Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Adaptive immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Innate immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Molecular mimicry wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
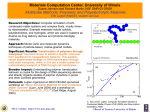
New Insights on Merkel Cell Carcinoma Emory Melanoma / Skin Cancer Symposium Saturday, Feb 27, 2016; Emory Conference Center 35 min talk + 10 min questions Paul Nghiem, MD, PhD Professor & Head, UW Dermatology/Medicine & Pathology George F. Odland Endowed Chair in Dermatology Clinic: Seattle Cancer Care Alliance Fred Hutchinson Cancer Research Center Research: Univ of WA Lake Union Campus UV DNA Damage/Cell cycle Merkel cell carcinoma Overview • Pathogenesis & the Merkel polyomavirus – Risk factors – Viral oncogenesis Overview • Pathogenesis & the Merkel polyomavirus – Risk factors – Viral oncogenesis • Tumor / viral immunity – Humoral and cellular immunity Overview • Pathogenesis & the Merkel polyomavirus – Risk factors – Viral oncogenesis • Tumor / viral immunity – Humoral and cellular immunity • Therapy – Current & future immune-based therapies Why is MCC important? • More lethal than melanoma – ~40% mortality (~15% for melanoma) Why is MCC important? • More lethal than melanoma – ~40% mortality (~15% for melanoma) • Reported incidence increasing – Quadrupled since 1986 – Currently ~2,000 new cases/yr in USA Why is MCC important? • More lethal than melanoma – ~40% mortality (~15% for melanoma) • Reported incidence increasing – Quadrupled since 1986 – Currently ~2,000 new cases/yr in USA • Optimal therapy is unique among skin CAs – Proper tx is relatively benign, effective What is a Merkel Cell? Friedrich Merkel, 1875 Mechanoreceptors in basal layer of epidermis? What is a Merkel Cell? Friedrich Merkel, 1875 Mechanoreceptors in basal layer of epidermis? copyright: Paul Nghiem & Paul Quade, www.EchoMedicalMedia.com What is a Merkel Cell? Friedrich Merkel, 1875 Mechanoreceptors in basal layer of epidermis? • Essential for light touch Maricich, et al, Science, 2009 • Derived from epidermis (not neural crest) Van Keymeulen, et al, J Cell Biol, 2009 Morrison, et al, Dev Biol, 2009 copyright: Paul Nghiem & Paul Quade, www.EchoMedicalMedia.com Merkel cell CA: clinical appearance (easy to miss) Clinician’s Impression at the Time of Bx in 106 MCC pts BENIGN 56% • Cyst/Acneiform lesion • Lipoma • Dermatofibroma MALIGNANT • • • • 32% 6% 5% 36% Non-melanoma skin CA Lymphoma Metastatic Carcinoma MCC Indeterminate • "Nodule" 19% 6% 2% 1% 8% Heath, JAAD, 2008 "Perinuclear dot pattern" of cytokeratin-20 MCC Reported Incidence is Rising 1500 new cases/yr in USA in 2005 (NCDB data) Lemos & Nghiem JID 2007 Many cases ‘missed’ CK20 antibody 1600 new cases/yr in USA in 2006 (SEER data) Albores-Saavedra J Cut. Path 2009 Increase in Risk Factors • Prolonged sun exposure – 98% Caucasian; Latitude associated; sunexposed skin • Immune suppression (HIV, SOTR, CLL) • Age > 50 Paulson & Nghiem, unpublished Clinical appearance (easy to miss) Clinical Presentation Generic description: "Firm papule / nodule, often red or purple" We wanted more concrete data… A: Asymptomatic E: Expanding rapidly I: Immune Compromised O: Older than 50 U: UV-exposed, fair skin 89% of MCCs: ≥ 3 features (sensitive, NOT specific!) A: Asymptomatic E: Expanding rapidly I: Immune Compromised O: Older than 50 U: UV-exposed, fair skin 89% of MCCs: ≥ 3 features (sensitive, NOT specific!) If red, rapidly growing, non-tender nodule on sun-exposed skin of pt over 60: ? biopsy MCC Presenting Site In 138 patients Heath, JAAD, 2008 MCC Presenting Site In 138 patients Skin: Primary MCC (n= 123) Nodal Presentation (n=15) (no primary) thought experiment... Assuming there is palpable nodal disease... better to have a primary or not? Heath, JAAD, 2008 How does one stage an MCC patient? 