Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Electrocardiography wikipedia , lookup
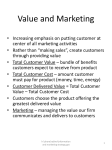
Differentiation of "A-V Junctional Rhythms" By BENJAMIN J. SCHERLAG, PH.D., RALPH LAZZARA, M.D., AND RICHARD H. HELFANT, M.D. SUMMARY Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Considerable controversy exists regarding the site(s) of origin of so-called junctional rhythms. However, experimental and clinical evidence indicates that a more precise identification of the origin of these rhythms is now possible. Microelectrode recordings from the atrioventricular (A-V) junction have clearly demonstrated that all three zones of the A-V node (upper nodal [AN], midnodal [NI, and lower nodal [NH] regions) exhibit action potentials which are functionally different from those recorded in contiguous atrial and His bundle cells. In addition, the amplitude and rate of rise of A-V nodal action potentials are markedly depressed by acetylcholine, a relative sensitivity not shared by atrial and His bundle cells. Cells of the AN and NH regions of the A-V node do show pacemaker activity as do His bundle cells. Experimental studies using His bundle recording techniques indicate significant differences in heart rate between nodal rhythms produced by sinus node isolation or suppression (average: 94 ± 22 beats/min) and His bundle rhythms caused by A-V nodal destruction (average: 39 ± 9 beats/min). Nontoxic doses of ouabain significantly reduced the average A-V nodal rate to 55 beats/min whereas the same dose regimen did not change the average rate of His bundle rhythms. Several clinical studies have claimed that the absence of "A-V nodal" potentials during so-called middle and lower A-V nodal rhythms indicate a site of origin in the His bundle and not the A-V node. However, the nondescript, sometimes spurious nature of A-V nodal recordings severely Lrmnts th.s approach to differentiation of junctional rhythms. Recent clinical studies using His bundle recordings showed that patients with complete heart block and narrow QRS complexes could be clearly divided into two groups. In one group the heart rates ranged from 45-60 beats/min and invariably increased significantly following atropine administration (A-V nodal pacemakers). In the other group heart rates ranged from 35-45 beats/min and there was no significant response to atropine (His bundle pacemakers). Intra-His bundle block could be documented in several patients in the latter group, confirming the His bundle location of the ventricular pacemaker. In conclusion, evidence gained from experimental in vivo and in vitro animal studies and from clinical investigations clearly suggests the existence of at least two pacemakers in the A-V junction. The two A-V junctional pacemakers are distinctly different in both heart rate and chronotropic response to cholinergic or cholinergic-blocking agents. Additional Indexing Words: Atrioventricular node Atrial pacing His bundle recordings His bundle pacing Atrioventricular conduction Tl' HE LOCALIZATION of pacemaker activity in the atrioventricular (A-V) node and the His bundle region has been a subject of considerable debate. As many as five different pacemaker sites have been described in the A-V junction: coronary sinus ostium, the upper, middle, and lower A-V node,' and more recently, the His bundle.2 In Heart rate the past, the distinction between these various pacemakers was made primarily on the basis of the temporal relationship between the retrograde P wave and the QRS. The latter ordinarily shows the same shape and duration as seen during supraventricular rhythms. It has since become clear that these temporal relationships can be affected by relative antegrade and retrograde conduction times as well as by the location of the pacemaker.3 Despite abundant accumulated evidence for the existence of A-V nodal automaticity,4 in recent years some experimental findings have fostered the concept that the A-V node is devoid of automaticity.5 Rhythms once attributed to the A-V node are now referred to as low atrial or His bundle rhythms.5' 6 The inability to resolve this controversy has led to a semantic compromise: the term "junctional rhythm."7 The purpose of this paper is From the Division of Cardiology, Department of Internal Medicine, Mount Sinai Medical Center, Miami Beach, Florida; The University of Miami School of Medicine, Coral Gables, Florida; and the Division of Cardiology, Department of Medicine, Presbyterian-University of Pennsylvania, Philadelphia, Pennsylvania. Address for reprints: Dr. B. J. Scherlag, Division of Cardiology, Mount Sinai Medical Center, 4300 Alton Road, Miami Beach, Florida 33140. Received January 12, 1973; revision accepted for publication March 20, 1973. 