Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart failure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Rheumatic fever wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Artificial heart valve wikipedia , lookup
Congenital heart defect wikipedia , lookup
Aortic stenosis wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
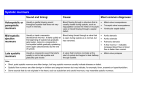
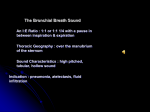
DIFFERENTIAL DIAGNOSIS OF HEART SOUNDS DIFFERENTIAL DIAGNOSIS OF HEART SOUNDS In clinical cardiology: Systole – period of ventricular contraction Diastole – period of ventricular relaxation What Is a Heart Murmur? These are abnormal sounds produced by turbulent blood flow in the heart caused by: Abnormal valve function: stenosis or regurgitation Increased volume or velocity of blood flowing through a normal valve such as during pregnancy, severe anemia, athletes Flow of blood through communications such as ASD, VSD Main signs Timing: systolic, diastolic or systolo- distolic Duration: e.g. pansystolic or late-systolic Site of maximum intensity Radiation Grading Character Relation with posture Relation with respiration Timing of murmur You need to be differentiated by palpating the carotid pulse during auscultation Systole starts with the first heart sound (coincides with the carotid pulse) and ends on second heart sound. Murmurs heard during this period are called systolic murmurs Diastole is the interval between second and first sound and it does not coincide with the carotid pulse. Murmurs heard during this period are called diastolic murmurs Duration of murmur б-protosystolic в-mid-systolic г-late-systolic (telesystolic) д-pansystolic е- golosystolic ж-presystolic з-protodiastolic и-systolo-diastolic Area of maximum intensity Murmur may be audible all over the precordium but the maximum intensity of murmur is heard where it originates Radiation Murmur radiate in the direction of blood flow to the specific sites from the precordium. Usually the systolic murmur radiates. When the area of maximum intensity has been noted, the stethoscope should be moved radically from this point in different directions to observe whether the murmur is localized or radiating to other of chest wall. Grading of systolic murmur Grade Grade 1/6 Feature Grade 3/6 So faint or soft that it is heard only with special effort Soft, but can be detected almost immediately by an experienced auscultator Prominent but not loud; no trill Grade 4/6 Loud; thrill just palpable Grade 5/6 Very loud; thrill easily palpable Grade 6/6 Very, very loud Grade 2/6 Grading of diastolic murmur Grade Feature Grade 1 Very soft (heard only in good circumstances) Grade 2 Soft Grade 3 Moderate Grade 4 Loud or associated with palpable thrill Dynamic maneuvers Relation with respiration: Murmurs of left side become louder during expiration and murmurs of right side become louder during inspiration. Relation with posture: Diastolic murmur of mitral stenosis is best heard in left lateral position while the diastolic murmur of aortic regurgitation is best heard when the patient sits and leaning forward. Dynamic maneuvers (2) Valsalva’s maneuver Listen over the left sternal border during the maneuver for changes in systolic murmur of hypertrofhic cardiomyopathy Functional (innocent) murmur These SM are produced due to change in velocity or viscosity of blood. These SM are present in the absence of heart abnormalities, disappear on exercise, do not radiate, thrill is never present and there is no change in the loudness of murmur with change of osture or respiration. Causes are: Anemia, polycytemia Fever Cirrhosis Thyrptoxicosis Hypertension Some common structural causes of systolic murmur Murmur Position where murmur is best heard Ejection (mid) systolic Aortic stenosis Pulmonary stenosis Atreal septal defect HOCM Aortic area Left sternal border Left sternal border II-III LIcostal Left sternal border Pan-systolic Mitral regurgitation Tricuspidal regurgitation Ventricular septal defect Apex Left sternal border Left sternal border III-IV L Icostal Some common structural causes of systolic murmur Murmur Position where murmur is best heard Late systolic HOCM Mitral valve prolapse Coarctation of aorta Accentuated on standing Apex Left sternal