Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Signal transduction wikipedia , lookup
Endogenous retrovirus wikipedia , lookup
Biosynthesis wikipedia , lookup
Gene therapy wikipedia , lookup
Gene regulatory network wikipedia , lookup
Biochemistry wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Silencer (genetics) wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Real-time polymerase chain reaction wikipedia , lookup
Community fingerprinting wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
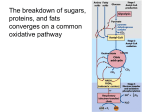
From www.bloodjournal.org by guest on June 17, 2017. For personal use only. Molecular Abnormality of Erythrocyte Pyruvate Kinase Deficiency in the Amish By Hitoshi Kanno, Sarnir K. Ballas, Shiro Miwa, Hisaichi Fujii, and Herbert S.Bowman We describe the cellular and molecular biologic studies of the erythrocyte pyruvate kinase (PK) deficiency of the Amish deme in Pennsylvania. Nucleotide sequencing of the patient's PK gene showed a point mutation, CGC to CAC, corresponding to no. 1436 from the translationafinitiatkn site of the R-type PK (R-PK) mRNA, and it caused a single amino acid substitution from Arg to His at the 479th amino acid residue of the R-PK. The substitutedArg residue is located in the C domainof PK subunit, that is essentialfor both the intersubunit contact and the allosteric regulation. Because this enzyme showsthe catalytic activity onlyas a dimer or tetramer, it is rational that the structural alteration would result in severePK deficiency. To elucidatethe effect of the PK deficiency on red blood cell (RBC) membrane, we performed the cellular studies of the patients' RBCs. Ouabaininsensitive K+ efflux was increased to 142% to 145% of normal controls andnot inhibaed byfurosemide, as previously observed in HbSC disease RBCs. 0 1994 by The Americen Sochty of Hematology. P family (Fig 1).STY,Sr, is a distant consanguineous relativeof SJY and AB who are believed to be the ancestral pair oftheMifflin CountyPennsylvaniaAmish red blood cell (RBC)PK-deficient gene." Family history showedJY to be one of 10 Old Order Amish siblings of the STY, Sr, pedigree. Two sisters hadbeenaffected with the Amish RBC PK-deficient hemolysis, one of whom died. A subsequent sister born later, AY, likewise was found to have this RBC disorder. JY was initially seen at age 1 month, having been icteric at 48 hours of life with deepeningjaundice during the subsequent5 days. As the icterus gradually faded, he evidenced increasing pallor and was referred to the Hematology Center, Harrisburg Hospital.He was transfused with packed RBCs sufficient to maintain the hematocrit at 26%, and such transfusions were maintained every eighth week. Thepretransfusionhematologic values were:RBCs,1.56 X lo6/ pL, hemoglobin (Hb), 5.1 g/dL, hematocrit (Hct), 18.5%, mean cell volume (MCV), 112 fL, reticulocytes, 15.4%. Blood film showed 58 nucleated RBCsIlOO white blood cells (WBCs), macrocytosis, polychromia, and marked anisocytosis. Total bilirubin was 2.6 mg/ dL, andlactate dehydrogenase (LDH) 1.250U.RBC PK activity was 0.1 U/lO'" RBCs. At 6 months of age, his spleen became palpable5 cm below the left costal margin. Transfusion therapy was continued until 17 months of age, when splenectomy was performed. Splenic red pulp preparations showed reticuloendothelial cell, RBCs,and reticulocyte phagocytosis and increased reticulocytes." Subsequent examinations have shown normal findings and no transfusion have beenrequired.Currentexaminationsatage 31 yearshaveshown YRUVATE KINASE (PK) deficiency is the most common hereditary nonspherocytic hemolytic anemia caused by a glycolytic enzyme defect. The residual erythrocyte PK activity is not usually related tothe severity of anemia, whereas the enzymatic characteristics such as a decreased substrate affinity, thermal instability, or impaired response to the allosteric activator correspond well to the phenotype.' We have analyzed the R-PK cDNA of six Japanese PK-deficient families, including five true homozygotes andacompoundheterozygote,andidentifiedfourdistinct missense mutation^.