304 Circulation, Volume XLVIII, August 1973 JUNCTIONAL RHYTHMS to examine evidence gained from microelectrode and catheter electrode recordings in experimental and clinical situations as they apply to the site of origin of junctional rhythms. On the basis of these data, a more precise classification of some of these rhythms is suggested. Definition of Terms Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 The terms to be discussed are defined as follows: 1) The A-V junction, according to the concept of Pick and Langendorf,' includes the specialized atrial fibers in the low right atrium or coronary sinus near the A-V node, the A-V node itself, and the common bundle or His bundle. 2) The A-V node, according to the concept of Hoffman and Cranefield,2 includes "the entire complex of fibers functionally interposed between the atrial fibers proper and the His bundle proper." On the basis of differences in electrical properties, the A-V node has been subdivided into an upper nodal (AN) region, a midnodal (N) region, and a lower nodal (NH) region.8' 9, 10 The action potentials of the AN are morphologically intermediate between those of the atrium and the N region. Those of the NH region similarly bridge the N region and the His bundle. In all these regions (AN, N, NH) conduction is slower than in the atrium or the His bundle. The upstroke velocity and action potential amplitude are correspondingly low. 3) The common bundle or His bundle is that structure which sits on the crest of the intraventricular septum connecting the A-V node with the bundle branches. According to Lev and Widran,"1 Hudson,12 and more recently, Rosenbaum et al.,13 the bundle of His is composed of two segments. "The penetrating portion of the bundle travels from the distal end of the A-V node to a point where the initial radiations of the left bundle are given off." The branching portion stems from the point where the bundle starts to emit the most posterior fibers of the left bundle to the point which marks the origin of the right bundle branch and the most anterior fibers of the left bundle branch.'3 Microelectrode Recordings from the A-V Junction Microelectrode techniques have been utilized to ascertain the differential responses of the cells of the A-V node and His bundle to various physiological and pharmacological interventions. Block of premature impulses may occur in any of the three regions.'4' 15, 16 All of these cells in the A-V node share a far greater sensitivity to acetylcholine than Circulation, Volume XLVIII, August 1973 305 those of the His bundle proper.'7 The loss of amplitude and upstroke velocity of the action potential of the A-V nodal cells with acetylcholine is a response which is qualitatively different from ordinary atrial cells or the cells composing the His bundle. In common with His bundle cells and some specialized atrial cells (sinus node), cells of the NH5 and AN'8 regions of the A-V node show pacemaker activity. The action potentials of His bundle cells have greater amplitude and upstroke velocity than those of the A-V nodal cells.2 In contrast to the A-V nodal cells, the amplitude and upstroke velocity of the His bundle cells are relatively constant over a wide range of heart rates and are relatively insensitive to acetylcholine.17 His bundle cells display slow diastolic depolarization, and pacemaker activity can occur when complete heart block is produced by acetylcholine.2 The rate of diastolic depolarization is relatively unaffected by acetylcholine.17 Thus the response of the action potentials of the A-V node and His bundle to rate changes, as well as their responses to acetylcholine, are clearly different. However, specific A-V nodal cell types and His bundle cells do show spontaneous depolarization characteristic of pacemakers. Characteristics of Junctional Pacemakers in Experimental Studies Rate Recent studies in animals and man, employing electrode catheter recordings from the A-V junction, have established criteria for differentiating junctional rhythms. Experimental studies in dogs with A-V nodal escape rhythms, induced after cooling or crushing of the sinoatrial node (SA), showed A-V nodal escape rates during pentobarbital anesthesia of 94 ± 22 beats/min.19 On the other hand, in animals with heart block, caused by local injection of the A-V node with formaldehyde, the QRS configuration and duration remained essentially unchanged and the heart rate averaged 39 +9 beats/min. Figure 1 shows typical recordings in a dog with sinus rhythm, A-V nodal rhythm, and His bundle rhythm during complete heart block. During A-V nodal rhythm, the His bundle potential precedes atrial and ventricular activity, a recording which is characteristic of the mid A-V nodal rhythm. With the induction of complete heart block, atrial and ventricular activity are completely dissociated but the His bundle potential still precedes the essentially unchanged QRS complex SCHERLAG, LAZZARA, HELFANT 306 A NSR L-2 HBe S A 1.