Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
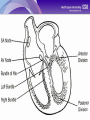
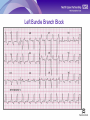
How to Find Your Way Around 1. You can play the PowerPoint, and find the Test here How to Find Your Way Around 2. You can minimise this column and make the main page bigger by clicking this icon. Click it again to bring it back. How to Find Your Way Around 3. Always click this ‘Home’ icon to save your progress and log off. This is very important! 22nd April 2009 ECG Recording and Basic Interpretation Introduction to the E.C.G. E.C.G is Electrocardiograph or electrocardiogram It can provide evidence to support a diagnosis, but remember…..LOOK AT THE PATIENT NOT JUST THE PAPER Is essential in the diagnosis of chest pain and abnormal heart rhythms Is helpful in diagnosing breathlessness The Electricity of the Heart Any muscle contraction causes an electrical change – depolarisation These changes can be detected by electrodes on the surface of the body To ensure recording of only cardiac electrical activity, the patient must be relaxed Although a four chamber organ, for E.C.G purposes, the heart can be thought of as two, as the atria and ventricles contract together The Electrical Pathway of the Heart Each electrical discharge starts in the sino-atrial node, located in the right atrium Then spreads through the atrial muscle fibres There is a delay while depolarisation spreads through the atrio-ventricular node Then along single carriageway Bundle of His along to parallel carriageways of the Right and Left Bundle Branches Left Bundle Branch carriageway divides into two and conduction spreads through specialised Purkinje fibres Normal heart rate is called sinus rhythm and implies that the electrical activity has commenced in the SA node The Shape of the ECG Atrial muscle mass is smaller compared with the ventricles – so the is the electrical charge Atrial contraction is the P wave Ventricular muscle mass is larger and creates a bigger deflection on the ECG This is represented by the QRS complex T wave represents repolarisation – the ventricular muscle mass returning to a resting state P,Q,R & S are waves, Q,R & S make up a complex, interval between S and T is called the ST segment ECG Recording ECG machines record electrical activity on moving paper – the speed and the squared paper is standardised Each large (5mm) square represents 0.2 sec, so 5 large squares per second 1 QRS per 5 squares means a pulse of 60 beats per minute PR interval should be 3 – 5 small squares QRS is usually 3 small squares – any abnormally long conduction shows as a widened QRS complex Recording an ECG 12 lead means 12 different “electrical pictures”; does not refer to wires that connect patient to machine Good skin contact is essential (chest shaving may be required) One electrode on each limb, and one that is positioned in 6 different places on the chest (or has 6 “terminals”) Electrodes labelled Left Arm, Right Arm, Left Leg and Right Leg, plus chest 1 to 6 Electrode Placement Lead V1 is placed over the 4th intercostal space, to the right of the sternum Lead V2 is placed over the 4th intercostal space, to the left of the sternum Lead V4 is placed over the 5th intercostal space in the midclavicular line Lead V3 is placed midway between V2 and V4 Lead V5 is placed on the same horizontal level as V4 but at the anterior axilliary line Lead V6 is placed on the same horizontal level as V4 and V5 but on the mid axilliary line The Shape of the QRS Complex Normal hearts have more muscle in left ventricle compared to right QRS complex represents ventricular activity and is normally the largest deflection Information can be gathered from looking at rhythm strips Layout of the ECG 12 views are represented and the segments are labelled I,II, III, aVR, aVL, and aVF. Most machines display each view horizontally, and vertically across the page A rhythm strip is included at the end to enable the reader to determine rate and regularity of heart rhythm Normal ECG A normal ECG will contain regular complexes Each complex will be made up of a P wave, swiftly followed by a QRS The QRS should be pointed The complexes should be of uniform appearance Normal ECG Abnormal ECG Abnormal ECG Left Bundle Branch Block Acute ST Depression Acute ST Elevation Inferior MI Acute ST Elevation Posterior MI Atrial Flutter Atrial Fibrillation Ventricular Fibrillation You Have Now Finished the Learning Please click the ‘Test’ icon in the left column. You may need to maximise the column by clicking the top left icon. Remember to click the ‘Home’ icon when you finish the Test to save your results