Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
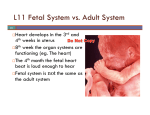
As Overview of Fetal Circulation Rima Bader MD ,PhD, FASE, FACC Professor of Pediatrics, Consultany Pediatric &Perinatal cardiology King Abdul Aziz University College of medicine Jeddah, Saudi Arabia Flow Chart of Fetal Circulation Fetal Circulation By the third month of development, all major blood vessels are present and functioning. Fetus must have blood flow to placenta. Resistance to blood flow is high in lungs. Umbilical Circulation Pair of umbilical arteries carry deoxygenated blood & wastes to placenta. Umbilical vein carries oxygenated blood and nutrients from the placenta. Overview of the Fetal circulation Blood is oxygenated in the placenta Oxygenated blood returns to the fetus via the umbilical vein Umbilical vein courses into the hilum of the liver and joins the portal vein Umbilical venous blood is directed in part through the ductus venosus which joins the IVC O2 rich ductus venosus blood is preferentially directed into the left atrium and left heart through the foramen ovale Venous return of the left heart is comprised of both ductus venosus and pulmonary venous blood less oxygenated blood of the liver (largely right lobe) and the SVC is directed into the right atrium and right heart The left and right hearts function in parallel rather than in series . The left ventricle ejects largely to the coronary arteries and upper body with an arterial PaO2 (in fetal lambs) of 25-28mmHg. The right ventricle ejects largely to the lungs, the lower body and the umbilical artery via the ductus arteriosus with an arterial PaO2 of 20-23mmHg (in fetal lambs) With a high pulmonary vascular resistance, less than 20% of the cardiac output goes through the fetal lungs with an increase in the third trimester The combined cardiac output of the fetal heart is 450cc/kg/min with mild RV dominance through the second and third trimesters in contrast to the 800cc/kg/min of the combined output that occurs in the in series circulation The Placenta Facilitates gas and nutrient exchange between maternal and fetal blood. The blood itself does not mix. The placenta Comprised of maternal (utero-placental) and fetal (feto-placental) components Provides nutrients, respiratory gas and metabolic exchange between the mother and fetus Placental development begins at implantation with attachment and invasion of trophoblast cells into the uterine mucosa (6-7 days post conception) Complete fetoplacental circulation is established around the start of the 5th week post conception Uteroplacental flow increases during gestation in 3 phases as a result of vasodilation: first of which may occur within days or weeks of pregnancy, second with development of intravillous spaces, third during rapid fetal growth after 30 weeks and this corresponds with a change in uterine blood flow from <1% of the maternal cardiac output to 16-25% near term. Fetoplacental blood flow also exponentially increases throughout gestation which is likely the consequence of both vasodilation and vascular growth and may be an index of fetal growth. Placental blood volume is approximately 30% of the combined fetal cardiac output in this same period. Clinically, umbilical artery Doppler flow studies have demonstrated evidence of a gestational-age dependent fall in placental resistance with essentially no forward diastolic flow in the late first trimester to increasing flow velocities in diastole through the second and third trimesters The fetal shunts 1. Ductus venosus Provides access for much of the highly oxygenated blood from the umbilical vein to the fetal inferior vena cava This streams preferentially into the left atrium as a consequence of the IVC’s central position and relationship with the foramen ovale, septum primum and septum secundum. Ductus Venosus . In its absence (also known as agenesis of the ductus venosus) the umbilical vein may connect with the portal venous system, another systemic vein such as the inferior vena cava or the right atrium itself. . Observations of changes in ductus venosus patterns in the context of evolving fetal heart failure with gradual reduction in forward velocities during atrial systole in the ductus venosus with ultimate development of a wave reversal that occurs before the development of umbilical venous notching This could also suggest a protective mechanism that prevents modestly elevated central venous pressures from significantly influencing the critical umbilical venous return Lets go! 2- Foramen ovale Blood is shunted from right atrium to left atrium, skipping the lungs. More than one-third of blood takes this route. Is a valve with two flaps that prevent backflow. Foramen ovale ( cont’d) a communication between the left and right atrium with a flap-valve (septum primum) that allows the oxygen rich blood of streaming through the ductus venosus from the umbilical vein to enter into the left atrium . Septum primum serves to prevent blood flow from moving from the left atrium to the right atrium In humans Doppler studies suggest the proportion of combined cardiac output that crosses the foramen goes from 34% at 20 weeks to 18% at term. 3- Ductus Arteriousus The blood pumped from the right ventricle enters the pulmonary trunk. Most of this blood is shunted into the aortic arch through the ductus arteriousus. 