- 1- a & g -1- -y- -1 l BH 130/min I 1 k- . = 1 1 l- I BH AV = 79/min A jS 0 .1, -. *1 BH I.15II, & BH Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 C I LH 1- ll- AL ~L wmru ~ ~ 49/min (Complete Heart Block) BH _ -1i ---1I a WA~ lONSOOP ~~~ = LL BH I v-rl11' L --dmmmmmb& -JL- W.. BH tl Figure 1 Atrial, His bundle, and ventricular relationships in a dog during normal sinus rhythm (NSR), A-V rhythm (AV) and His bundle rhythm (BH). The top trace in each panel is a standard lead II electrocardiogram (L-2); below is the His bundle electrogram (HBe) showing atrial, A; His bundle, BH; and late activity in the base of the ventricular septum, S. A) Normal sinus rhythm at a rate of 130/min with His bundle activity occurring during the P-R interval of the surface electrocardiogram. B) A-V nodal rhythm at a rate of 79 beats/mim produced by cooling the sinoatrial node. Note that His bundle activity precedes atrial activity which in turn occurs just prior to ventricular activity. C) His bundle rhythm at 49 beats/mim with complete heart block produced by injection of A-V node with formaldehyde. Note the dissociation of atrial activity from ventricular activity. A His bundle deflection precedes each ventricular complex and a normal QRS configuration persists. The interval between time lines equals 1 sec. Reproduced with permission of the Amer Heart J (81: 227, 1971). by the same interval as that seen during normal sinus rhythm and A-V nodal rhythm. In addition to these physiologic differences, A-V nodal and His bundle rhythms also have differential chronotropic responses to ouabain.19 With progressively increasing (nontoxic) doses of ouabain, the mean rate of A-V nodal rhythm decreased from 94 to 55 beats/min. In contrast, in animals with His bundle rhythms, there was no significant change in heart rate over the same range of ouabain dosages (average rate, 40 beats/min). Thus, experimentally created A-V nodal and His bundle rhythms have markedly different "escape" rates and chronotropic responses to ouabain. Conduction In another study from our laboratory, on the intact dog heart, retrograde conduction from the His bundle to the sinus node area was significantly longer during His bundle rhythms, produced by pacing the His bundle, than during spontaneous mid A-V nodal rhythms at the same heart rate.20 Figure 2 illustrates a lead II electrocardiogram recorded in conjunction with electrograms taken from the area of the sinus node (SA), the region of the His bundle (Hb), and the area of the coronary sinus (CS). Changes in sequence of activation of different recording sites are noted as the rhythm changes from sinus rhythm to A-V nodal rhythm and His bundle pacing rhythm. In panel B a mid A-V nodal rhythm was produced by crushing the sinus node. Note that the sequence of atrial activation then proceeded from the low atrium to the high right atrium with coronary sinus and atrial activity in the region of the His bundle preceding sinus node activation. The P wave is coincident with Circulation, Volume XLVIII, August 1973 JUNCTIONAL RHYTHMS A Sinus 307 Rhythm Hb ,^jp CS v 1 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 C His Bundle Pacing pi HR = 62/min PI-R 33 msec = PI H-SA = 115 msoc H-CS =100 mseccl Figure ; 2 A comparison of retrograde His bundle to atrium conduction in the dog during mid A-V nodal (Middle "Nodal" Rhythm) and electrically induced His bundle rhythm showing atrial (A), His bundle (H), and ventricular (V) activation. Traces in panels A and B, starting from the top: Lead II ECG (L-2); bipolar electrograms from the sinus node area (SA), the His bundle (Hb), and coronary sinus ostium (CS). In panel C traces are Lead II ECG and bipolar electrograms from SA and CS. A) During sinus rhythm (heart rate 120 beats/min) initial activity occurred in the sinus node area. Then the atrium was activated in the A-V-node-His-bundle region (A). Atrial activation in the area of the coronary sinus ostium followed. The H-V time was 32 msec. B) After crushing the sinus node, a mid A-V nodal rhythm (heart rate 65 beats/min) was produced with the P wave temporally coincident with the QRS. His bundle activation preceded all activity and the H-V time remained unchanged (32 msec). However, atrial activity in the His bundle electrogram was coincident with the early portion of the ventricular activation (note V complex in panel A) and was the earliest