting, also as a possible way of interacting therapeutically with the inflammatory response, to learn more about the signals that regulate monocyte supply. What are the danger signals that report cardiac injury to other organ systems, including the spleen and the bone marrow? Although macrophages are present in the remote zone after MI and in mice with pressure overload, it is unclear whether they are important and what functions they pursue. Finally, from a perspective of monocyte and macrophage heterogeneity, precise lineage relationships between these cells and their subsets have yet to be determined in the steady-state as well as in the diseased heart. Conclusion The motivation behind the questions is the need for new treatment concepts in heart failure. We should also explore how our current therapeutics interfere with monocyte and macrophage function. For example, monocyte progenitor release from the bone marrow after coronary ligation in mice depends on β-adrenergic signaling. Furthermore, angiotensin-converting enzyme inhibition decreases monocyte and macrophage numbers in the infarct of mice by inhibiting the mobilization of splenic monocytes. Are similar mechanisms active in patients? Newer therapeutic avenues may target the inflammatory activity after MI directly. There are 2 major clinical atherosclerosis trials underway exploring the role of the antiproliferative drug methotrexate92 and the action of neutralizing IL-1β,93 a cytokine that likely supports post-MI monocyte production in the spleen.10 These trials may provide important cues regarding the role of monocyte and macrophage activity in patients. Finally, understanding the signaling pathways and the fate of monocytes and their progenitors after MI will support the search for specific therapies. One example is RNAi silencing of the chemokine receptor CCR2, which inhibits the recruitment of inflammatory monocyte subset in mice with MI,82,94 possibly sparing noninflammatory monocyte and macrophage subsets. Any potential immune-targeted therapy will face scrutiny about unwanted effects. However, targeting a culprit subset, motivated by increased knowledge of monocyte and macrophage heterogeneity, may spare important immune functions, such as repair and defense against infection. Nahrendorf and Swirski Cardiac Macrophages 1631 Acknowledgments The authors acknowledge Servier Medical Art for help in producing figures. Sources of Funding This work has been funded in whole or in part with federal funds from the National Heart, Lung, and Blood Institute, the National Institutes of Health, and the Department of Health and Human Services (R01HL095612, R01HL095629, R01HL096576, Contract No. HHSN268201000044C). Disclosures None. References Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 1. Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart Disease and Stroke Statistics—2010 Update. A report from the American Heart Association. Circulation. 2010;121:948–54. 2.Pinto AR, Paolicelli R, Salimova E, Gospocic J, Slonimsky E, Bilbao-Cortes D, Godwin JW, Rosenthal NA. An abundant tissue macrophage population in the adult murine heart with a distinct alternativelyactivated macrophage profile. PLoS One. 2012;7:e36814. 3.Nahrendorf M, Swirski FK, Aikawa E, Stangenberg L, Wurdinger T, Figueiredo JL, Libby P, Weissleder R, Pittet MJ. The healing myocardium sequentially mobilizes two monocyte subsets with divergent and complementary functions. J Exp Med. 2007;204:3037–3047. 4.Swirski FK, Nahrendorf M. Leukocyte behavior in atherosclerosis, myocardial infarction, and heart failure. Science. 2013;339:161–166. 5.Sabin FR, Doan CA. The relation of monocytes and clasmatocytes to early infection in rabbits with bovine tubercle bacilli. J Exp Med. 1927;46:627–644. 