Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Aortic stenosis wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
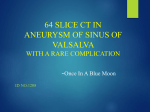
European Journal of Cardio-thoracic Surgery 22 (2002) 517–520 www.elsevier.com/locate/ejcts Surgical treatment of dissecting aneurysm of the interventricular septum Qingyu Wu*, Jianping Xu, Xiangdong Shen, Dongjin Wang, Shuiyun Wang Department of Cardiac Surgery, Cardiovascular Institute and Fu Wai Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing 100037, People’s Republic of China Received 4 August 2001; received in revised form 12 June 2002; accepted 17 June 2002 Abstract Objective: We reviewed our experience in the surgical treatment of an extremely rare disease, dissecting aneurysm of the interventricular septum (DAIS). The definition of DAIS is that the interventricular septum is dissected and forms an aneurysm which bulges into both the left and right ventricles, causing obstruction of both ventricular outflow tracts. It communicates with the aortic root, and may communicate with the ventricle. It is usually associated with aortic valve regurgitation and aortic annular enlargement. DAIS might also be related to the sinus of Valsalva aneurysm [Ann Thorac Surg 65 (1998) 735; Ann Thorac Surg 51 (1991) 996; Eur J Thorac Surg 12 (1997) 759]. But in three of our six patients DAIS was not associated with sinus of Valsalva enlargement or aneurysm. Methods: Between May 1992 and November 2000, six of 30,701 patients were diagnosed with DAIS, and underwent surgery at Fu Wai Hospital in Beijing. Aortic valve replacement was performed in five patients, and the perforation at the bottom of the right sinus of Valsalva was repaired in one. The aneurysm was resected simultaneously in all these patients. Results: One of the six patients required re-operation. And all patients recovered uneventfully without hospital mortality. Conclusions: DAIS has a progressive course and poor prognosis. Early diagnosis and surgical treatment are mandatory. q 2002 Elsevier Science B.V. All rights reserved. Keywords: Interventricular dissecting aneurysm; Cardiac surgery 1. Introduction Dissecting aneurysm of the interventricular septum (DAIS) is rare. The aneurysm involves the ventricular septum, and is usually associated with aortic valve regurgitation and obstruction of the left and right ventricular outflow tracts [1]. It communicates with the aortic root, and may communicate with the ventricle. The etiological factors included enlargement or aneurysm of the sinus of Valsalva, trauma, bacterial endocarditis, and congenital myocardial developmental anomaly [2–4]. In this article, we reviewed our surgical experience in six patients, and discussed the preoperative diagnosis and surgical technique of treating this rare disorder. 2. Patients and methods Six of 30,701 patients were diagnosed with DAIS and operated on at Fu Wai Hospital from May 1992 to November 2000. There were five males and one female, with ages ranging from 22 to 50 years. Three patients presented with * Corresponding author. Fax: 186-10-6833-2376. E-mail address: [email protected] (Q. Wu). severe congestive heart failure. One patient had a history of chest trauma and III A-V block; another had undergone a remote aortic valve replacement and repair of a ruptured right sinus of Valsalva aneurysm a year before his present admission (Table 1). No patients had history of infection preoperatively. Electrocardiogram (ECG) revealed complete A-V block in two patients, requiring a permanent and a temporary pacemaker, respectively, before surgery. The chest roentgenograms showed increased pulmonary vascular markings and left ventricle enlargement in five patients. In patient 6, pulmonary vascular markings decreased due to the obstruction of the right ventricular outflow tract caused by DAIS. Echocardiography demonstrated the diagnosis of DAIS in all patients, which was confirmed by angiography (Fig. 1). Magnetic resonance imaging (MRI) and electron beam computed tomography