Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Lutembacher's syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Echocardiography wikipedia , lookup
Jatene procedure wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
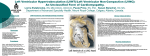
56 © JAPI • may 2012 • VOL. 60 Case Report Isolated Non-Compacted Right Ventricular Myocardium Monika Maheshwari*, RK Gokroo**, SK Kaushik*** Abstract Ventricular non-compaction or spongy myocardium is a rare type of cardiomyopathy resulting from arrested myocardial development during embryogenesis. This rare entity is characterized by excessive prominent trabeculations and deep inter-trabecular recesses in the ventricular wall. The clinical manifestations include heart failure, arrhythmias and cardioembolic events. The usual site of involvement is the left ventricle. Rarely the right ventricle (RV) is affected. Here we report a case of 40 year old male patient presenting with isolated RV non–compaction. W Introduction orld Health Organisation /International and Federation of Cardiology Task Force in 1995 categorised noncompacted ventricular myocardium (NCVM) as an ‘unclassified cardiomyopathy’.1 It has an estimated prevalence of 0.05% in adults and 0.14% in pediatric population with a male to female ratio of 5.7 to 1.2 The usual site of involvement is the left ventricle. Involvement of both ventricles or isolated non-compaction of RV has been described rarely.3-5 Hence it was worth reporting this unusual entity. Case – Report A 40 year male presented in emergency department with complains of exertional dyspnoea, palpitation and swelling over both lower extremities and abdomen since 1 month. On examination he was afebrile with pulse 102/minute regular, blood pressure-110/70 mmHg and respiratory rate-20/minute. There was pallor, bilateral pitting edema over lower extremities and raised jugular venous pressure 6 cm above sternal angle with a prominent ‘v’ wave. There was no cyanosis, clubbing, icterus or lymphadenopathy. On cardiac auscultation there was loud P2, prominent S3 gallop with a grade 3/6 systolic murmur at left lower sternum. His lung fields were clear. Chest Xray demonstrated cardiomegaly. Cardiac enzymes and electrocardiogram were normal. However, 2D transthorasic echocardiogram revealed spongy RV myocardium with heavy trabeculations and deep intertrabecular recesses prominent at the RV apex and free wall diagnostic for non-compaction. Left ventricle was normal. (Figures l and 2) The patient was treated with angiotensin– converting enzyme inhibitors, thiazide diuretics, aldosterone antagonist and warfarin and was discharged with symptomatic relief after 7 days. Discussion Myocardial non-compaction is a rare disorder with uncertain etiology.6 Both familial and sporadic forms of NCVM have been described. The diagnostic criteria for NCVM have been described as follows: 1. The absence of co - existing cardiac anomalies 2. A two layered structure of the ventricular wall,with end-systolic ratio of the non-compacted to compacted myocardial layer >2 3. Finding this structural abnormality predominantly in the apical and midventricular areas. Fig. 1 : Trans thoracic echocardiogram showing trabeculations and deep intertrabecular recesses prominent at the RV apex and free wall. Resident, ** Professor, *** Professor and HOD, Department of Cardiology, J.L.N. Hospital, Ajmer. Received: 08.04.2011; Accepted: 03.06.2011 * Fig. 2 : Trans thoracic echocardiogram showing trabeculations and deep intertrabecular recesses prominent at the RV apex and free wall. © JAPI • may 2012 • VOL. 60 4. The blood flow directly from the ventricular cavity into deep inter-trabecular recesses. Normally during 5 to 8 gestational weeks compaction of the developing myocardium occurs along with the commencement of coronary circulation in the myocardium; during compaction the recesses in the trabecular network are reduced to capillaries. Arrest in endocardial morphogenesis and failure of regression of embryonic ventricular sinusoids results in non compaction.7 However the exact etiology still remains unknown. Morbidity and mortality is substantial at an early age with five year survival less than 50%. The main complications are heart failure, arrhythmias and embolism. Endomyocardial morphology in NCVM is responsible for the development of mural thrombi within the inter-trabecular spaces. All adult patients are recommended oral anticoagulation irrespective of ventricular functions.8 Perhaps the most controversial management option is ICD implantation. Although studies demonstrating potential benefit of ICD implantation has not been performed, it seems intuitive that these devices may protect patients from sudden cardiac death. References 1. 57 Richardson P, Mckenna W, Bristow M, Maisch B, Mautner B, O’Connel J,Olsen E,Thienne G,Goodwin J et al. Report of the 1995 World Health Organisation/International Society and Federation Of Cardiology Task Force on the definition and classification of cardiomyopathy. Circulation 1996;93:841-2. 2. Dass B,Jusszczyk MA,Hoggman D,Young. Isolated non-compaction of the ventricular myocardium. Hospital Physician 2008;39-41. 3.Yuksel C, Necmi A, Bilgin T Bulent G, Omer G, Gulmira K, Ahmet U. Noncompaction of the ventricular myocardium : report of two cases with bicuspid aortic valve demonstrating poor prognosis and with prominent right ventricular involvement. Echocardiography 2003;20:379. 4. Ying ZQ, Xu G, Chen S, Ma J, You XD. Cerebral infarction in an adult patient with right ventricular hyper-trabeculation / noncompaction. Int J Cardiol 2008;127:150-51. 5. Ying ZQ,Ma J,Chen S,Xu G,Chen MY,You XD.Biventricular pacemaker implantation in a patient with isolated non-compaction of the right ventricular myocardium. Int J Cardiol 2008;131:14-16 6. Gomathi SB, Makadia N, Ajit SM. An usual case of isolated noncompacted right ventricular myocardium. European Journal of Echocardiography 2008;9:424-25. 7. Reynen K, Bachmann K, Singer H. Spongy Myocardium. Cardiology 1997;88:601-2. 8. Oeschslin E,Attenhofer C,Rohas J,Kauffmann P,Jenni R. Long term follow up of 34 adults with isolated left ventricular noncompaction :a distinct cardiomyopathy with poor prognosis. J AmColl Cardiol 2000;36;493-500.