2010 AJCC Staging System Replaced 5 conflicting staging systems... How does one stage an MCC patient? 2010 AJCC Staging System Replaced 5 conflicting staging systems... Bianca Lemos, MD AJCC MCC Staging System (2009) – Stage I: • Ia: • Ib: – Stage II: • IIa: • IIb: • IIc: – Stage III: • IIIa: • IIIb: – Stage IV: Local, ≤ 2cm Nodes negative by path exam Nodes not clinically detectable Local, > 2cm Nodes negative by path exam Nodes not clinically detectable Primary tumor invading bone/muscle/fascia/cartilage Regional Nodal Disease Nodes pos by path exam and not clinically detectable Nodes clinically detectable; in-transit metastasis Distant Metastatic Disease How predictive was the 7th Edition system? Analysis with an independent (subsequent) cohort Can we make it better? published 2009 Local disease (n=213; MCC-specific survival) IA (n=112) MCC-specific survival (%) 100 IB (n=48) 75 IIA (n=32) 50 IIB (n=21) 25 0 0 1 2 3 4 5 6 7 8 Time from diagnosis (years) 9 10 11 Nodal and distant disease (n=215; MCC-specific survival) MCC-specific survival (%) 100 75 IIIA (n=78) 50 IIIB (n=111) 25 IV (n=26) 0 0 1 2 3 4 5 6 Time from diagnosis (years) 7 8 Nodal and distant disease (n=215; MCC-specific survival) MCC-specific survival (%) 100 75 IIIA (n=78) 50 IIIB (n=111) known or unknown primary? 25 IV (n=26) 0 0 1 2 3 4 5 6 Time from diagnosis (years) 7 8 IIIB Patients by Primary Lesion Status (n=111; MCC-specific survival) MCC-specific survival (%) 100 IIIB Unknown Primary Lesion (n=62) 75 50 IIIB Known Primary Lesion (n=49) 25 0 Univariate analysis by competing risks regression: HR 0.31; p<0.01; 95% CI 0.16 – 0.60 Multivariate analysis by competing risks regression: (controlling for age at dx, sex, and immune suppression) HR 0.43; p=0.04; 95% CI 0.20 – 0.94 0 1 2 3 4 5 6 Time from diagnosis (years) 7 8 “Unknown primary” lesion better survival across independent cohorts 80 Unknown primary (76%) Unknown primary (65%) 70 % Survival 60 Unknown primary (57%) 50 40 Known primary (36%) 30 Known primary (28%) Known primary (33%) 20 10 0 2 year overall survival (Tarantola et al; n=50) 5 year MCC-specific survival (Seattle; n=104) 5 year MCC-specific survival (Busam et al; n=115) Among Stage IIIB Patients the Presence or Absence of a Primary Matters Known primaries Poorly functioning immune cells cannot eliminate the primary tumor Poorly functioning immune cells Primary tumor Positive Positive lymph node lymph node Among Stage IIIB Patients the Presence or Absence of a Primary Matters Known primaries Poorly functioning immune cells Poorly functioning immune cells cannot eliminate the primary tumor Primary tumor Positive Positive lymph node lymph node Unknown primaries Functional killer T cells secrete effector cytokines or molecules to destroyed the primary tumors. These patients do much better!! Highly functioning immune cells Primary Tumor gone Positive lymph node % with Unknown Primary The immune system likely mediates regression of primary tumors 100% 80% 66% 60% 40% p < 0.0001 (Fisher’s exact) 20% 0%!! 