were used in three patients. The operation was performed using hypothermic cardiopulmonary bypass with antegrade cold crystalloid or cold blood cardioplegia in all six patients. The aneurysmal wall was resected and the cavity closed (Figs. 2 and 3). In five of the six patients, a Dacron patch was used to repair the ventricular septal defect (VSD) created after resection of DAIS. In the other one patient, DAIS was not resected, 1010-7940/02/$ - see front matter q 2002 Elsevier Science B.V. All rights reserved. PII: S 1010-794 0(02)00375-5 518 Q. Wu et al. / European Journal of Cardio-thoracic Surgery 22 (2002) 517–520 Table 1 Preoperative patient data a No. Sex Age (years) Clinical NYHA Class History 1 2 3 4 5 6 Male Male Male Male Male Female 39 50 46 22 27 38 CHF CHF CHF Dyspnea, palpitations Dyspnea Angina III IV II III IV IV NS Chest trauma, TPI AVR, PPI NS NS NS a AVR, aortic valve replacement; CHF, congestive heart failure; NS, nothing special; NYHA, New York Heart Association; PPI, permanent pacemaker implantation; TPI, temporary pacemaker implantation. and the VSD was repaired with tissue of DAIS wall. Associated aortic valve replacement was performed in five patients. In patient 4, the perforation at the bottom of the right sinus of Valsalva was repaired with an autologous pericardial patch; in patient 1, aortic periprosthetic leakage and heart failure were found 2 months postoperatively so that a reoperation was required. The periprosthetic leak, with a size of 1 £ 1.8 cm, was found beneath the right coronary cusp area. At the upper part of the dissecting aneurysm, the aneurysmal wall disrupted from the prosthetic ring and formed a defect of 2 £ 1.5 cm between two ventricles. After resection of the whole aneurysmal wall via right ventriculotomy, a large Dacron patch of 4.5 £ 7 cm was used to repair the defect with three interrupted mattress stitches at the muscular section of the ventricular septum and with a 4/ 0 prolene running suture in the remaining margin. The periprosthetic leak was closed via aortotomy. Operative findings and techniques are presented in Table 2. 3. Results There was no operative mortality. In patient 2, a permanent pacemaker was implanted 1 month postoperatively; in patient 3, sinus rhythm recovered after surgery. All patients recovered well in the follow-up study (range, 4 months to 8 Fig. 1. DAIS was detected by echocardiography in patient 1 (short axis). Diastolic (left) and systolic (right). A, aorta; B, DAIS. years; mean, 3.58 ^ 3.54 years). Chest X-ray plain films and ECGs indicated no DAIS recurrence. Both prosthetic and native aortic valves were functioning quite well. The postoperative cardiac function was NYHA Class I in four patients, and Class II in two, respectively (Fig. 4). 4. Discussion DAIS is quite rare. In a literature review, the aneurysm originated from the right sinus of Valsalva in 40 of the 44 cases of DAIS [1,5,6]. It was believed that ruptured sinus of Valsalva aneurysm caused DAIS [1,3,5]. But among our six patients, a coronary sinus of Valsalva aneurysm was found in three patients (patients 1, 3 and 6). The data of patients 1 and 2 have been reported [7]. In patient 2, the sinus of Valsalva was normal, but the right coronary cusp was deformed; in patient 4, a perforation with the diameter of 2 cm was found at the bottom of the right coronary sinus of Valsalva; in patient 5, the coronary sinus of Valsalva presented normal, but the aortic annulus of the right coronary sinus and the ventricular septum were disconnected completely. So we think that ruptured sinus of Valsalva aneurysm is not the only cause of DAIS; pathological Fig. 2. DAIS was detected by echocardiography in patient 1 (longitudinal axis). Diastolic (left) and systolic (right). Q. Wu et al. / European Journal of Cardio-thoracic Surgery 22 (2002) 517–520 519 Fig. 4. Taking thrombosis (A) from DAIS via right ventriculotomy in patient 6. Fig. 3. Cavity of DAIS (B) was shown via right ventriculotomy in patient 4. The interventricular septum (A) was dissected