border Some common structural causes of dyiastolic murmur Murmur Position where murmur is best heard Mid-diastolic Mitral stenosis Tricuspid stenosis Apex , patient on left side, accentuated on exertion Left sternal border, accentuated on inspiration Austin-Flint murmur Apex Ealy diastolic Aortic regurgitation Left sternal border (III LIC, II aortic area and apex Right of sternum, louder on inspiration Pulmonary regurgitation Graham-Stell in pulmonary Left sternal border hypertention (due to MS) Some common structural causes of systolic murmur Murmur Position where murmur is best heard Combined systolic and diastolic Patent ductus arteriosus Left sternal edge Aortic stenosis and regurgitation Types of Murmurs Innocent (harmless) murmurs A person with an innocent murmur has a normal heart and usually has no other signs or symptoms of a heart problem. Innocent murmurs are common in healthy children. Abnormal murmurs A person with an abnormal murmur usually has other signs or symptoms of a heart problem. Most abnormal murmurs in children are due to congenital heart defects-heart defects present at birth. In adults, abnormal murmurs are most often due to heart valve problems caused by infection, disease, or aging. Types of Murmurs Innocent murmurs Normal heart murmurs Benign heart murmurs Functional heart murmurs Physiologic heart murmurs Still's murmur Flow murmur Abnormal murmurs Pathologic heart murmurs Innocent Heart Murmurs Innocent murmurs are heard when blood moves noisily through a normal heart. Sometimes these murmurs occur when: Blood is flowing faster than usual through the heart and blood vessels attached to the heart. An increased amount of blood is flowing through the heart. Illnesses or conditions that can cause blood to flow faster than usual through the heart include: Fever Anemia Too much thyroid hormone in the body (hyperthyroidism) Innocent murmurs are sometimes due to changes to the heart resulting from heart surgery or from aging. Abnormal Heart Murmurs The most common cause of abnormal murmurs is congenital heart defects. Congenital heart defects occur when the heart, heart valves, or blood vessels attached to the heart do not develop normally before a baby is born. Common defects that cause murmurs include: Congenital septal defects, which are holes in the wall (septum) that separates the right and left sides of the heart. They account for more than half of abnormal murmurs in children. Congenital valve defects, which include narrow valves that do not allow enough blood to flow through them and leaking valves that do not close properly. Abnormal Heart Murmurs Infections and other conditions that damage heart valves or other structures of the heart also may cause murmurs. Theses includes: Rheumatic fever, a serious illness that can develop after a person has an untreated or incompletely treated infection caused by the bacteria that cause strep throat or scarlet fever. Rheumatic fever can lead to permanent damage to the heart. If your doctor diagnoses strep throat, be sure your child takes all of the antibiotics prescribed, even if he or she feels better before the antibiotics run out. Endocarditis, an inflammation of the inner lining of the heart and valves that is usually caused by a bacterial infection. Endocarditis is a serious disease that can lead to permanent heart damage and other complications. Endocarditis usually occurs in an abnormal heart. Calcification (hardening and thickening) of valves as a result of aging. The hardened and thickened heart valves do not work as they should. PHYSIOLOGIC CLASSIFICATION OF SYSTOLIC MURMURS A. Systolic ejection murmurs-forward flow across the left or right ventricular outflow tract. B. Systolic regurgitate murmurs—regurgitates flow from a highpressure chamber to a lower-pressure chamber 1. Pansystolic regurgitant murmurs (mitral and tricuspid regurgitation, ventricular septal defect, left ventricle to right atrial defect) 2. Early systolic regurgitant murmur (acute mitral regurgitation, tricuspid regurgitation secondary to isolated disease of the valve, small ventricular septal defect) 3. Mid and late systolic regurgitant murmurs (papillary muscle dysfunction, mitral and tricuspid valve prolapse) PHYSIOLOGIC CLASSIFICATION OF DIASTOLIC MURMURS A. Diastolic filling murmurs (rumbles)- forward flow across the atrio-ventricular valves. 