0% Immune Suppressed IIIb cases: (n = 11 ) Not Immune Suppressed (n = 92) % with Unknown Primary The immune system likely mediates regression of primary tumors 100% 80% 66% 60% 40% p < 0.0001 (Fisher’s exact) 20% 0%!! 0% Immune Suppressed IIIb cases: (n = 11 ) Not Immune Suppressed (n = 92) Bottom line on initial therapy... Surgery & radiation: >95% of patients ‘free of detectable disease’... but MCC recurs in nearly half Bottom line on initial therapy... Surgery & radiation: >95% of patients ‘free of detectable disease’... but MCC recurs in nearly half Metastatic MCC chemotherapy (‘small cell regimen’) - shrinks MCC in most cases - over half progress by 3 mos... Chemotherapy & metastatic MCC PFS after 1st line chemo Iyer, et al, in preparation 53% of patients ‘respond’... Half progress by 93 days after starting chemo (Quite toxic therapy...unsatisfactory results...need options!) Given links to immune suppression, UV... how does MCC arise? A new human virus that causes cancer (in 2008) Moore/Chang (KSHV) Present in 8/10 MCCs Schematic of MCPyV genome Validated in dozens of studies Virus (MCPyV) is extremely common! Virus on us all yet only 1 in 3000 will get MCC…how? Adapted from Bhatia/Afanasiev, et al, Curr Oncol Rep, 2011 Virus on us all yet only 1 in 3000 will get MCC…how? What are mutation patterns in virus-pos vs virus-neg tumors? Adapted from Bhatia/Afanasiev, et al, Curr Oncol Rep, 2011 3 studies in late 2015... genetic mutations in viruspos & virus-neg MCC... 3 studies in late 2015... genetic mutations in viruspos & virus-neg MCC... 3 studies in late 2015... genetic mutations in viruspos & virus-neg MCC... “MCC-High” “MCC-Low” 49 MCCs... Goh, et al. 2015. Oncotarget “MCC-High” “MCC-Low” 49 MCCs... Goh, et al. 2015. Oncotarget “MCC-High” “MCC-Low” 49 MCCs... Goh, et al. 2015. Oncotarget Viral status greatly affects mutation frequency Goh, et al. 2015. Oncotarget Viral status greatly affects mutation frequency 100-fold difference between MCC-Lo & MCC-Hi Goh, et al. 2015. Oncotarget Virus-negative MCCs ‘neoantigens’ Goh, et al. 2015. Oncotarget PDL1-pos (‘immune visible’) tumors have more mutations Wong, et al. 2015. Cancer Res. PDL1-pos (‘immune visible’) tumors have more mutations Virus-neg tumors may be immunogenic... We will return to this! Wong, et al. 2015. Cancer Res. Humoral immunity: a powerful biomarker Kelly Paulson, MD, PhD Denise Galloway, PhD Jody Carter, PhD Mark Wener, MD Will Simonson,MD, PhD Antibodies to T-Ag (not capsid) fall after tx Antibodies to T-Ag (not capsid) fall after tx Capsid antibodies: >60% of us have them! T-Ag antibodies: <1% of 530 population controls ~50% of newly diagnosed MCCs Antibodies to T-Ag (not capsid) fall after tx Capsid antibodies: >60% of us have them! T-Ag antibodies: <1% of 530 population controls ~50% of newly diagnosed MCCs Antibodies to T antigen reflect disease burden “This could be clinically useful...” Paulson, Carter, et al, CA Research, 2010 Detecting MCC recurrences using serology PPV = 66% NPV = 97% Paulson, et al, submitted MCC Specific Survival by Oncoprotein Ab Titer 100 MCC specific Survival (%) Oncoprotein Ab Positive (n = 114) 75 Oncoprotein Ab Negative (n = 105) 50 25 0 Competing-risks Regression Controlling for: Age, Stage, and Sex p = 0.037 Paulson, et al, submitted Hazard Ratio = 0.46 95% CI = 0.224 – 0.955 0 1 2 3 Time after Diagnosis (Days) 4 5 59 MCC Specific Survival by Oncoprotein Ab Titer 100 MCC specific Survival (%) Oncoprotein Ab Positive (n = 114) 75 Oncoprotein Ab Negative (n = 105) 50 25 0 Sero-neg