Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
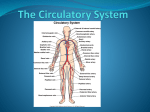
11/28/11 Overview of the Cardiovascular System The Heart: high-pressure pump Blood Vessels (vasculature): distribute blood to all parts of the body and return blood to the heart Blood: transport medium in which materials to be transported are dissolved or suspended 2 vascular (blood vessel) loops: Pulmonary circulation: from heart to lungs and back) Systemic circulation: from heart to other organs and back Overview of Cardiovascular System Functions Most basic and important function: to provide adequate blood flow to all the organs and tissues of the body Transport Respiratory gases: oxygen & carbon dioxide Nutrition: absorbed products of digestion Excretion: metabolic wastes delivered (to liver and kidneys) Regulation & Protection: hormones, immune cells, clotting proteins Regulation Hormones Thermoregulation (skin blood flow) Protection Blood clotting (protects against haemorrhage) Pathogens (immune system) Exchange between blood and tissue takes place in capillaries Blood gases: Pulmonary capillaries Blood entering lungs is deoxygenated Oxygen diffuses from tissue to blood (CO2 from blood to tissue) Blood leaving lungs is oxygenated Systemic capillaries Blood entering tissues is oxygenated Oxygen diffuses from blood to tissue (CO2 from tissue to blood) Blood leaving tissues is deoxygenated 1 11/28/11 Blood On average, 5L of blood (approx 8% body weight) Arterial Blood Leaving the heart Bright Red High oxygen content (oxyhaemoglobin) Venous blood Returning to the heart Darker colour Lower oxygen content (deoxyhaemoglobin) Cellular portion of blood (45% blood volume) a) Erythrocytes (red blood cells): oxygen transport b) Leukocytes (white blood cells): immune function c) Platelets: Blood clotting Plasma (55% blood volume) a) Water b) Dissolved solutes eg. ions c) Plasma proteins d) Other components eg. metabolites, hormones, enzymes, antibodies. Anatomy of the heart Size of fist Weighs approximately 250 – 350 grams Location Located in thoracic cavity - Diaphragm separates abdominal cavity from thoracic cavity 2 11/28/11 The Heart: anatomy Ventricle walls thicker Four chambers: 2 Atria & 2 Ventricles than atrial walls Dual pump: right & left sides Left ventricle wall Septum prevents mixture of blood between the 2 thicker than right sides ventricle wall Atria and ventricles separated by dense connective tissue: the fibrous skeleton (allows them to contract separately) Cardiac Muscle (myocardium) Gap junctions - Contracts as a unit Desmosomes - Resist stress Atria & Ventricles are separate units separated by fibrous skeleton 99% contractile cells 1% autorhythmic cells Function: Rhythmic contraction and relaxation generates heart pumping action Contraction pushes blood out of heart into vasculature Relaxation allows heart to fill with blood 3 11/28/11 Valves and Unidirectional Blood Flow Pressure within chambers of heart vary with heartbeat cycle Pressure difference drives blood flow: High pressure to low pressure Normal direction of flow: Atria to ventricles, then ventricles to arteries Valves prevent backward flow of blood All valves open passively based on pressure gradient Atrioventricular valves = AV valves R: tricuspid valve; L: bicuspid (mitral) Papillary muscles and chordae tendinae keep AV valves from everting Semilunar valves Aortic Valve Pulmonary Valve Electrical Activity of the Heart Autorhythmic cells generate their own rhythm Conduction System Pacemaker cells: Coordinate and provide rhythm to heartbeat The Sinoatrial (SA) node is the pacemaker of the heart Conduction fibers: Rapidly conduct action potentials initiated by pacemaker cells to myocardium Atrioventricular (AV) node Bundle of His Purkinje fibers 4 11/28/11 Spread of Excitation Atria contract first, then ventricles (fibrous skeleton) Coordination due to presence of gap junctions and conduction pathways Recording the Electrical Activity of the Heart with an Electrocardiogram ECG: non-invasive technique that tests for clinical abnormalities in electrical activity of the heart Body is conductor: currents in body spread to surface (ECG, EMG, EEG) Distance & amplitude of spread depends on size of potentials and synchronicity of potentials from other cells Cardiac electrical activity is synchronized