6.van Furth R, Cohn ZA. The origin and kinetics of mononuclear phagocytes. J Exp Med. 1968;128:415–435. 7. Goodman JW, Hodgson GS. Evidence for stem cells in the peripheral blood of mice. Blood. 1962;19:702–714. 8. van Furth R, Diesselhoff-den Dulk MM. Dual origin of mouse spleen macrophages. J Exp Med. 1984;160:1273–1283. 9.Robbins CS, Chudnovskiy A, Rauch PJ, et al. Extramedullary hematopoiesis generates Ly-6C(high) monocytes that infiltrate atherosclerotic lesions. Circulation. 2012;125:364–374. 10. Leuschner F, Rauch PJ, Ueno T, et al. Rapid monocyte kinetics in acute myocardial infarction are sustained by extramedullary monocytopoiesis. J Exp Med. 2012;209:123–137. 11. Swirski FK, Nahrendorf M, Etzrodt M, Wildgruber M, Cortez-Retamozo V, Panizzi P, Figueiredo JL, Kohler RH, Chudnovskiy A, Waterman P, Aikawa E, Mempel TR, Libby P, Weissleder R, Pittet MJ. Identification of splenic reservoir monocytes and their deployment to inflammatory sites. Science. 2009;325:612–616. 12. Gautier EL, Shay T, Miller J, et al; Immunological Genome Consortium. Gene-expression profiles and transcriptional regulatory pathways that underlie the identity and diversity of mouse tissue macrophages. Nat Immunol. 2012;13:1118–1128. 13. Ginhoux F, Greter M, Leboeuf M, Nandi S, See P, Gokhan S, Mehler MF, Conway SJ, Ng LG, Stanley ER, Samokhvalov IM, Merad M. Fate mapping analysis reveals that adult microglia derive from primitive macrophages. Science. 2010;330:841–845. 14. Hoeffel G, Wang Y, Greter M, et al. Adult Langerhans cells derive predominantly from embryonic fetal liver monocytes with a minor contribution of yolk sac-derived macrophages. J Exp Med. 2012;209:1167–1181. 15. Schulz C, Gomez Perdiguero E, Chorro L, Szabo-Rogers H, Cagnard N, Kierdorf K, Prinz M, Wu B, Jacobsen SE, Pollard JW, Frampton J, Liu KJ, Geissmann F. A lineage of myeloid cells independent of Myb and hematopoietic stem cells. Science. 2012;336:86–90. 16.Hashimoto D, Chow A, Noizat C, et al. Tissue-resident macrophages self-maintain locally throughout adult life with minimal contribution from circulating monocytes. Immunity. 2013;38:792–804. 17. Wynn TA, Chawla A, Pollard JW. Macrophage biology in development, homeostasis and disease. Nature. 2013;496:445–455. 18. Auffray C, Sieweke MH, Geissmann F. Blood monocytes: development, heterogeneity, and relationship with dendritic cells. Annu Rev Immunol. 2009;27:669–692. 19.Geissmann F, Manz MG, Jung S, Sieweke MH, Merad M, Ley K. Development of monocytes, macrophages, and dendritic cells. Science. 2010;327:656–661. 20.Serbina NV, Pamer EG. Monocyte emigration from bone marrow during bacterial infection requires signals mediated by chemokine receptor CCR2. Nat Immunol. 2006;7:311–317. 21. Tsou CL, Peters W, Si Y, Slaymaker S, Aslanian AM, Weisberg SP, Mack M, Charo IF. Critical roles for CCR2 and MCP-3 in monocyte mobilization from bone marrow and recruitment to inflammatory sites. J Clin Invest. 2007;117:902–909. 22.Carlin LM, Stamatiades EG, Auffray C, Hanna RN, Glover L, Vizcay-Barrena G, Hedrick CC, Cook HT, Diebold S, Geissmann F. Nr4a1-dependent Ly6C(low) monocytes monitor endothelial cells and orchestrate their disposal. Cell. 2013;153:362–375. 23. Swirski FK, Libby P, Aikawa E, Alcaide P, Luscinskas FW, Weissleder R, Pittet MJ. Ly-6Chi monocytes dominate hypercholesterolemia-associated monocytosis and give rise to macrophages in atheromata. J Clin Invest. 2007;117:195–205. 24. Tacke F, Alvarez D, Kaplan TJ, Jakubzick C, Spanbroek R, Llodra J, Garin A, Liu J, Mack M, van Rooijen N, Lira SA, Habenicht AJ, Randolph GJ. Monocyte subsets differentially employ CCR2, CCR5, and CX3CR1 to accumulate within atherosclerotic plaques. J Clin Invest. 2007;117:185–194. 25. Sunderkötter C, Nikolic T, Dillon MJ, Van Rooijen N, Stehling M, Drevets DA, Leenen PJ. Subpopulations of mouse blood monocytes differ in maturation stage and inflammatory response. J Immunol. 