patients: follow with scans Competing-risks Regression Controlling for: Age, Stage, and Sex p = 0.037 Paulson, et al, submitted Hazard Ratio = 0.46 95% CI = 0.224 – 0.955 0 1 2 3 Time after Diagnosis (Days) 4 5 60 Assay ‘live’ (available) as of January 2014... Run by UW Lab Medicine (50 ul serum) Cost $200 (very modest vs CT scan) Helps both virus-pos and virus-neg patients... Antibodies are useful for tracking MCC... What are T cells good for? Antibodies are useful for tracking MCC... What are T cells good for? Survival!! If CD8+ T cells are moderate or high within tumor, survival is 100% (n=146 patients + n=150 patients) How do CD8 T cells recognize their target? killer CD8 T cell MCC cell expressing MCPyV protein Finding MCPyV-specific T cells David Koelle MCPyV-Antigen source MCPyV proteome map Jayasri Iyer x x x x Finding MCPyV-specific T cells David Koelle MCPyV-Antigen source Persistently expressed in MCCs MCPyV proteome map x x x x 95 peptides: covering 389 AA Jayasri Iyer Finding MCPyV-specific T cells David Koelle T cell source Blood MCPyV-Antigen source “TIL” Persistently expressed in MCCs MCPyV proteome map x x x x 95 peptides: covering 389 AA Jayasri Iyer Finding MCPyV-specific T cells David Koelle T cell source Blood MCPyV-Antigen source “TIL” Persistently expressed in MCCs MCPyV proteome map x x x x 95 peptides: covering 389 AA Antigen presenting cells Assay: T cells produce IFN-γ if recognize peptide Jayasri Iyer First 26 MCPyV epitopes identified from blood and MCC tumors MCPyV MCPyV proteome map x x x x Persistently expressed in MCCs 95 peptides: covering 389 AA epitopes discovered ‘Tools’ for MVPyV-specific T cell study Iyer, et al, Clin Ca Res, 2011 Iyer/Afanasiev et al, CCR, 2011; Afanasiev et al, submitted % subjects with tet+ T cells ‘Tools’ for MVPyV-specific T cell study Iyer, et al, Clin Ca Res, 2011 Iyer/Afanasiev et al, CCR, 2011; Afanasiev et al, submitted 0% Control subjects MCC patients (n=10) (n=9) Why do virus-positive tumors grow if patients have virus-specific T cells?? Virus infected cell CD8 T cell Jim Dowdalls/Photo Researchers, Inc Are virus-specific T cells dysfunctional? T cell surface receptor phenotype reveals functional profile Activated cells, characterized by expression of: Acute antigen exposure Adapted from Afanasiev, Nghiem, MCC book chapter CD28 Co-stimulatory receptor (ligand: B7); required for T cell activation CD69 Earliest inducible cell surface glycoprotein during T cell activation; plays a role in T cell proliferation CD137 (41BB) Member of TNF-receptor family; induced by T cell activation; important in T cell proliferation, cytokine secretion and cytotoxicity CD38 Cyclic ADP ribose hydrolase; marker of T cell activation; functions in cell adhesion, signal transduction and calcium signaling HLA-DR MHC class-II surface receptor that is upregulated with T cell activation T cell surface receptor phenotype reveals functional profile Activated cells, characterized by expression of: Acute antigen exposure Adapted from Afanasiev, Nghiem, MCC book chapter CD28 Co-stimulatory receptor (ligand: B7); required for T cell activation CD69 Earliest inducible cell surface glycoprotein during T cell activation; plays a role in T cell proliferation CD137 (41BB) Member of TNF-receptor family; induced by T cell activation; important in T cell proliferation, cytokine secretion and cytotoxicity CD38 Cyclic ADP ribose hydrolase; marker of T cell activation; functions in cell adhesion, signal