Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Aortic stenosis wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Atrial fibrillation wikipedia , lookup
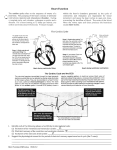
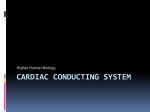
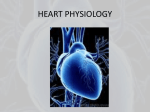
B io Factsheet www.curriculum-press.co.uk Number 234 Electrocardiograms (ECGs) Exam questions frequently ask candidates to explain electrical activity (and blood pressure changes) during the cardiac cycle. This Factsheet: • Summarises the electrical activity of the cardiac cycle • Describes how electrocardiogram (ECG) traces can be used to identify heart defects • Illustrates common exam questions on this topic What happens during a heart beat? Fig. 1 shows the pathway of electrical activity through the heart . aorta LA = Left Atrium LV = Left Ventricle RA = Right Atrium RV = Right Ventricle sino-atrial node (SAN/ pacemaker) in wall of right atrium 2 2 LA 1 bundle of His 3 2 4 5 LV RA artri-ventricular node (AVN) in the atrioventricular septum 1. wave of excitation that starts each heart beat is sent from the SAN 2. spreads over atrial walls causing contraction 3. delayed at non-conducting atrioventricular septum 4. wave of excitation is sent from AVN 5. passes along bundles of His/Purkine fibres to the base of the ventricles which then contract 6. before spreads over the walls of the ventricles causing them to contract Purkine fibres 6 RV 6 5 5 intraventricular septum Typical Exam Question Read through all of the following passage and then fill in the spaces with the most appropriate word or words. The cardiac cycle is initiated and controlled by the heart itself. Cardiac muscle is said to be ......................... since it will contract and relax of its own accord. The beat is initiated by the .........................which is situated in the wall of the ............... Waves of depolarisation travel through the atria causing atrial .............. The waves of depolarisation can only travel to the ventricles via the ................... situated at the top of the ventricular septum. From here the waves travel to the apex of the heart through the ..................... which is made of specialised conducting cells called ........................... These then carry the waves of depolarisation through the ventricle walls causing both ventricles to contract simultaneously. At this stage the ..................... are open and the ........................... are shut so that blood can be forced into the arches. myogenic; sinoatrial node/pacemaker; right atrium; systole/contraction; atrioventricular node; bundle of His/left + rightbundle branches; Purkinje fibres; semilunar valves; atrioventricular valves; Markscheme Extract from Chief Examiner’s Markscheme A surprising number of candidates were confused about the roles of the SAN, AVN and bundle of His. Many thought that the only role of the SAN was to relay impulses from the CNS. Few candidates realized that the AVN produces the electrical activity that causes the ventricles to contract and a quarter of the candidates thought that the bundle of His was responsible for the contraction of the ventricles from their bases. 1 Bio Factsheet 234. Electrocardiograms (ECGs) www.curriculum-press.co.uk Electrocardiograms (ECGs) Extract from Chief Examiner’s Markscheme Few candidates realised that ECGs shows electrical activity rather than blood flow. Only about half the candidates knew that the P wave corresponded to electrical activity prior to atrial systole and that the QRS corresponded to electrical activity prior to ventricular systole. ECGs are a record of the electrical currents that cause the heart muscle to contract. Electrodes placed on the skin detect the electrical activity. Electrode jelly ensures good electrical contact and the patient is required to keep still because movement causes interference to the trace due to the electrical impulses from the muscles (Fig 2). Fig. 2 Typical ECG for a normal cardiac cycle Key P: atrial systole (contraction) the wave of depolarisation in the walls of the atria i.e. atrial systole. The atria contract and blood flows into the ventricles. The heart rate can be calculated from the interval between successive P waves R electrical potential /mV QRS: ventricular systole (contraction) the wave of depolarisation in the walls of the ventricles i.e. ventricular systole. The ventricles contract and the valve between atrium and ventricle closes T P Q T : ventricular diastole The ventricles relax • The PR interval = the time taken for an electrical impulse to travel from the atria to the ventricles S 0 0.2 0.4 time (s) 0.6 0.8 • The QT interval = the contraction time because the ventricles are contracting • The interval between T of one cardiac cycle and Q of the following cycle = the filling time because blood is firstly filling the atria, then the ventricles Fig. 3 shows an abnormal ECG trace from a patient who has suffered a heart block. The ECG trace shows a much longer than normal time interval between the P and R waves. This could be a result of damage to the Purkine tissue or improper functioning of the AV node. Atrial fibrillation causes blood flow to slow down and it may even stop. This can cause ‘pooling’ of the blood in certain places in the circulatory system. Fig.3 ECG of patient with heart block Fig.5 shows an ECG trace from a patient suffering tachycardia in which the heart beat much faster than normal - exceeding 100bpm even when the patient is at rest. Greater voltages are also generated. Fig. 5 ECG showing tachycardia 1 mv 1 sec Fig.4 shows an abnormal ECG trace from a patient suffering who has suffered ventricular fibrillation caused either by an acute heart attack or electrical shock. Fig. 4 ECG showing ventricular fibrillation Typical Exam Question Suggest what effects tachycardia could have on cardiac output. Cardiac output could increase if ventricles have time to fill sufficiently; But it could decrease if there was insufficient time to fill the ventricles between contractions; Net effect depends on whether the decrease in stroke volume is compensated by the increase in heart rate; Markscheme 2 Bio Factsheet 234. Electrocardiograms (ECGs) www.curriculum-press.co.uk Fig.6 shows an ECG trace from a patient suffering from hypothermia – the heart beat is much slower than normal but retains the shape of that of a normal individual However, because even patients with heart disease can display a normal ECG trace modifications of the ECG procedure are routinely used: Fig.6 ECG trace showing hypothermia 1. 