Standard ECG Trace P wave atrial depolarization QRS complex ventricular depolarization T wave ventricular repolarization 5 11/28/11 Abnormal Heart Rates “Sinus rhythm”: generated by SA node Abnormal Heart Rates: Tachycardia- fast Bradycardia- slow Pathophysiology If the SA node is damaged, other cardiac cells can take over its pacemaker role. AV node and Purkinje fibres: these are latent pacemakers Artificial pacemakers can also be used Fibrillation Loss of coordination of electrical activity. Can be corrected by defibrillation Atrial fibrillation - weakness Ventricular fibrillation - death within minutes Damage to heart muscle Cardiac Cycle Events associated with the flow of blood through the heart during a single complete heartbeat Mechanical Events Systole - Ventricular contraction and blood ejection Diastole - Ventricular relaxation and filling Opening of Valves Valves open passively due to pressure gradients AV valves open when P atria > P ventricles Semilunar valves open when P ventricles > P arteries 6 11/28/11 Pressure & volume changes during cardiac cycle 1 START Isovolumic ventricular 5 relaxation: as ventricles relax, pressure in ventricles falls, blood flows back into cups of semilunar valves and snaps them closed. Ventricular ejection: 4 as ventricular pressure rises and exceeds pressure in the arteries, the semilunar valves open and blood is ejected. Late diastole: both sets of chambers are relaxed and ventricles fill passively. 2 Atrial systole: atrial contraction forces a small amount of additional blood into ventricles. Isovolumic ventricular 3 contraction: first phase of ventricular contraction pushes AV valves closed but does not create enough pressure to open semilunar valves. Ventricular Volume and Stroke Volume EDV = end diastolic volume = volume of blood in ventricle at end of diastole ESV = end systolic volume = volume of blood in ventricle at end of systole SV = stroke volume = volume of blood ejected from heart each cycle = SV = EDV - ESV 130 mL – 70 mL = 60 mL 7 11/28/11 Cardiac Output Volume of blood pumped by each ventricle per minute Cardiac Output = CO = SV x HR Equal on both sides of the heart Average CO = 5 litres/min at rest (70ml/beat x 70beat/min) Can increase 5-fold during exercise Regulation of Cardiac Output Regulate heart rate and stroke volume These can change from moment to moment Extrinsic and Intrinsic regulation Extrinsic - outside » hormones (adrenaline) » nerves (autonomic nervous system) Intrinsic - local Autonomic nervous system Efferent nervous system Autonomic (involuntary) Somatic (voluntary) Parasympathetic Sympathetic Motor Parasympathetic and sympathetic have opposing effects 8 11/28/11 Factors Affecting Cardiac Output Heart Rate Neuronal: Pacemaker (SA node) initiates contraction – innervated by autonomic nerves Parasympathetic slows heart rate (dominant at rest) Sympathetic increases heart rate Balance between sympathetic and parasympathetic is key Stroke Volume Primary factors affecting stroke volume 1) Afterload: Pressure in aorta during ejection This is the force that the heart must pump against 2) End-diastolic volume (preload) 3) Ventricular contractility Hormonal: Adrenaline (epinephrine) - same effect as sympathetic nervous system Glucagon - increases heart rate 2) EDV 3) ventricular contractility Length-Tension Curve (Starling Curve) for cardiac muscle End-diastolic volume is the preload – the work the heart must do. Increased EDV stretches the cardiac muscle fibres: closer to optimum length Next contraction is greater: increased SV Increased EDV= increased SV: this is called the Starling Effect An intrinsic mechanism ensures that venous return matches cardiac output – the heart pumps out the blood that is returned to it If ventricles contract with more force they eject more blood & SV increases Sympathetic nerves increase SV Parasympathetic have no effect Adrenaline increases SV 9 11/28/11 Autonomic regulation of Cardiac Output Remember: CO = HR x SV Autonomic nerves affect both variables to influence CO Increases in Cardiac Output: exercise CO can increase 5 fold during exercise Exercise affects HR and SV Influence of autonomic nerves Increased venous return eg via skeletal muscle pump One-way valves in peripheral veins Skeletal muscle contracts and squeezes veins: increased pressure Blood moves