transduction and calcium signaling HLA-DR MHC class-II surface receptor that is upregulated with T cell activation T cell surface receptor phenotype reveals functional profile Activated cells, characterized by expression of: Acute antigen exposure CD28 Co-stimulatory receptor (ligand: B7); required for T cell activation CD69 Earliest inducible cell surface glycoprotein during T cell activation; plays a role in T cell proliferation CD137 (41BB) Member of TNF-receptor family; induced by T cell activation; important in T cell proliferation, cytokine secretion and cytotoxicity CD38 Cyclic ADP ribose hydrolase; marker of T cell activation; functions in cell adhesion, signal transduction and calcium signaling HLA-DR MHC class-II surface receptor that is upregulated with T cell activation T cell Exhausted T cells, characterized by prolonged expression of: PD-1 Programmed death-1; inhibitory T cell receptor (ligands: PDL1 (B7-H1), PD-L2 (B7-DC)); reduces T cell proliferation and effector functions CTLA-4 (CD152) Cytotoxic T-Lymphocyte Antigen 4; inhibitory receptor (ligand: B7); effectively competes for ligands with CD28 (which has lower avidity than CTLA-4), preventing T cell activation Tim-3 T cell Immunoglobulin Mucin-3; inhibitory T cell receptor (ligand: galactin-9); leads to decrease in effector T cell function Chronic antigen exposure Adapted from Afanasiev, Nghiem, MCC book chapter T cell surface receptor phenotype reveals functional profile Activated cells, characterized by expression of: Acute antigen exposure T cell CD28 Co-stimulatory receptor (ligand: B7); required for T cell activation CD69 Earliest inducible cell surface glycoprotein during T cell activation; plays a role in T cell proliferation CD137 (41BB) Member of TNF-receptor family; induced by T cell activation; important in T cell proliferation, cytokine secretion and cytotoxicity CD38 Cyclic ADP ribose hydrolase; marker of T cell activation; functions in cell adhesion, signal transduction and calcium signaling HLA-DR MHC class-II surface receptor that is upregulated with T cell activation Recently activated T cells, characterized by expression of: Combination of activation and inhibition markers via appropriate immunoregulatory feedback mechanisms Exhausted T cells, characterized by prolonged expression of: PD-1 Programmed death-1; inhibitory T cell receptor (ligands: PDL1 (B7-H1), PD-L2 (B7-DC)); reduces T cell proliferation and effector functions CTLA-4 (CD152) Cytotoxic T-Lymphocyte Antigen 4; inhibitory receptor (ligand: B7); effectively competes for ligands with CD28 (which has lower avidity than CTLA-4), preventing T cell activation Tim-3 T cell Immunoglobulin Mucin-3; inhibitory T cell receptor (ligand: galactin-9); leads to decrease in effector T cell function Chronic antigen exposure Adapted from Afanasiev, Nghiem, MCC book chapter T cell surface receptor phenotype reveals functional profile Activated cells, characterized by expression of: Acute antigen exposure T cell CD28 Co-stimulatory receptor (ligand: B7); required for T cell activation CD69 Earliest inducible cell surface glycoprotein during T cell activation; plays a role in T cell proliferation CD137 (41BB) Member of TNF-receptor family; induced by T cell activation; important in T cell proliferation, cytokine secretion and cytotoxicity CD38 Cyclic ADP ribose hydrolase; marker of T cell activation; functions in cell adhesion, signal transduction and calcium signaling HLA-DR MHC class-II surface