24 hour ‘ambulatory’ monitoring of the ECG. The patient wears the heart monitor and takes readings about every 20 minutes. The data are stored and the patient keeps a diary of how they are feeling, enabling feelings of breathlessness etc to be linked to changes in their ECG trace. 0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 2. Exercise tolerance test or stress test The ECG electrodes are attached to the patient who then walks on a slowly – moving treadmill set at a slight incline. Both the incline and the speed of the treadmill incline are gradually increased so that the patient’s heart rate increases. 1.8 Typical Exam Question (a) The electrocardiogram (ECG) trace below was recorded over a period of 5 seconds from a healthy person. Exam Hint:- Do not confuse electrical activity with blood flow. ECGs show electrical activity, NOT blood flow Fig.7 shows an ECG trace from a patient suffering from a damaged AVN. Because it is the AVN that produces electrical activity, there is a much lower spike and the low AVN spike results in less electrical activity in the rest of the heart. Fig. 7 ECG comparing healthy heart to one with damaged AVN Count the number of complete cardiac cycles, and then calculate the heart rate in beats per minute (2). (b) The following ECG trace was taken from a different person. healthy damaged AVN Identify one irregularity shown in the trace (1). Typical Exam Question The diagram shows ECGs from a healthy heart and from a diseased heart. (c) A woman was found to have collapsed in the street. A paramedic obtained the following trace using a portable ECG monitor. healthy heart Explain why the person collapsed (4). diseased heart (c) Heart attack / myocardial infarction/ cardiac arrest; Branch of coronary artery blocked with blood clot/ atheroma; Reduced oxygen supply (to heart muscle; Ventricular fibrillation / ventricles quiver; Random / haphazard depolarisation of cells in ventricle; Uncoordinated waves /No coordinated heart beat; Atria and ventricles not contracting simultaneously; Rapid drop in blood pressure; electrical activity in muscles of atria electrical activity in muscles of ventricles Looking at the ECGs, a consulting cardiologist was reasonably certain that the damage caused to the diseased heart had not affected the sinoatrial node. Explain why (2) (b) frequency/distance between peaks varies/ arrhythmia; Markschemes SAN is in the (right) atrium; ECG from the healthy person is identical to the trace for the diseased heart in the region of the atria; (a) 5 complete cardiac cycles; 5 × 12 = 60 (beats per minute; Markscheme 3 Bio Factsheet 234. Electrocardiograms (ECGs) www.curriculum-press.co.uk Linking electrical activity to blood flow Exam Hint:- Don’t go into the exam hall if you can’t explain Fig.8! Fig. 8 shows the pressure, volume and electrical changes that occur during the cardiac cycle. Fig.8 An electrocardiogram (ECG) and associated pressure changes semilunar valve closes 120 semilunar valve opens 100 pressure (mm Hg) 4 aortic pressure 3 80 60 40 atrioventricular valve open atrioventricular valve closed 20 atrial pressure 5 1 6 2 0 ventricular pressure R ECG trace T P Q 0 0.1 atrial systole S 0.2 0.3 0.4 time (s) ventricular systole 0.5 0.6 0.7 0.8 Aorta Atrial and ventricular diasole P: atrial systole (contraction) The wave of depolarisation in the walls of the atria i.e. atrial systole. The atria contract and blood flows into the ventricles. semilunar (aortic) valve QRS: ventricle systole (contraction) the wave of depolarisation in the walls of the ventricles i.e. ventricular systole. The ventricles contract and the valve between atrium and ventricle closes bicuspid (atrioventricular) valve Left atrium Left ventricle T : ventricular diastole. The ventricles relax 1. Atria contracting so blood flowing into ventricle 2. Ventricles start to contract so ventricular pressure > atrial pressure and the atrioventricular valve closes 3. Ventricular pressure > aortic pressure forcing open aortic valve so blood flows from the ventricle into the aorta 4. Ventricular pressure falls below aortic pressure, so aortic valve closes 5. Ventricular pressure falls below atrial pressure so that blood flows from the atria to the ventricles and ventricular volume rises rapidly 6 Atrium filling with blood from pulmonary vein until atrial pressure> ventricular pressure and blood flows from atrium to ventricle Acknowledgements: This Factsheet was researched and written by Kevin Byrne and Martin Griffin. Curriculum Press, Bank House, 105 King Street, Wellington, Shropshire, TF1 1NU. Bio Factsheets may be copied free of charge by teaching staff or students, provided that their school is a registered subscriber. No part of these Factsheets may be reproduced, stored in a retrieval system, or transmitted, in any other form or by any other means, without the prior permission of the publisher. ISSN 1351-5136 4