1. 2. Forward flow across a stenosed or obstructed atrioventricular valve (mitral or tricuspid stenosis, left or right atrial myxoma) High flow across a normal atrioventricular valve (mitral flow rumble of a ventricular septal defect or patent ductus arteriosus, tricuspid flow rumble of an atrial septal defect, hyperkinetic states, complete heart block) PHYSIOLOGIC CLASSIFICATION OF DIASTOLIC MURMURS 3. High flow across an incompetent atrio-ventricular valve without significant stenosis (flow rumble of mitral and tricuspid regurgitation) 4. Forward flow across a partially closed atrioventricular valve (presystolic murmur of mitral stenosis, Austin Flint murmur secondary to severe aortic or pulmonary regurgitation) 5. Combinations of 1 through 4 PHYSIOLOGIC CLASSIFICATION OF DIASTOLIC MURMURS B. Diastolic regurgitant murmurs—regurgitant flow across an incompetent semilunar valve: 1. Pandiastolic regurgitant murmurs (aortic regurgitation and pulmonic regurgitation secondary to pulmonary hypertension) 2. Abbreviated diastolic regurgitant murmurs (acute aortic regurgitation, minimal aortic regurgitation) 3. Delayed diastolic regurgitant murmur (organic pulmonic regurgitation) PHYSIOLOGIC CLASSIFICATIONS OF CONTINUOUS MURMURS A. Continuous murmurs caused by rapid blood flow 1. Venous hum 2. Mammary souffle 3. Hemiangioma 4. Hyperthyroidism 5. Acute alcoholic hepatitis 6. Hyperemia of neoplasm (hepatoma renal cell carcinoma, Paget's disease) PHYSIOLOGIC CLASSIFICATIONS OF CONTINUOUS MURMURS B. Continuous murmurs caused by high-to-low pressure shunts: 1.Systemic artery to pulmonary artery (patent ductus arteriosus, aortopulmonary window, truncus arteriosus, pulmonary atresia, anomalous left coronary, bronchiectasis, sequestration of the lung) 2. Systemic artery to right heart (ruptured sinus of Valsalva, coronary artery fistula) Left-to-right atrial shunting (Lutembacher's syndrome, mitral atresia plus atrial septal defect). 3. Venovenous shunts (anomalous pulmonary veins, portosystemic shunts)| 4. Arteriovenous fistula (systemic or pulmonic) What Are the Signs and Symptoms of Heart Murmurs? Most people with heart murmurs do not have any other signs and symptoms of a heart problem. The murmur is usually innocent (harmless). Some people with heart murmurs do have signs and symptoms of a heart problem. The signs and symptoms may include: Blue coloring of the skin, especially on the fingertips and inside the mouth Poor eating and failure to grow normally (in infants) Fast breathing Excessive sweating Chest pain Dizziness Shortness of breath Fainting Fatigue (feeling very tired) The signs and symptoms depend on the cause and the severity of the problem causing the murmur. How Are Heart Murmurs Diagnosed? Doctors use a stethoscope to listen to heart sounds and hear murmurs. They often notice innocent heart murmurs during routine checkups or physical exams. Physical Exam Doctors listen carefully to the heart with a stethoscope to help decide if a murmur is innocent or abnormal. They listen to the loudness, location, and timing of the murmur to classify and describe the sound. This helps the doctor begin to diagnose the cause of the murmur. How Are Heart Murmurs Diagnosed? The doctor also: Takes a medical and family history Does a complete physical exam, looking for signs of illness or physical problems (such as blue coloring of the skin, delayed growth, and feeding problems in an infant) Asks about symptoms, such as chest pain, shortness of breath (especially with exercise), dizziness, or fainting Tests Chest x-ray. A chest x ray takes a picture of your heart and lungs. It can show if the heart is enlarged, and it can show some problems of the heart and lungs. (С/Т)х100 (normal < 50%) Tests ECG. This test is used to measure the rate and regularity of your heartbeat. The EKG can help rule out a variety of heart problems. Will most likely do the followup testing. These tests might include: An echocardigram, a test that uses ultrasound (sound waves) to allow doctors to view your heart as it pumps and relaxes. The echocardiogram is more detailed than an x-ray image and shows the structure and function