receptor that is upregulated with T cell activation Recently activated T cells, characterized by expression of: Combination of activation and inhibition markers via appropriate immunoregulatory feedback mechanisms Exhausted T cells, characterized by prolonged expression of: PD-1 Programmed death-1; inhibitory T cell receptor (ligands: PDL1 (B7-H1), PD-L2 (B7-DC)); reduces T cell proliferation and effector functions CTLA-4 (CD152) Cytotoxic T-Lymphocyte Antigen 4; inhibitory receptor (ligand: B7); effectively competes for ligands with CD28 (which has lower avidity than CTLA-4), preventing T cell activation Tim-3 T cell Immunoglobulin Mucin-3; inhibitory T cell receptor (ligand: galactin-9); leads to decrease in effector T cell function Chronic antigen exposure Adapted from Afanasiev, Nghiem, MCC book chapter Are the ‘brakes’ ON in MCC-specific T cells? (compared to other viral responses) PD-1 Tim-3 Examined ‘exhausted’ PD1+/Tim-3+ cells Are the ‘brakes’ ON in MCC-specific T cells? (compared to other viral responses) Tim-3 Examined ‘exhausted’ PD1+/Tim-3+ cells PD1+Tim3+ (%positive cells) PD-1 (Data from 4-7 MCC patients) Afanasiev et al, Clin Ca Research 2013 Are the ‘brakes’ ON in MCC-specific T cells? (compared to other viral responses) Tim-3 Examined ‘exhausted’ PD1+/Tim-3+ cells PD1+Tim3+ (%positive cells) PD-1 (Data from 4-7 MCC patients) Afanasiev et al, Clin Ca Research 2013 Are the ‘brakes’ ON in MCC-specific T cells? (compared to other viral responses) Tim-3 Examined ‘exhausted’ PD1+/Tim-3+ cells PD1+Tim3+ (%positive cells) PD-1 (Data from 4-7 MCC patients) Afanasiev et al, Clin Ca Research 2013 PD-1 & PDL-1 trials are beginning... MCC Clinical Trials Overview Clinical Trial Indication Target Patient characteristic Status IL-12 (Oncosec) Local Injection of IL12 gene Injectable lesion Complete GLA (Immune Design) Local Toll-like receptor agonist Injectable lesion Complete PD-1 (Merck) Metastatic 1st line PD-1 on T cell No prior systemic therapy Recruiting PD-L1 (EMD Serono) Metastatic 2nd line PD-L1 on Tumor Progressed after receiving chemo Recruiting T cell + PD-L1 (EMD + Pfizer) Metastatic Infuse Virus specific T cells Virus + MCC ? 4-1BB (Pfizer) Metastatic CD-137 on T cell +/- chemo or immune therapy closed PDL1 (2nd line) MCC trial: 55 yo woman; primary lesion on chest x 1 year (had metastases at dx) Failed chemotherapy (Carbo + etoposide) Large liver mets: 2 x 11 cm MCPyV-negative After 4 weeks (2 doses) of PDL1 Activity of PD-1 blockade with pembrolizumab as first systemic therapy in patients with advanced Merkel cell carcinoma European Cancer Congress / ESMO Vienna, Austria Sunday, September 27th, 2015 Paul Nghiem1,2, Shailender Bhatia1,2, Adil Daud3, Philip Friedlander4, Harriet Kluger5, Holbrook Kohrt6, Ragini Kudchadkar7, Evan Lipson8, Lisa Lundgren2, Kim Margolin6, Sunil Reddy6, Erica Shantha1, William Sharfman8, Elad Sharon9, John Thompson1,2, Suzanne Topalian8, Mac Cheever1,2 1) University of Washington 2) Fred Hutchinson Cancer Research Center 3) Univ of California San Francisco 4) Mt Sinai Medical Center 5) Yale University 6) Stanford University 7) Emory University 8) Johns Hopkins University 9) NCI-Cancer Therapy Evaluation Program Metastatic MCC platin + etoposide Initial responses common (53%) poor durability: >50% of patients progress by 3 months >90% of patients progress by 10 months Iyer, et al, J Clin Oncol 32:5s, 2014 (suppl; abstr 9091) Median survival = 9.6 months n = 179 Miller, et al, Curr