into two sections. changes mainly in the ventricular septum should not be overlooked. The etiology of this disease still remains obscure. The coronary sinus of Valsalva aneurysm compresses coronary arteries, and this may lead to ventricular septal ischemia [8]. Other potential causes include intra-septal myocardial rupture, hematoma formation and coronary arterial dysplasia [1,6]. In three of our six patients, the sinus of Valsalva was normal. We believed that the sinus of Valsalva aneurysm was not the only cause of DAIS. The upper part of the ventricular septum was compressed by coronary sinus of Valsalva aneurysm, and injured by blood flush, which might lead to the DAIS formation. Inherited embryological defects of the aortic annulus and the ventricular septal myocardium may also contribute to the development of this pathology [4,9]. DAIS is usually associated with aortic insufficiency of moderate to severe degree [1]. Among our six patients, five had severe aortic valve regurgitation, and three had congestive heart failure. The right aortic valve cusp was Table 2 Operative findings and techniques a No. Approach Aortic valve SV DAIS Operation 1 AO, RVOT RCC deformed, severe AI LSV unruptured 3 £ 5 £ 3 cm Repair aneurysm of LSV, close DAIS cavity, AVR 2 AO, RVOT RCC deformed, severe AI, annular dilation Normal 3 AO, RVOT, RA RSV repaired 4 AO, RVOT, RA Perivalvular leakage beneath RCC area Normal 5 £ 8 £ 6 cm, communication to AO, RV 5 £ 4 £ 6 cm, thrombosis inside, intima fibrosis 4 £ 5 £ 6 cm RSV perforation at bottom, 2 cm in diameter 4 £ 5 £ 6 cm 5 AO, RVOT Normal 4 £ 0.5 £ 3 cm 6 AO, RVOT, PA AI, RCC discontinued to the annulus AI, RCC absent RSV ruptured 6 £ 8 £ 7 cm, thrombus Close DAIS cavity, AVR Resect DAIS, Dacron patch repair, AVR Resect DAIS, Dacron and pericardial patch repair, tricuspid annularplasty Resect DAIS, pericardial patch repair, AVR Resect DAIS, Dacron patch repair, AVR a AO, aorta; AI, aortic valve insufficiency; AVR, aortic valve replacement; SV, coronary sinus of Valsalva; DAIS, dissecting aneurysm of interventricular septum; LSV, left coronary sinus of Valsalva; RA, right atrium; RCC, right coronary cusp of aortic valve; RSV, right coronary sinus of Valsalva; RV, right ventricle; RVOT, right ventricular outflow tract. 520 Q. Wu et al. / European Journal of Cardio-thoracic Surgery 22 (2002) 517–520 thickened and deformed in three patients, and was completely absent in one. In addition, annular dilation and annular cusp disruption also contributed to aortic insufficiency. Clinical manifestations revealed obstruction of one or both ventricular outflow tracts, congestive heart failure, arrhythmia, A-V block, etc. The diagnosis of DAIS can be made by echocardiography. It can detect the site and size of dissecting aneurysm, its relation with the left and right ventricles, and any abnormality in the aortic valve. Nowadays, color Doppler can easily show aortic regurgitation, vortex flow in the DAIS cavity, and communication between DAIS and left or right ventricle. Aside from echocardiography, MRI and angiography of the ascending aorta, aortic root, and ventricles have been proven helpful in the diagnosis of this disease. DAIS differs from aortic root abscess both in clinical manifestation and in pathological changes. Patients with aortic root abscess often have signs and symptoms of infection over a long period of time. Even when the infection is controlled and the pus absorbed, the cystic wall becomes thickened and severely fiberized. The abscess cyst is usually not so large. DAIS is involved mainly in the ventricular septum; thrombus, instead of abscess, is usually found inside the cavity that communicates with the left ventricle. The objective of the operation in patients with DAIS is to restore the function of the aortic valve and the integrity of the ventricular septum, to resect the aneurysm, and to obliterate the obstruction of the left and right ventricular outflow tracts, so as to improve the heart function. Aortotomy and right