3- Ductus Arteriosus The ductus arteriosus is a vessel that permits the majority of the right ventricular output to be ejected into the descending aorta. Early in gestation its size is very similar to that of the aortic arch Later in gestation, however, likely in preparation for postnatal closure, intimal cushions form within its lumen as a result of vascular smooth muscle cell proliferation and migration into the subendothelium. The formation of intimal cushions could correspond with the very high velocities observed in the ductus arteriosus of late third trimester human fetuses Circulating PGE2 probably controls the patency of the ductus arteriosus in utero 4- Aortic Isthmus While not a true fetal shunt, The aortic isthmus acts somewhat as a watershed between the aortic arch and ductus arteriosus-descending aorta which reflects differences in vascular impedance between the cerebral vascular bed and the lower body and placenta The Fetal Myocardium A- Developmental changes in structure/growth: knowledge of the developmental changes that occur in the fetal heart are important in understanding the fetal circulation Fetal myocardial growth–in the fetus particularly early in gestation, is largely through cardiac myocyte and nonmyocyte proliferation Rapid myocardial growth and general somatic occurs in fetal life, particularly in the first half of gestation after embryogenesis B-Developmental Changes in Myocardial Function Systolic function echocardiographic parameters of systolic performance are not so different in the fetus versus the postnatal heart normal dP/dt max 1500-3000mmHg/s LV and RV shortening fraction is 30-34% and does not change with age LV ejection fraction is 60-65% in the fetus and postnatally cardiac output changes from 450ml/kg/min in utero to 800ml/kg/min for the combined ventricular output. In utero the RV output is approximately 1.2-1.4 that of the LV Diastolic function Changes with gestational age and postnatallysingle muscle strip preparations suggest greater passive tension of the fetal myocardium Ventricular Doppler filling patterns demonstrate increasing e wave (early ventricular diastole) with gestation and no change in the a wave velocity (during atrial systole) which suggests changes in the ability of the ventricles to relax with gestation Isvolumic relaxation time does not significantly change between the second and third trimesters Preload Fetal myocardium does follow Frank-Starling rules as is most simply demonstrated by the increased ventricular output following a premature beat Left ventricular (LV) preload is determined by inferior vena cava flow, pulmonary venous return, size of the foramen ovale, right heart filling pressures, in the right atrium, the diastolic or filling function of the left ventricle Right ventricular (RV) preload is determined by the superior and inferior vena caval flow left heart filling pressure foramen ovale size and right ventricular diastolic function Afterload left ventricular afterload is largely from the upper body right ventricular afterload is largely determined by the vascular bed of the lower body (including the placenta) and patency of the ductus arteriosus afterload has a significant impact on cardiac output the low vascular impedance of a normal placenta results in a large proportion of the combined ventricular output to go through the umbilical circulation at midgestation 50% of the total fetal blood volume is contained within the placenta, however this decreases to about 33% by term Heart rate normal fetal heart rates range 110-150bpm at less than 10 weeks, from 150-180bpm at 10-16 weeks 120-160bpm from 20 weeks to term over the normal range of heart rates, the human fetus does not significantly change the cardiac output but rather changes stroke volume to maintain a stable cardiac output What happens at birth? The change from fetal to postnatal circulation happens very quickly. Changes are initiated by baby’s first breath. Foramen ovale Ductus venosus Closes shortly after birth, fuses completely in first year. Closes soon after birth, becomes ligamentum arteriousum in about 3 months. Ligamentum venosum Umbilical arteries Medial umbilical ligaments Umbilical vein Ligamentum teres Ductus arteriousus Problem with persistence of fetal circulation Patent (open) ductus arteriosus and patent foramen ovale each characterize about 8% of congenital heart defects. Both cause a mixing of oxygen-rich and oxygenpoor blood; blood reaching tissues not fully oxygenated. Can cause cyanosis. Transcatheter closure or surgical correction now available, ideally completed around age two. Many of these defects go undetected until child is at least school age. Take home message 1. Fetal left and right hearts function in parallel 2. rather than in series and this is a result of the unique fetal shunts and placental circulation As a consequence of the fetal circulation and streaming of blood, the left heart in utero sees more highly oxygenated blood which goes to the fetal myocardium and brain 3. Normal fetal heart rates range from 110150bpm at less than 10 weeks, from 150180bpm at 10-16 weeks and 120-160bpm from 20 weeks to term 4. There are key developmental differences between the fetal, neonatal and adult myocardium that result in differences in diastolic and systolic function The fetal myocardium does follow Frank-Starling rules as is most simply demonstrated by the increased ventricular output following a premature beat The fetal response to stress includes increase in the mean arterial pressure, decrease in the fetal heart rate, late in the course decrease in the combined cardiac output and redistribution of the cardiac output to critical organs: the brain, heart, adrenal glands. Thank you!