^^ Another group found point mutations in the Turkish and Lebanese PK-deficient individuals: and one mutation found in the Lebanese was identical with the mutation identified intwo Japanese families? It was noteworthy that these mutations may cause the structural changes near the potassium-binding sites'; consequently, the variant PKs showed low affinity with the substrate, phosphoenolpyruvate (PEP). We have also shown that the variant PK synthesized in Escherichia coli had a thermal instability? Although the reticulocyte mRNA is the appropriate source for cloning and sequencing the R-PK cDNA, the genomic DNA is more convenient for handling. Recently,we have clarified thestructure of the humanGtype PK (GPK) gene, and it becomes possible to search the mutation in the genomic DNA analysis.' In 1963, five PK-deficient kindred found in the Mifflin County Amish deme in Pennsylvania were reported? Previous studies showed that all the Amish PK variants descended from a common ancestor, and consanguineous marriage was often noted in the family." Therefore, the PK-deficient subjects in the population are homozygous with an identical mutation. The clinical manifestation of the Amish PK variant was reported to be severe, and sometimes death occurred in the neonatal or infantile period unless splenectomy was performed.' To clarify the molecular abnormality of the Amish PK variant might be useful not only for the understanding of the relationship between the structure and the function of PK but also for the screening of the variant gene in the population. In this report, we present the molecular abnormality identified in an Amish family, and discuss the structure-function relationship of PK and the cellular characteristics of PK-deficient erythrocytes. MATERIALS AND METHODS Clinical features of the Amish PK-deficient subjects. AY and JY are siblings, being brother and sister and members of the STY,Sr, Blood, Vol 83, No 8 (April 15). 1994: pp 2311-2316 From the Okinaka Memorial Institute for Medical Research; the Department of Blood Transfusion Medicine, the Tokyo Women's Medical College, Tokyo, Japan; the Cardeza Foundationfor Hematologic Research, Jefferson Medical College, Philadelphia; and the Harrisburg Hospital, Harrisburg, PA. Submitted June 18, 1993; accepted December 8,1993. Supported in part by a Scientific Research Grant from the Ministry of Education, Science, and Culture, and by a Research Grant for Specific Diseases from the Ministry of Health and Welfare, Japan, andin part by the National Institutes of Health Comprehensive Sickle Cell Grant No. HL 38632. Address reprint requests to Hitoshi Kanno, MD, Okinaka Memorial Institute for Medical Research, 2-2-2 Toranomon, Minato-h, Tokyo 105, Japan. The publication costs of this article weredefrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 8 1994 by The American Society of Hematology. O006-497I/94/8308-00I9$3.00/0 2311 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 2312 1.22 KANNO ET AL 2.46 DIED 2.64 1.04 0.17 3.3 AY 0.1 3.75 1.35 0.46 JY Fig 1. The pedigree of the Amish PK-deficient family. Number indicates erythrocyte PK activity, units per 10'' RBCs. RBCs 2.55 X 106/pL, Hb 10 g/dL, Hct 29.6%, MCV 116 fL, and reticulocytes 26%. In the blood film, macrocytes, polychromasia, and echinocyte were noted. LDH was 278 U. Materials. Blood samples from the probands were obtained under informed consent. High molecular weight genomic DNAs were purified by the standard protocol." Restriction endonucleases and modifying enzymes were purchased from Takara Shuzo (Kyoto, Japan) and New England Biolabs (Beverly, MA). Taq DNA polymerase (AmpliTaq) was obtained from Perkin Elmer Cetus (Norwalk, CT). DNA was sequenced using a DNA sequencing system (Model 373A; Applied Biosystems, Foster City, CA). The computer software, DNASIS (Hitachi Software Engineering, Yokohama, Japan), was used toanalyze the hydrophobicity properties of the variant protein based on the theory of Hopp and Woods." Hematologic data and cellular studies about PK-deficientRBCs. Routine hematologic methods were used to determine the Hb level, Hct, RBC indices, and reticulocyte count. Whole RBC deformability and RBC sodium (Na+) and potassium (K') concentrations were determined as previously de~cribed.'~ The ouabain-insensitive component of K+-efflux was measured as described previo~sly.'~ Amplification and sequencing of the humanL-PK gene. Oligonucleotides used for the amplification of the exons of human L-PK gene are listed inthe Table 1. L1 (S-CCCGGGAGGCAGAGGCCGCAGT-3') and L2 (5'-CAAAAGCTCCATCTGGACATT-3') were used for amplifying the 3' end sequences of exon 10. Polymerase chain reaction (PCR) was performed in a total volume of 100 pL containing 1 pg of the template DNA, deoxynucleotides at 200 mmol/L each, a pair of primers, 10 mmoVL Tris/HC1 @H 8.3), 50 mmol/L KCl, 1.5 to 3 mmol/L MgCI2, 0.001% gelatin, and 5 U of Taq DNA polymerase. The amplified DNA fragments were subcloned into pBluescript (Stratagene, La Jolla, CA) by the restriction sites within the DNA or primers. Exons 1, 3 through 12, and the adjacent intron sequences were sequenced by the dideoxy chain termination method with fluorescent primers. RESULTS Cellular studies of the PK-deficient RBCs. Hematologic characteristics of the subjects studied and the rheologic prop- erties of PK-deficient RBCs are listed in Table 2. Because both JY and AY had been splenectomized, the anemia was not severe on the examination. The MCV in PK deficiency was increased, and it seemed to be reflectedon the high reticulocyte counts, which were usually observed in PK deficiency after splenectomy. It should be noted that the PKdeficient RBCs showed increased maximum deformability as well as increased deformability at isotonic conditions. To elucidate further the hydration status and surface areato-volume ratio of PK-deficient RBCs,we measured the density distribution and cation content of these cells (Fig 2, Table 3). There is a significant shift to lower density in PKdeficient RBC populations as seen in Fig 2. Table 3 shows that the sodium content of PK-deficient cells is similar to that of controls, whereas the potassium and total cation contents are significantly increased to 117% to 121% of normal controls. To investigate the nature of the abnormal cation regulation in PK-deficient RBCs further, we determined the ouabaininsensitive K' efflux in the presence or absence of 1.0 mmol/ L furosemide, an inhibitor of Cl- transport and chloridedependent K+ flux. Table 4 shows that PK-deficient cells had a markedly increased K+ efflux. The first-order rate constant for K' efflux of the PK-deficient cells was 0.034 to 0.035 h-', compared with 0.024 for control cells (142% to 145% increase). The addition of furosemide reduced the rate constant for K+ efflux of normal cells, but did not decrease that of the PK-deficient cells. Identification of a point mutation in the L-PK gene of the Amish PK variant. Sequencing of the L-PK gene from the Amish PK variant showed that the variant had a single nucleotide change at the 3'-end nucleotide of exon 10 of human L-PK gene, corresponding tono. 1436 of humanR-PK cDNA, 1436 CGC -+ CAC. This missense mutation caused a single aminoacid substitution; 479 Arg His (R479H), which subsequently decreased the hydrophobicity properties near the mutated site (Fig 3). The predicted secondary structure by the theory of