Treat Options Onc, 2013 85 Trial design: pembrolizumab in MCC • Strong rationale for anti-PD1 in MCC – tumor-specific T cells are PD1+, Tim3+ – PDL1 frequent in MCC tumors • Multi-center (7 sites), single arm, open label, Phase II trial of first systemic therapy • Primary endpoint: response rate (RECIST 1.1) 86 Interim results 9/18/15 • 24 patients had received at least one dose of pembrolizumab • 14 patients had at least one post-treatment scan Response in MCC target lesions % Change in target lesions at 1st scan (At first scan, RECIST 1.1 as of 9/18/15 data export) Progression based on new lesions n = 14 * * Progressive disease: target lesion f/u data initially not available = Partial Response: 1st scan data initially not available, at 2nd scan was -70% = *Complete responses (RECIST 1.1) occurred in lymph nodes that regressed to < 10 mm. Activity of MK-3475 in patients with advanced MCC (RECIST 1.1 data as of 9/18/15) n = 14 includes 2 patients who have PD based only on new lesions (no f/u data on target lesions currently) Key: Progressive disease: target lesion f/u data not available = Progressive Disease = Stable Disease = Partial Response = Complete Response = *Complete responses (RECIST 1.1) occurred in lymph nodes that regressed to < 10 mm. Response to anti-PD1 Baseline: - Bulky tumors in pelvis: bladder compression - Subcutaneous metastases on R leg Baseline Response to anti-PD1 Baseline: - Bulky tumors in pelvis: bladder compression - Subcutaneous metastases on R leg Baseline 3 wks after pembrolizumab After 1 dose: - SQ lesion barely palpable at 3 weeks; biopsy showed. . . What happened in the SQ tumor? What happened in the SQ tumor? What happened in the SQ tumor? Pathologic CR after single dose of pembrolizumab Partial response on pembrolizumab Bulky pelvic disease: Baseline 1st scan (13 wks) after PD1 Bladder symptoms resolved Continues on trial (week 34) No side effects Tumors continue to shrink Partial response on pembrolizumab Bulky pelvic disease: Baseline 1st scan (13 wks) after PD1 Bladder symptoms resolved Continues on trial (week 34) No side effects Tumors continue to shrink Conclusions: Pembrolizumab in MCC • Responses (RECIST 1.1) in 10 of 14 patients (71%) – More durable than chemotherapy (historical) • Biomarker studies will address: – Virus-pos vs. virus-neg MCC responses? – Does PD-1 increase the number and/or function of preexisting virus-specific T cells in blood/tumor? (possible in 5 of 15 cases thus far) • Expansion plans underway...for first line & relapsed disease Vision for future MCC management 1. Minimize recurrences - best initial management (surgery, RT) - immune-stimulation in ‘adjuvant’ setting... Vision for future MCC management 1. Minimize recurrences - best initial management (surgery, RT) - immune-stimulation in ‘adjuvant’ setting... 2. If recurrence: - find early by serology or scans - reduce tumor & reverse immune evasion - immune-therapy for long-lasting control... Thanks to funding sources Michael Piepkorn Endowment Bezos Immune Therapy Fund Lab Team Jayasri Iyer Research fellows: Erica Shantha Candice Church Graduate and medical students/doctors: Ata Moshiri, Olga Afanasiev, Natalie Miller, Kelly Paulson, Natalie Vandeven UV & DNA repair Research scientists: Dafina Ibrani, Lola Yelistratova, Chris Lewis, Ryan Doumani Masaoki Kawasumi, Kaifeng Hung Undergraduate research assistants & students: Jamil Qazi, Hannah Thomas, Austin Anderson, Christine Ma, Kaushik P, Seesha T, Tessa Marx