2004;172:4410–4417. 26. Varol C, Landsman L, Fogg DK, Greenshtein L, Gildor B, Margalit R, Kalchenko V, Geissmann F, Jung S. Monocytes give rise to mucosal, but not splenic, conventional dendritic cells. J Exp Med. 2007;204:171–180. 27. Yona S, Kim KW, Wolf Y, Mildner A, Varol D, Breker M, Strauss-Ayali D, Viukov S, Guilliams M, Misharin A, Hume DA, Perlman H, Malissen B, Zelzer E, Jung S. Fate mapping reveals origins and dynamics of monocytes and tissue macrophages under homeostasis. Immunity. 2013;38:79–91. 28. Hilgendorf I, Swirski FK. Making a difference: monocyte heterogeneity in cardiovascular disease. Curr Atheroscler Rep. 2012;14:450–459. 29. Cros J, Cagnard N, Woollard K, Patey N, Zhang SY, Senechal B, Puel A, Biswas SK, Moshous D, Picard C, Jais JP, D’Cruz D, Casanova JL, Trouillet C, Geissmann F. Human CD14dim monocytes patrol and sense nucleic acids and viruses via TLR7 and TLR8 receptors. Immunity. 2010;33:375–386. 30.Ingersoll MA, Spanbroek R, Lottaz C, Gautier EL, Frankenberger M, Hoffmann R, Lang R, Haniffa M, Collin M, Tacke F, Habenicht AJ, Ziegler-Heitbrock L, Randolph GJ. Comparison of gene expression profiles between human and mouse monocyte subsets. Blood. 2010;115:e10–e19. 31.Ziegler-Heitbrock L, Ancuta P, Crowe S, et al. Nomenclature of monocytes and dendritic cells in blood. Blood. 2010;116:e74–e80. 32.Mosser DM, Edwards JP. Exploring the full spectrum of macrophage activation. Nat Rev Immunol. 2008;8:958–969. 33.Sica A, Mantovani A. Macrophage plasticity and polarization: in vivo veritas. J Clin Invest. 2012;122:787–795. 34. Arnold L, Henry A, Poron F, Baba-Amer Y, van Rooijen N, Plonquet A, Gherardi RK, Chazaud B. Inflammatory monocytes recruited after skeletal muscle injury switch into antiinflammatory macrophages to support myogenesis. J Exp Med. 2007;204:1057–1069. 35.Egawa M, Mukai K, Yoshikawa S, Iki M, Mukaida N, Kawano Y, Minegishi Y, Karasuyama H. Inflammatory monocytes recruited to allergic skin acquire an anti-inflammatory M2 phenotype via basophil-derived interleukin-4. Immunity. 2013;38:570–580. 36.Ramachandran P, Pellicoro A, Vernon MA, et al. Differential Ly-6C expression identifies the recruited macrophage phenotype, which orchestrates the regression of murine liver fibrosis. Proc Natl Acad Sci USA. 2012;109:E3186–E3195. 37.Lee S, Vinegoni C, Feruglio PF, Fexon L, Gorbatov R, Pivoravov M, Sbarbati A, Nahrendorf M, Weissleder R. Real-time in vivo imaging of the beating mouse heart at microscopic resolution. Nat Commun. 2012;3:1054. 38. Jung K, Kim P, Leuschner F, Gorbatov R, Kim JK, Ueno T, Nahrendorf M, Yun SH. Endoscopic time-lapse imaging of immune cells in infarcted mouse hearts. Circ Res. 2013;112:891–899. 39.Frangogiannis NG. Regulation of the inflammatory response in cardiac repair. Circ Res. 2012;110:159–173. 1632 Circulation Research June 7, 2013 Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 40.Anzai A, Anzai T, Nagai S, et al. Regulatory role of dendritic cells in postinfarction healing and left ventricular remodeling. Circulation. 2012;125:1234–1245. 41. Dobaczewski M, Xia Y, Bujak M, Gonzalez-Quesada C, Frangogiannis NG. CCR5 signaling suppresses inflammation and reduces adverse remodeling of the infarcted heart, mediating recruitment of regulatory T cells. Am J Pathol. 2010;176:2177–2187. 42.Hofmann U, Beyersdorf N, Weirather J, Podolskaya A, Bauersachs J, Ertl G, Kerkau T, Frantz S. Activation of CD4+ T lymphocytes improves wound healing and survival after experimental myocardial infarction in mice. Circulation. 2012;125:1652–1663. 43. Frangogiannis NG, Lindsey ML, Michael LH, Youker KA, Bressler RB, Mendoza LH, Spengler RN, Smith CW, Entman ML. Resident cardiac mast cells degranulate and release preformed TNF-alpha, initiating the cytokine cascade in experimental canine myocardial ischemia/reperfusion. Circulation. 