Chou and Fasman showed that the core of a-helix might be formed by this amino acid change (data not shown). This Arg residue is well conserved during evolution, including chicken M1-, cat M1-,ratR-, and human M2-type PK (Fig 4).16-19 Demonstration of the point mutation by the Hpa II digestion of the genomic PCR products. To confirm this nucleotide change in genomic DNAs of the probands, the 3' end -+ Table 1. Oligonucleotidesfor PCR of Genomic PK Exon I 111 IV-v VI VII-VIII IX-x XI XI I Sense Primer 5'-CTAAAGClTCTGTGGGGACAGGGTGGC-3' 5'-GTGACATGCAGTCCCTGAGCICCC-3' 5'-GGCGlTCTGAGAAFsGTAATGG-3' 5"GACTCCGGAGCTCAGAACTCA-3' 5"CTGACCGCAGCTGGCTCl"rCATG-3' 5"GGTGTCAGAGAGGTAsClTGGGC-3' 5'-LAAlTCACCACl"rClTGC-3' 5'-CCACAGCTGTCCAATGAllTG-3' Antisense Primer 5"GAGGCTCTGAAGAACGTACG-3' 5"ATACCAATAGGCCTGTGTGGCT-3' 5"TCCAClTCCGACTCTGGACC-3' 5"CAGCGCACGGATGTGATCAGG-3' 5"CCCTGCAGTGTGGGTAlTCACCCA-3' 5"CAAAGGATCCATCTGGACAlTCC-3' 5'-CTCCGGATsCAAATGGTAGGAG-3' 5"AAGGCATCTTAGGGCCTGChGAGC-3' Product (bp) 374 260 559 Sac 272 626 531 281 450 Restriction Sites HindlllISty l Sac IIPst l €CO RIIApa I IIBcl l Pvu IIIPst I Kpn IIBamHI €coRIIBamHI Pvu IIIfSt I The primers used in sequencing the entire coding region for the R-type PK are shown. To create appropriate restriction sites, the underlined nucleotides are added or substituted to the primers. From www.bloodjournal.org by guest on June 17, 2017. For personal use only. PYRUVATE KINASE DEFICIENCY IN THE AMISH 2313 Table 2. Hematologic and Rheologic Data on the Patients Studied Max Dl Age/ Sex Hb (g/dL) Het MCV Reticulocytes (%) (fL) (X) 29F 31/M 11.0 9.3 37.3 27.3 116.1 115.8 18.5 25.4 Patient AY JY % of Normal 111 120 112 120 Maximum deformability index (Max Dl) was attained by osmotic gradient ektacytometry. Dl 290 is the deformability index of RBCs suspended in a buffer the osmolarity of which is 290 mOsmkg. region of exon 10 was amplified by PCR and examined the Hpa I1 cleavage site, that should be abolished by the nucleotide change. A 201-bp fragment flanking the 3' end of exon 10 was amplified by PCR. When the Hpa I1 site is intact, theband becomes four fragments, 132, 39, 28,and 2 bp, r a w I . -!P=+ , Table 3. Cation Content of PK-Deficient RBCs Dl 290 ? i Patient Control P Variable AY JY n=3 Value Na', mEq/L RBCs K', mEq/L RBCs Na* + K-, mEq/L RBCs 13.6 99.5 113.1 11.9 102.0 113.9 11.9 z 3.30 84.6 2 2.04 96.4 2 1.39 >.05 c.025 c.005 after Hpa I1 digestion. As shown in Fig 5, one of the Hpa I1 sites was abolished in the PCR products of the probands, meaning the homozygous mutation in the probands' L-PK gene. DISCUSSION Here we report a molecular abnormality in the Amish PK deficiency. The probands had suffered from severe hemolytic anemia, and required transfusion every 8 weeks. After splenectomy the anemia was compensated, with a Hb level of about 9 to 10 g/dL. Cellular studies of the PK-deficient RBCs showed increased K' content and a markedly expanded ouabain-insensitive K' efflux. The pathophysiology of PK-deficient erythrocytes has been Keitt'" has shown that PK-deficient erythrocytes were almost entirely dependent on mitochondrial oxidative phosphorylation rather than on glycolysis to maintain adenosine triphosphate (ATP) levels. A rapid decrease of ATP levels because of decreased oxidative phosphorylation during maturation of erythrocytes allows massive losses of potassium and water, resulting in the formation of spiculated erythrocytes, ie, echinocytes. These cells usually have decreased deformability, and are easily sequestered by the reticuloendothelial system." Splenectomy may prevent reticulocytes and young erythrocytes from being trapped by the reticuloendothelial system, resulting in improvement of the anemia in most cases. The hematologic data of the Amish PK deficiency showed postsplenectomy reticulocytosis, which was usually observed