toward heart Blood cannot move backwards (valves) Skeletal muscle relaxes Blood flows into veins 10 11/28/11 Distribution of Cardiac Output at rest and during exercise Independent regulation of blood flow during exercise Cardiac output increases during exercise Distribution of blood does not increase proportionally Dilation to eg. skeletal muscle and heart increases blood flow Constriction to GI tract and kidneys decreases blood flow Overview of the Vasculature (Blood vessels) Heart →Arteries → Arterioles → Capillaries → Venules → Veins Arteries: relatively large, branching vessels that conduct blood away from the heart. Major artery is aorta Microcirculation Arterioles: small branching vessels with high resistance Capillaries: site of exchange between blood and tissues Venules: small converging vessels that drain blood to veins Veins: relatively large converging vessels that conduct blood to the heart. Major vein is vena cava (superior and inferior) Arteries branch; veins converge Differences between blood vessel types: Structure: diameter; composition of walls Function 11 11/28/11 Arteries Rapid transport pathway: large diameter - little resistance Under high pressure: walls contain elastic and fibrous tissue Arteries are pressure reservoirs Thick elastic arterial walls expand as blood enters arteries during systole & recoil during diastole Arteries & disease Atherosclerosis - ‘hardening of the arteries’ A plaque composed of cholesterol, calcium and other substances builds up in an artery Plaques reduce blood flow; they can rupture & cause clots – heart attacks or strokes can result Risk factors: age; smoking; diabetes; obesity Treatments: Angioplasty; stent implantation Arterioles Resistance vessels in microcirculation Connect arteries to capillaries Contain smooth muscle: regulate radius (& thus resistance; below) Arterioles provide greatest resistance to blood flow Largest pressure drop in vasculature (90 mmHg to 40 mmHg) Radius dependent on contraction state of smooth muscle in arteriole wall Vasoconstriction: increased contraction (decreased radius) Vasodilation: decreased contraction (increased radius) Functional importance Controlling blood flow to individual capillary beds Regulating mean arterial pressure Vasoactivity influenced by: Autonomic nerves (sympathetic constricts) Hormones (eg adrenaline constricts) Metabolism (eg. decreased O2 causes dilation) These factors therefore influence blood flow 12 11/28/11 Capillaries Site of exchange between blood and tissue Materials exchanged: O2, CO2, glucose, fatty acids, hormones etc. 1 mm length; 5-10 µm diameter (small diffusion distance) Walls - 1 endothelial cell layer plus basement membrane (small diffusion barrier) 10-40 billion per body; total SA = 600 m2 Most cells within 2 or 3 cell diameters of a capillary Capillaries can be continuous or fenestrated Fenestrated capllaries are more permeable. Located in kidneys, liver, intestines, bone marrow Cerebral vessels The arborizing network of cerebral arteries is demonstrated here in this cerebral angiogram seen laterally after injection of contrast into the right internal carotid artery Blood-brain barrier Tight junctions between endothelial cells lining cerebral blood vessels Prevents easy passage of large macromolecules and pathogens between the circulation and the brain 13 11/28/11 Venules Smaller than arterioles Connect capillaries to veins Thin walls Little smooth muscle in walls Some exchange of material between blood and interstitial fluid Veins Large diameter, but thin walls, which contain muscle and elastic tissue Valves allow unidirectional blood flow Volume reservoirs: at rest, systemic veins contain 60% of total blood volume Return of blood to heart from veins is called venous return Path of blood flow through cardiovascular system Cardiovascular system is a closed system Flow through systemic and pulmonary circuits are in series Left ventricle systemic circuit right atrium right ventricle pulmonary circuit left atrium left ventricle Flow within systemic (and pulmonary) circuit is in parallel: allows independent regulation of blood flow to organs 14 11/28/11 Blood Flow and Blood Pressure Physical laws governing blood flow: Pressure Gradients & Resistance in the Cardiovascular System Pressure gradients: Flow occurs from high pressure to low