1998;98:699–710. 44.Ren G, Michael LH, Entman ML, Frangogiannis NG. Morphological characteristics of the microvasculature in healing myocardial infarcts. J Histochem Cytochem. 2002;50:71–79. 45.Iyer RP, Patterson NL, Fields GB, Lindsey ML. The history of matrix metalloproteinases: milestones, myths, and misperceptions. Am J Physiol Heart Circ Physiol. 2012;303:H919–H930. 46.Jourdan-Lesaux C, Zhang J, Lindsey ML. Extracellular matrix roles during cardiac repair. Life Sci. 2010;87:391–400. 47. Balsam LB, Wagers AJ, Christensen JL, Kofidis T, Weissman IL, Robbins RC. Haematopoietic stem cells adopt mature haematopoietic fates in ischaemic myocardium. Nature. 2004;428:668–673. 48. Dewald O, Zymek P, Winkelmann K, Koerting A, Ren G, Abou-Khamis T, Michael LH, Rollins BJ, Entman ML, Frangogiannis NG. CCL2/ monocyte chemoattractant protein-1 regulates inflammatory responses critical to healing myocardial infarcts. Circ Res. 2005;96:881–889. 49. Tsujioka H, Imanishi T, Ikejima H, et al. Impact of heterogeneity of human peripheral blood monocyte subsets on myocardial salvage in patients with primary acute myocardial infarction. J Am Coll Cardiol. 2009;54:130–138. 50. Troidl C, Möllmann H, Nef H, Masseli F, Voss S, Szardien S, Willmer M, Rolf A, Rixe J, Troidl K, Kostin S, Hamm C, Elsässer A. Classically and alternatively activated macrophages contribute to tissue remodelling after myocardial infarction. J Cell Mol Med. 2009;13:3485–3496. 51.Ehninger A, Trumpp A. The bone marrow stem cell niche grows up: mesenchymal stem cells and macrophages move in. J Exp Med. 2011;208:421–428. 52. Lo Celso C, Scadden DT. The haematopoietic stem cell niche at a glance. J Cell Sci. 2011;124:3529–3535. 53. Chow A, Huggins M, Ahmed J, Hashimoto D, Lucas D, Kunisaki Y, Pinho S, Leboeuf M, Noizat C, van Rooijen N, Tanaka M, Zhao ZJ, Bergman A, Merad M, Frenette PS. CD169(+) macrophages provide a niche promoting erythropoiesis under homeostasis and stress. Nat Med. 2013;19:429–436. 54.Leuschner F, Panizzi P, Chico-Calero I, et al. Angiotensin-converting enzyme inhibition prevents the release of monocytes from their splenic reservoir in mice with myocardial infarction. Circ Res. 2010;107:1364–1373. 55. Dutta P, Courties G, Wei Y, et al. Myocardial infarction accelerates atherosclerosis. Nature. 2012;487:325–329. 56.Assmus B, Iwasaki M, Schächinger V, Roexe T, Koyanagi M, Iekushi K, Xu Q, Tonn T, Seifried E, Liebner S, Kranert WT, Grünwald F, Dimmeler S, Zeiher AM. Acute myocardial infarction activates progenitor cells and increases Wnt signalling in the bone marrow. Eur Heart J. 2012;33:1911–1919. 57. Massa M, Rosti V, Ferrario M, Campanelli R, Ramajoli I, Rosso R, De Ferrari GM, Ferlini M, Goffredo L, Bertoletti A, Klersy C, Pecci A, Moratti R, Tavazzi L. Increased circulating hematopoietic and endothelial progenitor cells in the early phase of acute myocardial infarction. Blood. 2005;105:199–206. 58. Auffray C, Fogg D, Garfa M, Elain G, Join-Lambert O, Kayal S, Sarnacki S, Cumano A, Lauvau G, Geissmann F. Monitoring of blood vessels and tissues by a population of monocytes with patrolling behavior. Science. 2007;317:666–670. 59. Oka T, Hikoso S, Yamaguchi O, Taneike M, Takeda T, Tamai T, Oyabu J, Murakawa T, Nakayama H, Nishida K, Akira S, Yamamoto A, Komuro I, Otsu K. Mitochondrial DNA that escapes from autophagy causes inflammation and heart failure. Nature. 2012;485:251–255. 60. Jankowski M, Wang D, Danalache B, Gangal M, Gutkowska J. Cardiac oxytocin receptor blockade stimulates adverse cardiac remodeling in ovariectomized spontaneously hypertensive rats. Am J Physiol Heart Circ Physiol. 2010;299:H265–H274. 61. Lee WW, Marinelli B, van der Laan AM, et al. PET/MRI of inflammation in myocardial infarction. J Am Coll Cardiol. 