in PK deficiency, and the large, lower density cells with increased deformability may reflect mainly the increased number of reticulocytes. Despite the increased K' content, these cells are prone to lose K' andwaterrapidly because of impaired ATP availability, and become dehydrated and en- Table 4. Effect of Furosemide on Ouabain-Insensitive K' Efflux of Normal and PK-Deficient RBCs - 3 In K- ConcentrationlmL RECs ~~ PK-Deficient RECs Normal -. C AY JY Fig 2. The actual density profile of PK-defificientRBC (Ay and JY) and a normal control (C). Additive RECs AY JY None 1.0 mmol/L furosemide 0.024 0.014 0.034 0.037 0.035 0.037 Cells were incubated for 2 hours at 37°C in 10 mmol/L HEPES (pH 7.5). 5 mmol/L glucose, 0.2 mmol/L ouabain, and NaCl to bring the final osmolarity to 290 mOsm/kg, in the presence or absence of the indicated additive. Values shown are the negative In of the calculated intracellular K+ concentration as a function of time. From www.bloodjournal.org by guest on June 17, 2017. For personal use only. KANNO ET AL 2314 5 1 I 1 0 -1 -2 -3 -4 -5 Arg-His -q p"----d ..................................................... l' 471 ................................................................. I 48 1 ity were unfavorable characteristics of this variant, which may be responsible for the phenotype. There are four mammalian PK isozymes23:type-M1, M2, L, and R. The M-type PK (M-PK) gene encodes both M1 andM2 isozyme^.^^^^^ In contrast, L and R isozymes are encoded by the L-PK gene.8." Both the M- and L-PK gene of rats and humans have 12 exons.8,18,25,26 Alternative splicing produces two distinct mRNAs, which contain either exon 9 (Ml) or 10 (M2) of the M-PK gene. Exons 1 and 2 of the L-PK gene are specifically transcribed to the R- and L-PK mRNA by the tissue-specific promoter. It is of interest that among four isoenzymes only M1-type is not allosterically regulated." Because M1 and M2 isozymes differ only in the exon 9-10 region, exon 10 should encode the amino acid residues responsible for the allosteric property. Comparison of exon 10 between the M- and L-PK gene disclosed that there was an extensive homology, indicating that the exon 10-encoding region of L-PK gene also contained the allosteric structure (Fig 4). It seemed to be rational that the variant showed lower response to the allosteric effector, because the missense mutation identifiedin exon 10 would cause the drastic change of hydrophobicity and secondary structure. The amino acid substitution (R479H) resides in the third ahelix of the C domain of PK subunit, deduced from the tertiary structure of cat muscle PK." The C domain is considered to be important for the intersubunit contact as well as the allosteric regulation. Because PK has kinetic activity only as either dimer or tetramer, the structural change may interfere with tetramer formation, resulting in a drastic loss of activity. The identification of the molecular lesion of erythrocyte County Pennsylvania Amish PK deficiency in the Mienables us to detect the mutation by a simple procedure, PCR and restriction endonuclease digestion. Thus, it can be applied to genetic counseling or the prenatal diagnosis of the Amish PK-deficient hemolytic anemia, which has been known as a most severe form of PK deficiency. As only the Geauga County Ohio Amish are related to the MiWin County Pennsylvania Amish deme by an ancestral genetic member B ) : 'no other demes of Amish within the United States (ie, A are believed to exist sharing this missense mutation or the erythrocyte PK deficiency hemolytic anemia. I 490 Fig 3. Hydrophobicity profiles neer the mutated site. The dolted line indicatesthe hydrophobicity propertiesof normel R-PK from no. 471 to no. 490 amino acid noidues, and the solid line s h o w the altered hydrophobicprop.rtkr of the Amish PK variant. The