of the heart. In some cases, transesophageal echocardiography (TEE) might be needed to get a better view of the heart. In TEE, the doctor inserts an ultrasound probe down the throat into the esophagus after the patient is sedated. Tests Cardiac catheterization and angiography. Cardiac catheterization is a procedure in which a thin, flexible tube (catheter) is passed through an artery or vein in your upper thigh (groin) or in your arm to reach the heart, after you are sedated. This allows measurement of pressure inside the heart and blood vessels. Angiography involves injecting a dye that can be seen by using x ray. This helps the doctor see the flow of blood through the heart and blood vessels. Mitral Regurgitation (MR) Chronic MR Rheumatic heart disease (50%) Mitral valve prolapse Disease that cause dilatation of left ventricle cavity cause dilatation of valve annulus and mild MR (called functional MR), such disease are: Aortic valve disease Acute rheumatic fever Myocarditis Dilated cardiomyopathy Ischemic heart disease Acute MR Myocardial infarction (due rupture of chordae tendineae) Infective endocarditis Sign Aetiology Morphology Organic MR Rheumatism, Atherosclerosis, Connective Tissue diseases Valve change 1 heart sound Concerned connectivity Loudness murmur noise loud MR Myocarditis EH Cardiosclerosis Valve non change Non concerned low, faint Depending on Noise constant, position of body auscultate in any position of body Noise non constant, disappear at change on position of body Duration Pan systolic or 2/3part short, 1/3 – ½ of systole Dependence of breath phases Become louder during expiration Weakens or disappears during expiration On the left side Radiating Becomes stronger Widely over the precardium, axilla soft May disappear Apex 1 heart sound No change Innocent Systolic Murmurs Pansystolic murmur Sign Organic MR Common Systolic murmur at apex, I heart sound low, faint Aetiology Rheumatism, Atherosclerosis, Connective Tissue diseases Complaints breathlessness, heart pain, palpitation S1 Connectivity Concerned Mitral valve Prolapse (MVP) Genetic disease, Marfan syndrome, Connective Tissue diseases Most patients are asymptomatic breathlessness, heart pain, palpitation Non concerned Duration SM Pan-systolic Late-systolic Irradiation Apex to axilla Apex Depending on Noise constant, position of body auscultate in any position of body weakens, disappears at change on position of body Exertion Become louder during expiration Weakens Additional heart tones No additional tones Mid systolic click is present ECHO Valve structure is changed Mitral valve Prolapse MVP Pan-systolic M at the MR Mid-systolic clik and late systolic M at the MVP Late systolic M at the MVP Sign Organic MR Aortic Stenosis Common Pan Systolic murmur, loud, harsh S1 Change Normal or soft S2 Ascent on 2 lIC Soft only P2 is audible Localization Apex 2 right IC, point Erba Depending on position of body Noise constant, auscultate On the right side, in any position of body sitting while bending ahead Irradiation Apex to axilla To the carotid artery, precardium to the apex Phonocardiogram Pansystolic. Ribbon like Mid-systolic. Rhombus like Systolic vibration absent present ECHO Left atrial cavity increase, Left ventricular mitral valve changes cavity increase, aortic valve changes ECG LAH, LVH LVH Aortic stenosis- M ECHO Aortic stenosis- B ECHO Sign Aortic Stenosis Ventricular septal defect Common Systolic murmur, loud, harsh, increasing Localization 2 right IC, point Erba III-IV left IC Depending on On the right side, sitting position of body while bending ahead Independent Examination Apex beat is strong Hump Palpation Systolic vibration in jugular fossa ECG ECHO LVH Left ventricular cavity increase, aortic valve changes Left sternal boader and epigastria pulsation RVH Interventricular septal defect Sign Aortic Stenosis Atrial septal defect Common Systolic murmur, loud, harsh, increasing Localization 2 right IC and point Erba II left IC Depending on position of body On the right side, sitting while bending ahead Independent Examination Apex beat is strong Hump Palpation Systolic vibration in jugular fossa Pericardial and epigastria pulsation ECG ECHO LVH Left ventricular cavity increase, aortic valve changes RVH, RAH