Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
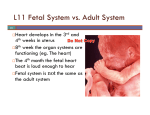
Physiological Problems of the Fetus and Placenta Immune Attack • Why isn’t the fetus rejected by the mother’s immune system? • Hypothesis 1: uterus is a special immunologically safe place. But, ectopic pregnancies can occur and succeed. • Hypothesis 2: the placenta is able to protect the fetus from antibody-mediated attack by restricting passage of fetal antigens into the mother’s body and maternal antibodies into the fetal circulation. Yes, but how about Rh disease, in which Rh- mother can develop antibodies to Rh+ fetus and cause miscarriage? • With contemporary methods, it has been shown that mothers are invaded by small numbers of fetal cells in each pregnancy and these cells may survive in mother’s body for extended periods. Consequences – bad: autoimmune disease – good: mother makes a better tissue donor for her children. Gas Exchange Between Mother and Fetus • Oxygen: PO2 of maternal blood in placental blood sinuses is about 30-35 mmHg. PO2 of fetal blood in umbilical vein is about 30 mmHg. So, fetal blood must load O2 at a considerably lower PO2 and with a considerably smaller gradient than adult blood. • A partial solution is provided by fetal Hb, which consists of 2 α chains and 2 γ chains rather than 2 α chains and 2 β chains, and is left-shifted relative to adult Hb. This gives about 85% saturation for blood in the umbilical vein. Also, the fetal blood has an O2 carrying capacity about 50% higher than maternal blood. • CO2: the gradient between maternal and fetal blood is only 5 mmHg, so CO2 transport is about half as efficient as in the adult lung. • This crummy situation is the result of the truly goofy design of the reproductive physiology of placental mammals. Roadmap of fetal-placental circulation Umbilical vein (80% sat) Placenta Umbilical arteries (58% sat) Ductus venosus Fetal Body Left Heart Ductus arteriosus Green connections will be eliminated at birth Lower body venous blood (27% sat) Vena cava (67% sat) Lungs Right Heart Foramen ovale Placental venous blood joins the fetal circulation via the ductus venosus in the liver The numbers show the percentage of fetal cardiac output that passes each checkpoint. Note that about half of the fetus’ cardiac output goes to the fetal body and the other half to the placenta. At the junction of ductus venosus and inferior vena cava, venous blood from the fetal body mixes with relatively oxygenated umbilical cord blood. Two anatomical shunts – the ductus arteriosus and the foramen ovale - allow most of the right heart’s output to bypass the pulmonary loop Summary of blood oxygenation levels in the fetal circulation • Lungs are collapsed, so pulmonary loop R is high; with placenta in place and little sympathetic outflow, systemic loop R is low. • A R to L shunt operates via ductus arteriosus and foramen ovale • Fetal vena cava blood is a mixture of 80% saturated blood from placenta and 27% saturated blood from fetal lower body, so when the two bloods mix at the right atrium, the Hb saturation is about 67%. • About ½ of fetal cardiac output flows to the placenta. Circulatory Changes at Birth • Lungs inflate: ventilation stimulated by cold, asphyxia; pulmonary arterioles dilate, pulmonary resistance falls • Systemic loop resistance rises: large sympathetic outflow during birth, removal of placenta • Foramen ovale closes: swinging door effect • Ductus venosus closes: ? • Ductus arteriosus closes: prostaglandin involved • Umbilical vessels close: probably several factors involved. Note that the umbilical vein is still available for intravenous drug delivery in adults. What would the consequences be if one of these events didn’t happen? Birth Stresses and Responses in the Neonate • What are the stresses? – Hypoxia – Need to start thermoregulating – Need to inflate lungs and start breathing – Pressure – especially on the head during vaginal birth Central Role of Adrenal Catecholamines • Large surge of catecholamine is released during birth – levels in blood can reach 50 nM – about 6X higher than in exercising adults. If asphyxia occurs, the concentration can reach 200 nM. • Effects: – Breathing: dilates bronchioles, increases pulmonary surfactant secretion, promotes fluid absorption – Vascular: peripheral vasoconstriction; MAP increases; increased pressure in systemic loop closes foramen ovale. – Metabolic: mobilizes glucose; stimulates heat production by brown fat – CNS: promotes alertness Brown fat provides heat for the brain and thorax for several months after birth • Unlike white fat, brown fat contains a high density of mitochondria • An uncoupling factor (a H+ channel) is expressed in response to T3 • The uncoupling factor is activated in response to epinephrine • Uncoupled mitochondria convert almost all of the energy of fat catabolism to heat rather than phosphorylation potential. • True hibernators retain brown fat for rewarming in the spring • We now know that adult humans have some brown fat Vaginal birth is usually better • Caesarian-delivered babies don’t get the beneficial effects of sympathetic activation • Caesarian rate is 15-20% of deliveries – roughly 50% of unplanned Caesareans seem to be unnecessary • In evaluating the extent of fetal distress in a difficult labor, it is best to measure the pH of scalp blood (<7.25 indicates asphxia), rather than make decision on basis of fetal heart monitor.