arrows show the position of the 479th emino acid residue, whkh is substituted from Arg to His, and the shift of the hydrophobicity profile caused bythe amino acid substitution. trapped in the splenic environment. This hypothesis is supported by the finding of entrapped reticulocytes in the splenic red pulp of the patient's spleen." It should be noted that the potassium efflux of the Amish PK-deficient erythrocytes was increased up to 142% to 145% of normal controls. Activation of Na+-independent K+/Cl- cotransport seemed unlikely in PK deficiency, because the addition of 1.0 mmol/L furosemide (an inhibitor of KC1 cotransport) to the medium did not reduce the rate constant of K+ efflux. The K+ efflux may be increased by a mechanism similar tothat observed in Hbsc RBcs.ls The reported enzymatic characteristics" of the identical variant PK were a low Michaelis constant (Km) for PEP, low Km for adenosine diphosphate, narrow nucleotide specificity, less ATP inhibition than normal, more fructose-l, 6diphosphate (FDP) required for 50% activation, thermal instability, normal optimum pH, and normal migration in polyacrylamide gel electrophoresis. It should be noted that lower response to the allosteric effector, FDP, and thermal instabil- Fig4. The comparison of the aminoacid sequence of the C domain of PK, encoded by exon 9 (Ml)or 10 ( M 2 ,R). Open boxes surrounded by solid lines indicate amino acid residues, which are conserved in all species examined. Boxes with dotted lines showthe amino acids, which are only found in the allosterkdy r e g M isozymes, M2 and R (L). The arrow polnb the Arg residue, which is substituted to His in the Amish PK variant. The numbers indicate the amino acid comrponding to the Arg residues. From www.bloodjournal.org by guest on June 17, 2017. For personal use only. PYRUVATEKINASEDEFICIENCY M 1 2 IN THE AMISH 2315 3 - bp 171 132 39 28 Fig 5. Hpa II digestion of the PCR productsflanking the 3' end of exon 10 from the probands and a normal control. Becausethere are three Hpa II recognitionsites in the amplified DNA, the PCR product of normal control is digested into four fragments: 132, 39, 28, and 2 bp. When the 1436 G to A mutation is present, the 201-bp products are digested into three fragments:171,28, and 2bp. M, pBR322 digested with Msp I; 1, normal control; 2, the AmishPK-deficient subject JV; 3, the Amish PK-deficient subject AV. ACKNOWLEDGMENT WC are indebted to Y. Okamura, A. Kawaguchi, and M. Watanabe for their technical assistance. REFERENCES KR, Paglia DE:Pyruvatekinaseand other cnzyme deficiency disorders ofthe erythrocyte, in Scriver CR, Bcaudet AL. Sly WS. Valle D (cds): The Metabolic Basis of Inherited Disease (ed 6 ) . New York, NY, McGraw-Hill, 1989, p 2341 1. ValentineWN,Tanaka 2. Kanno H, Fujii H, Hirono H. Miwa S: cDNA cloning of human R-typepyruvatekinaseand identification of asingleamino acid substitution (Thr384 Met) affecting enzymatic stability in a pyruvate kinase variant (PK Tokyo) associated with hereditary hemolytic anemia. Proc Natl Acad Sci USA 88:8218, 1991 3. Kanno H, Fujii H, HironoA,Omine M. Miwa S: Identical point mutations of the R-type pyruvate kinase (PK) cDNA found in unrelated PK variants associated with hereditary hemolytic anemia. Blood 79:1347, 1992 4. Kanno H, Fujii H, Tsujino G , Miwa S: Molecularbasis of impaired pyruvate kinase isozyme conversion in erythroid cells: A singleaminoacidsubstitution near the activesite and decreased mRNA content of the R-type PK. Biochem Biophys Res Commun 192:46,1993 5. Kanno H, Fujii H, Miwa S: Low substrate affinity of pyruvate kinase variant (PK Sapporo) due to a single amino acid substitution (426Arg .