pressure Heart creates the pressure gradient for flow of blood A gradient must exist throughout circulatory system to maintain blood flow Resistance: systemic circuit is high pressure (gradient is approx 90mmHg), high resistance; pulmonary circuit is low pressure (gradient is approx 15mmHg), low resistance Pressures throughout the vasculature are variable Flow = ΔP/R = pressure gradient/resistance Pressure gradient across systemic circuit Pressure gradient = pressure in aorta minus pressure in vena cava just before it empties into right atrium Pressure in aorta = mean arterial pressure (MAP) = 90 mm Hg Pressure in vena cava = central venous pressure (CVP) = 0 mm Hg Pressure gradient = MAP – CVP = 90 – 0 = 90 mm Hg 15 11/28/11 Resistance in the Cardiovascular System The lower the resistance, the greater the flow Factors affecting resistance to flow Poiseuille’s Law R= 8ηL πr4 8 & π = constants L=length of vessel (normally doesn’t change) η=viscosity of fluid (normally doesn’t change) r=radius of vessel In arterioles (and small arteries) – radius is regulated RADIUS IS THE MOST IMPORTANT FACTOR Flow = ΔP/R = ΔPπ r4 8ηL Regulate blood flow by regulating radius: vasoactivity Vasodilation & vasoconstriction Functional importance Controlling blood flow to individual capillary beds Regulating mean arterial pressure Vasoactivity influenced by: Autonomic nerves (sympathetic constricts) Hormones (eg adrenaline constricts) Metabolism (eg. decreased O2 causes dilation) These factors therefore influence blood flow Control of blood flow distribution to organs Regulation of organ blood flow based on need (eg to skeletal muscles during exercise) Regulated by varying radius (and therefore resistance) Organ blood flow = MAP / organ resistance ie driving force for blood flow resistance to flow in that organ For any given P gradient, blood flow changes when resistance changes 16 11/28/11 Distribution of Cardiac Output at rest and during exercise Independent regulation of blood flow during exercise Cardiac output increases during exercise Distribution of blood does not increase proportionally Dilation to eg. skeletal muscle and heart increases blood flow Constriction to GI tract and kidneys decreases blood flow Blood pressure: Mean Arterial Pressure MAP = driving force for blood flow F = ΔP/R Regulating MAP critical to normal function MAP < normal: Hypotension Clinical risk: Inadequate blood flow to tissues MAP > normal: Hypertension Clinical risk: Stress on heart and walls of blood vessels (heart attack, stroke) Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember the importance of vasodilation and vasoconstriction) This means that MAP is completely determined by HR, SV & TPR 17 11/28/11 Short- and long-term regulation of MAP Short-term regulation: seconds to minutes Involves heart and blood vessels Primarily neuronal control Long-term regulation: minutes to days Regulation of blood volume Involves kidneys Primarily hormonal control Short-Term Regulation of MAP The baroreceptor reflex: A negative feedback loop that helps maintain normal blood pressure Baroreceptors are stretch receptors (mechanoreceptos) Arterial baroreceptors High pressure baroreceptors Sinoaortic baroreceptors Location Carotid sinus Aortic arch 18 11/28/11 Cardiovascular Control Centre Medulla oblongata Integration center for blood pressure regulation Output • Sympathetic nerves • Parasympathetic nerves Sympathetic: SA node (increase HR) Ventricles (increase contractility) Arterioles (increase resistance) Veins (increase venomotor tone) Parasympathetic: SA node (decrease HR) Major neural pathways in the control of cardiovascular function Components of Baroreceptor Reflex Detectors = baroreceptors Afferents = nerves Integration center = cardiovascular control center Efferents = autonomic nervous system Effectors = heart, arterioles, veins Example: a person who had been lying down stands up quickly • Gravity causes venous pooling in the legs. • This causes a decrease in VR, causing a decrease in CO • This causes a decrease in blood pressure. • Baroreceptors sense the decrease: reflex occurs • The reflex causes increased sympathetic and decreased parasympathetic activity. • CO and TPR are increased. • Blood pressure is increased back to normal. 19 11/28/11 Baroreceptor Reflex in response to a decrease in MAP 20