2012;59:153–163. 62.Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008;454:428–435. 63. Gordon S, Taylor PR. Monocyte and macrophage heterogeneity. Nat Rev Immunol. 2005;5:953–964. 64. Ley K, Miller YI, Hedrick CC. Monocyte and macrophage dynamics during atherogenesis. Arterioscler Thromb Vasc Biol. 2011;31:1506–1516. 65. Libby P. Inflammation in atherosclerosis. Nature. 2002;420:868–874. 66. Kinne RW, Bräuer R, Stuhlmüller B, Palombo-Kinne E, Burmester GR. Macrophages in rheumatoid arthritis. Arthritis Res. 2000;2:189–202. 67. Szekanecz Z, Koch AE. Macrophages and their products in rheumatoid arthritis. Curr Opin Rheumatol. 2007;19:289–295. 68. Duffield JS, Forbes SJ, Constandinou CM, Clay S, Partolina M, Vuthoori S, Wu S, Lang R, Iredale JP. Selective depletion of macrophages reveals distinct, opposing roles during liver injury and repair. J Clin Invest. 2005;115:56–65. 69. Schulze PC, Biolo A, Gopal D, Shahzad K, Balog J, Fish M, Siwik D, Colucci WS. Dynamics in insulin resistance and plasma levels of adipokines in patients with acute decompensated and chronic stable heart failure. J Card Fail. 2011;17:1004–1011. 70. Dixon DL, Griggs KM, Bersten AD, De Pasquale CG. Systemic inflammation and cell activation reflects morbidity in chronic heart failure. Cytokine. 2011;56:593–599. 71. Maekawa Y, Anzai T, Yoshikawa T, Asakura Y, Takahashi T, Ishikawa S, Mitamura H, Ogawa S. Prognostic significance of peripheral monocytosis after reperfused acute myocardial infarction:a possible role for left ventricular remodeling. J Am Coll Cardiol. 2002;39:241–246. 72. Engström G, Melander O, Hedblad B. Leukocyte count and incidence of hospitalizations due to heart failure. Circ Heart Fail. 2009;2:217–222. 73. Yvan-Charvet L, Pagler T, Gautier EL, Avagyan S, Siry RL, Han S, Welch CL, Wang N, Randolph GJ, Snoeck HW, Tall AR. ATP-binding cassette transporters and HDL suppress hematopoietic stem cell proliferation. Science. 2010;328:1689–1693. 74.Murphy AJ, Akhtari M, Tolani S, Pagler T, Bijl N, Kuo CL, Wang M, Sanson M, Abramowicz S, Welch C, Bochem AE, Kuivenhoven JA, YvanCharvet L, Tall AR. ApoE regulates hematopoietic stem cell proliferation, monocytosis, and monocyte accumulation in atherosclerotic lesions in mice. J Clin Invest. 2011;121:4138–4149. 75. Panizzi P, Swirski FK, Figueiredo JL, Waterman P, Sosnovik DE, Aikawa E, Libby P, Pittet M, Weissleder R, Nahrendorf M. Impaired infarct healing in atherosclerotic mice with Ly-6C(hi) monocytosis. J Am Coll Cardiol. 2010;55:1629–1638. 76.Goldstein JA, Demetriou D, Grines CL, Pica M, Shoukfeh M, O’Neill WW. Multiple complex coronary plaques in patients with acute myocardial infarction. N Engl J Med. 2000;343:915–922. 77. Milonas C, Jernberg T, Lindbäck J, Agewall S, Wallentin L, Stenestrand U; RIKS-HIA Group. Effect of Angiotensin-converting enzyme inhibition on one-year mortality and frequency of repeat acute myocardial infarction in patients with acute myocardial infarction. Am J Cardiol. 2010;105:1229–1234. 78. Wright AP, Öhman MK, Hayasaki T, Luo W, Russo HM, Guo C, Eitzman DT. Atherosclerosis and leukocyte-endothelial adhesive interactions are increased following acute myocardial infarction in apolipoprotein E deficient mice. Atherosclerosis. 2010;212:414–417. 79. Monis B, T. Aminopeptidase activity in myocardial infarction of man. a histochemical study. Am J Pathol. 1964;44:867–876. 80.Sosnovik DE, Nahrendorf M, Deliolanis N, Novikov M, Aikawa E, Josephson L, Rosenzweig A, Weissleder R, Ntziachristos V. Fluorescence tomography and magnetic resonance imaging of myocardial macrophage infiltration in infarcted myocardium in vivo. Circulation. 2007;115:1384–1391. 81.Nahrendorf M, Sosnovik DE, Waterman P, Swirski FK, Pande AN, Aikawa E, Figueiredo JL, Pittet MJ, Weissleder R. Dual channel optical tomographic imaging of leukocyte recruitment and protease activity in the healing myocardial infarct. Circ Res. 2007;100:1218–1225. 