-* Gln) associated with hereditary hemolytic anemia.Blood 81:2439, 1993 6. Neubauer M, Lakomek M, Winkler M, Parke S. Hofferbert S, Schroter W: Point mutations in the L-type pyruvate kinase gene of two children with hemolytic anemia caused by pyruvate kinase deficiency. Blood 77:1871, 1991 7. Nowak T, MildvanAS:Nuclearmagneticresonancestudies of the function of potassium in the mechanism of pyruvate kinase. Biochemistry 11:2819,1972 8. Kanno H, Fujii H, Miwa S: Structural analysis of human pyruvate kinase L-gene and identification of the promoter activity in erythroid cells. Biochem Biophys Res Commun 188516. 1992 9. Bowman HS, Procopio F: Hereditarynon-spherocytic hemolytic anemia of the pyruvate kinase deficient type. Ann Intern Med 58:567, 1963 10. Bowman HS. McKusick VA, Dronamraju KR: Pyruvate kinase deficient hemolyticanemia in anAmishisolate. Am J Hum Genet 17:1,1965 1I . Bowman HS. Oski FA: Laboratorystudies of erythrocyte pyruvatekinasedeficiency.Pathogenesis of the hemolysis. Am J Clin Pathol 70:259, 1978 12. Sambrook J, Fritsch EF, Maniatis T: Molecular Cloning. A Laboratory Manual (ed 2). Cold Spring Harbor, NY. Cold Spring Harbor Laboratory, 1989 13. Hopp TP, WoodsKR: Prediction of protein antigenic determinants from amino acid sequences. ProcNatl Acad Sci USA 78:3824. 1981 14. Ballas SK, Bator SM, Aubuchon JP, March WL, Sharp DE. Toy EM: Abnormal membrane physical properties ofred cells in McLeod syndrome. Transfusion 30:722, 1990 15. Ballas SK, Larner J, Smith ED, Surrey S, Schwartz E. Rappaport EF: The xerocytosis of Hb SC disease. Blood 69:124. 1987 16. Lonberg N. Gilbert W: Primary structure of chicken muscle 80:3661, 1983 pyruvate kinase mRNA. Proc Natl Acad Sci USA 17. Muirhead H, Clayden DA, Barford D, Lorimer CG, Fothergill-Gilmore LA, Schlitz E, Schmitt W:The structure of cat muscle pyruvate kinase. EMBO J 5:475, 1986 18. Noguchi T,Yamada K. Inoue H, Matsuda T, Tanaka T: The L- and R-type isozymes of rat pyruvate kinase are produced from a single gene by use of different promoters. J Biol Chem 26214366. 1987 19. Tani K, Yoshida MC, Satoh H, Mitamura K, Noguchi T, Tanaka T, Fujii H, Miwa S: Human M,-type pyruvate kinase. cDNA cloning, chromosomal assignment and expressionin hepatoma. Gene 73:509, 1988 20. Keitt AS: Pyruvate kinase deficiency and related disorders of red cell glycolysis. Am J Med 41:762, 1966 21. Mentzer WC, Baehner RL, Schmidt-Schoenbein H, Robinson From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 2316 SH, Nathan D G Selective reticulocyte destruction in erythrocyte pyruvate kinase deficiency. J Clin Invest 50:688, 1971 22. Muir WA, Beutler E, Wasson C: Erythrocyte pyruvate kinase deficiency in the Ohio Amish: Origin and characterization of the mutant enzyme. Am J Hum Genet 36:634, 1984 23. Imamura K, Tanaka T, Nishina T, Nakashima K, Miwa S: Studies on pyruvate kinase (PK) deficiency. 11. Electrophoretic, kinetic, and immunological studies on pyruvate kinase of erythrocytes and other tissues. J Biochem (Tokyo) 74:1165, 1973 24. Noguchi T, Inoue H,Tanaka T: The M1- and M2-type iso- KANNO ET AL zymes of rat pyruvate kinase are produced from the same gene by alternative RNA splicing. J Biol Chem 261:13807, 1986 25. Takenaka M, Noguchi T, Sadahiro S, Hirai H, Yamada K, Matsuda T, Imai E, Tanaka T Isolation and characterization of the human pyruvate kinase M gene. Eur J Biochem 198:101, 1991 26. Takenaka M, Noguchi T, Inoue H,Yam& K, Matsuda T, Tanaka T: Rat pyruvate kinase M gene. J Biol Chem 264:2363,1989 27. Imamura K, Tanaka T Multimolecular forms of pyruvate kinase from rat and other mammalian tissues. J Biochem (Tokyo) 71:1043, 1972 From www.bloodjournal.org by guest on June 17, 2017. For personal use only. 1994 83: 2311-2316 Molecular abnormality of erythrocyte pyruvate kinase deficiency in the Amish H Kanno, SK Ballas, S Miwa, H Fujii and HS Bowman Updated information and services can be found at: http://www.bloodjournal.org/content/83/8/2311.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.