Atrial septal defect Sign Aortic Stenosis Common Systolic murmur, loud, harsh at point Erba, Irradiation clavicles, jugular fossa Aetiology Rheumatism, Unaware, hereditary factor Atherosclerosis, syphilis, бактериальный infective endocarditis, congenital anomaly of valves and aortic I sound weakening I sound non change or intensification Ausculta tion Connection Not connected with heart with I sound sounds HOCMP Not connected with heart sounds Sign Aortic Stenosis HOCMP Irradiation Irradiation clavicles, jugular fossa Not irradiation clavicles, jugular fossa Depending on position of body Noise constant, auscultate Murmur increases at test Val in any position of body, salve non disappear after body position change ECG LVH Q wave in V1-6, deep, narrow ECHO Valve structure is changed Thickness of IVS is >1 cм (2-3см), LV cavity is decreased X-ray Aorta is enlarged in ascending aortic part, strong pulsation Little or not presence of heart shadow enlargement Middle valve aortic stenosis IVSD- early systolic murmur IVSD- pan systolic murmur ASD- loud, tricuspid component of I sound and II sound splitting Differential diastolic murmurs description organic functional Aetiology mitral or tricuspid stenosis, left or right atrial myxoma, ductus arteriosus functional tricuspid stenosis, atrial septal defect Loudness loud low Duration Depending on position of body long Noise constant, auscultate in any position of body Diastolic filling murmurs short weakens, disappears at change on position of body Diastolic regurgitate murmurs Mechanism Proto diastolic murmurs S1 S2 S1 S2 S1 Presystolic and pandiastolic murmurs Mitral stenosis (МS) Signs Aortic insufficiency (AI) Types of DM Relationship with II sound True proto diastolic Different types of DM Starts immediately with Starts some time from II II sound sound (after QS – sound) Duration Timbre Prolonged Soft, quiet III – IV i/c place at left side Body position Vertical position II sound II sound in aortic zone is decreased, II sound in pulmonary zone is not changed Localization Short Rather harsh Apex of heart Horizontal position II sound in aortic zone is not changed, II sound in pulmonary zone is increased Signs АI МS I sound Is not changed or weakened Flapping I sound Extra sound Pre systolic murmur of Astine-Flint OS sound ECG RVH RAH and RVH ECHO Aortic valve changes, Mitral valve changes, aortic regurgitation, LV area of mitral aperture cavity increases decreases, LA and RV increase АR МS Signs Common Aetiology Mitral stenosis Myxoma of left atrial (МS) I sound increased, can be present in III sound at QS zone, diastolic murmur Reumatism Tumor cause is unknown Auscultation OS sound appears in 0,06-0,12 sec after II sound III extra sound can present but appears later than in 0,12 sec after II sound Types of DM Often pre systolic Often mid systolic, seldom pre systolic Sound stability Murmur is stable, can be heard at intake and at body position on the left side Murmur is unstable, can be heard at sitting and standing position, sometimes disappears when position is changed ECHO Valve is changed Valve is not changed, tumor is present in left atrial Signs МS Common DM - left side of sternum, epigastria and pre cardiac pulsation, accent II sound at pulmonary artery, heart boundaries enlarge to the right тона Reumatism COPD Aetiology Auscultation Types of DM Sound stability OS sound appears in 0,06-0,12 sec after II sound Often pre systolic Cor Pulmonale Dull heart sounds Proto diastolic (GrahamStill) Murmur is stable, can Murmur is unstable, can be heard at intake and at disappear after treatment body position on the left side Signs МS Cor Pulmonale Dependence on breath phases Can be heard on outward breath Can be heard at intake and breath delay at standing ECG LAH and RVH RAH and RVH ECHO Mitral valve is changed, Mitral valve is not LA and RV increased changed, pulmonary artery is enlarged, pulmonary regurgitation, RA and RV increased X-ray LA is increased, mitral heart configuration Bulging of truncus pulmonary artery, signs of main disease are present DIFFERENTIAL DIAGNOSIS OF HEART SOUNDS DIFFERENTIAL DIAGNOSIS OF HEART SOUNDS CONDITION EXPIRATION INSPIRATION NOTES VARIATIONS OF REGURGITANT MURMURS DIASTOLIC FILLING MURMUR (RUMBLE OF MITRAL STENOSIS)