ventriculotomy provide good exposure for resecting the aneurysm and repairing the VSD after DAIS is resected. Resecting the DAIS wall should be tailored to each patient. In four of the six patients, the wall was resected completely; a Dacron patch was used to repair the VSD when the aortic valve was replaced, and its adjacent aortic annulus was firmly attached to the VSD margins, and positioned to the sewing ring of the prosthetic valve. It is undesirable to close the aneurysmal wall directly if the tissue is edematous and weak, which may lead to perivalvular leakage, communication between two ventricles as well as heart failure. In patient 2, the DAIS was probably caused by trauma; the aneurysmal wall was strong enough to keep the ventricular septum intact after the aneurysmal cavity was closed with five interrupted and pledgeted mattress sutures. In patient 4, the DAIS was probably related to the perforation of the right sinus of Valsalva. Since the ventricular septum did not equally split in this case, the aneurysmal wall was thin on the left side. A good surgical result was achieved by resecting the aneurysmal wall and repairing the perforation of the right sinus of Valsalva. Because of the high pressure in the DAIS cavity and its excessive extension into the ventricular septum, severe tricuspid insufficiency and separation between the septal and anterior tricuspid leaflets developed. Tricuspid insufficiency was repaired successfully using the DeVega technique. DAIS is usually associated with aortic valvular abnormalities [1,5], therefore, aortic valve replacement is often necessary. According to our experience, it is better to put interrupted pledgeted mattress stitches from the upper part of the ventricular septum to the aortic annulus via the right ventriculotomy, utilizing a suitable-sized prosthetic valve. A temporary pacing should be inserted transvenously, and temporary pacing wires applied to the epicardium during the operation. If complete heart block persists, permanent pacemaker implantation is essential 1–2 weeks postoperatively. DAIS has a progressive course and poor prognosis. All patients underwent surgery 13 days to 6 months after the symptoms of DAIS first occurred. Its preoperative complications include obstruction of the left and right ventricular outflow tracts, arrhythmia, complete heart block, and communication with the left ventricle, which may result in intractable heart failure. Early diagnosis and surgical intervention are mandatory. References [1] Choudhary SK, Bahn A, Reddy SCB, Sharma R, Murari V, Airan B, Kumar AS, Venugopal P. Aneurysm of sinus of Valsalva dissecting into interventricular septum. Ann Thorac Surg 1998;65:735–740. [2] Engel PJ, Held JS, van der Bel-Kahn J, Spitz H. Echocardiographic diagnosis of congenital sinus of Valsalva aneurysm with dissection of the ventricular septum. Circulation 1981;63:705–711. [3] Raffa H, Mosieri J, Sorefan AA, Kayali MT. Sinus of Valsalva aneurysm eroding into the interventricular septum. Ann Thorac Surg 1991;51:996–998. [4] Fasoli G, Della Valentina P, Scognamiglio R. Echocardiographic findings in left ventricular septal aneurysm. Int J Cardiol 1988;18:441–443. [5] Bapat VN, Tendolka AG, Khandeparkar J. Aneurysms of sinus of Valsalva eroding into the interventricular septum: etiopathology and surgical considerations. Eur J Thorac Surg 1997;12:759–765. [6] Vaideeswar P, Kaliamoorthy A. Aneurysm of sinus of Valsalva with extensive dissection of interventricular septum and left ventricular free wall. Int J Cardiol 2001;77:93–95. [7] Wu Q. Surgical treatment of dissecting aneurysm of the interventricular septum. Ann Thorac Surg 1997;63:545–547. [8] Gallet B, Combe E, Saudemont JP, Tetard C, Barret F, Gandjbakhch I, Hiltgen M. Aneurysm of the left aortic sinus causing coronary compression and unstable angina: successful repair by isolated closure of the aneurysm. Am Heart J 1988;115:1308–1310. [9] Sawyer AJ, Mauss IH, Rosenblaff P. Congenital diverticulosis of left ventricle. Am J Dis Child 1950;79:117.