82.Majmudar MD, Keliher EJ, Heidt T, et al. Monocyte-directed RNAi targeting CCR2 improves infarct healing in atherosclerosis-prone mice. Circulation. 2013;127:2038–2046. 83. Majmudar MD, Yoo J, Keliher EJ, Truelove JJ, Iwamoto Y, Sena B, Dutta P, Borodovsky A, Fitzgerald K, Di Carli MF, Libby P, Anderson DG, Swirski FK, Weissleder R, Nahrendorf M. Polymeric nanoparticle PET/ MR imaging allows macrophage detection in atherosclerotic plaques. Circ Res. 2013;112:755–761. Nahrendorf and Swirski Cardiac Macrophages 1633 Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 84. Naresh NK, Xu Y, Klibanov AL, Vandsburger MH, Meyer CH, Leor J, Kramer CM, French BA, Epstein FH. Monocyte and/or macrophage infiltration of heart after myocardial infarction: MR imaging by using T1-shortening liposomes. Radiology. 2012;264:428–435. 85. Flögel U, Ding Z, Hardung H, Jander S, Reichmann G, Jacoby C, Schubert R, Schrader J. In vivo monitoring of inflammation after cardiac and cerebral ischemia by fluorine magnetic resonance imaging. Circulation. 2008;118:140–148. 86. Alam SR, Shah AS, Richards J, Lang NN, Barnes G, Joshi N, MacGillivray T, McKillop G, Mirsadraee S, Payne J, Fox KA, Henriksen P, Newby DE, Semple SI. Ultrasmall superparamagnetic particles of iron oxide in patients with acute myocardial infarction: early clinical experience. Circ Cardiovasc Imaging. 2012;5:559–565. 87.Yilmaz A, Dengler MA, van der Kuip H, Yildiz H, Rösch S, Klumpp S, Klingel K, Kandolf R, Helluy X, Hiller KH, Jakob PM, Sechtem U. Imaging of myocardial infarction using ultrasmall superparamagnetic iron oxide nanoparticles: a human study using a multi-parametric cardiovascular magnetic resonance imaging approach. Eur Heart J. 2013;34:462–475. 88.Heine GH, Ulrich C, Seibert E, Seiler S, Marell J, Reichart B, Krause M, Schlitt A, Köhler H, Girndt M. CD14(++)CD16+ monocytes but not total monocyte numbers predict cardiovascular events in dialysis patients. Kidney Int. 2008;73:622–629. 89.Rogacev KS, Seiler S, Zawada AM, Reichart B, Herath E, Roth D, Ulrich C, Fliser D, Heine GH. CD14++CD16+ monocytes and cardiovascular outcome in patients with chronic kidney disease. Eur Heart J. 2011;32:84–92. 90.Rogacev KS, Cremers B, Zawada AM, et al. CD14++CD16+ monocytes independently predict cardiovascular events: a cohort study of 951 patients referred for elective coronary angiography. J Am Coll Cardiol. 2012;60:1512–1520. 91.Berg KE, Ljungcrantz I, Andersson L, Bryngelsson C, Hedblad B, Fredrikson GN, Nilsson J, Björkbacka H. Elevated CD14++CD16monocytes predict cardiovascular events. Circ Cardiovasc Genet. 2012;5:122–131. 92.Ridker PM. Testing the inflammatory hypothesis of atherothrombosis: scientific rationale for the cardiovascular inflammation reduction trial (CIRT). J Thromb Haemost. 2009;7 (Suppl 1):332–339. 93. Ridker PM, Thuren T, Zalewski A, Libby P. Interleukin-1β inhibition and the prevention of recurrent cardiovascular events: rationale and design of the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS). Am Heart J. 2011;162:597–605. 94.Leuschner F, Dutta P, Gorbatov R, et al. Therapeutic siRNA silencing in inflammatory monocytes in mice. Nat Biotechnol. 2011;29:1005–1010. 95.Majmudar MD, Nahrendorf M. Cardiovascular molecular imaging: the road ahead. J Nucl Med. 2012;53:673–676. Monocyte and Macrophage Heterogeneity in the Heart Matthias Nahrendorf and Filip K. Swirski Downloaded from http://circres.ahajournals.org/ by guest on June 17, 2017 Circ Res. 2013;112:1624-1633 doi: 10.1161/CIRCRESAHA.113.300890 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2013 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/112/12/1624 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/