atrial activation recorded. Activation in the area of the coronary sinus ostium (CS) and sinus node (SA) followed. The retrograde conduction time from the onset of His bundle activity to the CS and SA activation was 35 and 50 msec, respectively. C) During His bundle pacing at essentially the same rate as the spontaneous mid A-V nodal rhythm (panel B), the time from delivery at the pacing impulse (PI) to activation of the CS and of the SA was 100 and 115 msec, respectively. Note that the time from PI to the onset of ventricular activity closely corresponded to the previously measured H-V time (panels A and B) and the QRS was identical to that seen during sinus and mid A-V nodal rhythm. The interval between time lines equals 1 sec. ventricular activation and thus is not seen on the surface electrocardiogram. The His bundle deflection (H) precedes ventricular activation by 32 msec, the same as that seen during sinus rhythm. If this mid A-V nodal rhythm actually arises in the His bundle, as has been suggested by Damato et al.,6 it should be possible to pace the His bundle at approximately the same rate as the mid A-V nodal Circulation, Volume XLVIII, August 1973 rhythm and show that the time from the paced impulse back to any part of the atrium is essentially the same as that seen during the spontaneous mid A-V nodal rhythm. In panel C (fig. 2), His bundle pacing was achieved at a slightly lower heart rate than the mid A-V nodal rhythm (A-V nodal rhythms can be readily suppressed by overdrive). Note that the QRS is unchanged from that recorded SCHERLAG, LAZZARA, HELFANT 308 Table 1 Comparison of Spontaneous Mid Nodal Rhythm and His Bundle Rhythm at Similar Heart Rates in Dogs* Spontaneous mid A-V nodal rhythm HR BH-SA (beats/min) (msec) Exp. 1 2 3 4 108 92 95 6 7 Average SD 109 90 124 103 103l1 His bundle pacing BH-SA HR (msec) 75 50 45 65 39 45 50 150 62 105 105 75 65 93 53 12t 94 2St (beats/min) 108 93 90 103 95 12 5 104 103 9 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Abbreviations: HR = heart rate; BH = bundle of His; SA = sinus node. *From reference 20. tPaired t test, P < 0.01. during spontaneous A-V nodal rhythm or sinus rhythm and that the time from the pacer impulse to the R wave (PI-R) is equal to 33 msec, the same as the H-V time as measured in panels A and B during spontaneous rhythm and mid A-V nodal rhythm, respectively. However, the time from the stimulus applied at the His bundle to activation of the SA node electrogram and the coronary sinus electrogram was 115 and 100 msec, respectively. This is ECG P8EQ A-V Nodal Potentials Several recent studies have utilized catheter recordings of A-V nodal potentials2 to differentiate the origin of junctional rhythms.6 22 Damato et al.6 indicated that recordings of A-V nodal potentials were made in three patients with so-called middle and lower A-V nodal rhythm. Pacing of the atrium at a faster rate than the nodal rate resulted in a sequence consisting of atrial depolarization, a small slow potential, His bundle activation, and ventricular activation. During A-V nodal rhythm the slow S :QR HBE markedly longer than the time measured from the recorded His bundle deflection to the SA nodal electrogram or the coronary sinus electrogram during the spontaneous mid A-V nodal rhythms. The significant increase of conduction time during His pacing reflects the delay of the impulse across the entire A-V node. During mid A-V nodal rhythms the impulse must traverse only a portion of the A-V node. The average values and standard deviations recorded for retrograde conduction time during mid A-V nodal rhythms and during His bundle pacing at the same heart rate show that the retrograde conduction time during the His bundle pacing is significantly increased when compared with conduction time during spontaneous A-V nodal rhythm (table 1). Xi.~~~~~~~~. l : Qf*0;120 Q . 4 P'@ 4 He Z ., .e . .0 .. 1. Figure 3 Influence of electronic filtering on slow waves in the P-R interval in a patient. The two traces above are standard lead 11 and a His bundle electrogram recorded with bandpass fiters of 0.1 to 200 Hz. Note that the His deflection in the second trace occurs on the crest of a slow wave. In the bottom trace, the His bundle electrogram frequency settings of 40-500 Hz show a deflection resembling an N potential at the end of atrial depolarization but prior to His bundle depolarization. cps= Hz. (From Circulation 39: 13, 1969). Circulation, Volume XLVIII, August 1973 I JUNCTIONAL RHYTHMS ,;1;0__L t S t oVR t m cYF vi t BE i-; A A 770 msec RR 1 320 msec H-V 40 msec 309 X E 2m VZ V3 F7 e~~~~~~~~~~~~~~~MW. VS V4 Vt6 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Li-R aVR _ a V F~~~~~~~~~~~~~~~~~~~~~~~~~~ Figure 4 His bundle electrocardiographic analysis of a patient with complete heart block in which the lesion was localized proximal to the recording of the bundle of His electrogram. At the top are 12 standard ECG leads showing a narrow QRS complex with atrioventricular dissociation. The His bundle recording showed His bundle activity (BH) constantly linked to ventricular activity (V) and QRS complexes (H-V = 40 msec, R-R = 1320 msec). Atrial activity (A) occurs at a cycle length of 770 nsec and is independent of ventricular activation. (Modified from Circulation 41: 437, 1970). A-V nodal or "N potentials" did not precede His bundle activity but were associated with atrial activity, the latter usually occurring during or after ventricular activation. However, each QRS complex was preceded by a His bundle potential. The authors interpreted these data as evidence that the site of origin of these rhythms was the His bundle, not the A-V node. However, an isoelectric segment was usually interposed between the A-V nodal deflection and the His deflection. Since activation of A-V node is continuous throughout the interval between activation of the atrium and the His bundle,'0 a portion of A-V nodal activation must occur during the isoelectric interval present in the recordings reported in the study by Damato et al., as well as in the isoelectric interval recorded in another similar study in the experimental animal." 22 This argues against the authors' contention that the absence of an A-V "nodal potential" preceding a His deflection localizes the pacemaker in the His bundle, because the A-V nodal activity occurring during the isoelectric interval may be unrecorded or undetectable.23 Circulation, Volume XLVIII, August 1973 Slow deflections recorded at the A-V junction should be interpreted cautiously. False potentials were recorded by Scher et al.24 In addition, slow potentials are invariably present during the P-R interval in unfiltered records (fig. 3). These slow EkontrD t i -- HR 401-'n 1-2 FVigure 5 Electrocardiogram shzowinig the response of a patient with complete heart block to atropine. A previous His bundle study indicated block was proximal to the recorded His bunldle electrogram. A) Note the slow ventricular rate of 40 beats/mmn and dissociated atrial rate of 73 beats/mzn. B) After 0.5 mg atropine, the ventricular rate increased to 75 beats/mmn. The QRS retained its configuration duration and complete A-V block is still evidenlt. (From Circulation 41: 437, 1970). SCHERLAG, LAZZARA, HELFANT 310 evidence for the existence of pacemakers in the A-V node and His bundle. Both physiological and pharmacological studies were performed on 25 patients with complete heart block and a narrow QRS complex.26 Figures 4-6 illustrate examples of the two groups of patients which were defined. In fig. 4 a bipolar His bundle recording (BE) was made in a patient with complete heart block and a narrow QRS complex (see 12 lead ECG above and three simultaneously recorded ECG leads I, aVR, and aVF below ).27 It can be seen that the ventricular activity was preceded in each cycle by a His bundle deflection. Atrial activity was not related to either His bundle or ventricular activation. With the administration of a small dose of potentials are presumably associated with atrial repolarization.25 The application of the conventional filter settings to record the His bundle electrogram (40-200 Hz) can convert the slow potentials into A-V "nodal humps" or "N potentials" (see fig. 3). Indeed, Hoffman et al. have suggested that upstroke velocities of cells of the A-V node are too slow to be recorded by commonly used extracellular techniques.25 Thus, the nondescript, spurious nature of A-V nodal recordings would severely limit if not totally exclude their usefulness in differentiating the site of origin of junctional rhythms. Clinical Studies Recent studies in man have provided further Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 t BE - v A -YU*VR W lA 't 4- i i 1 A ' A-A II 401 940 ,A.jliH H | 90'v'se 40 s.c 940 o .Hl90 t, RH 440 150 125 SN 600 40 37/min~ H-R L-2 c l-3 vP 5 t Bs 7f -il Pi-1 40 BHR 085/m L-3 t C P1 R2 40 ml@c Figure 6 His bundle electrocardiographic analysis of patient with complete heart block and narrow QRS complex. At the top are the 12 standard ECG leads showing QRS complex and dissociated atrial activity. A) The His bundle electrogram (BE) indicates two rapid deflections, one associated wtih atrial activity, the other associated with ventricular activity (BH and BH', respectively). Premature atrial stimulation (PI = pacer impulse) shows that the A to BH time widens from 90 to 150 msec. B) C) Validation of the BH' potential was performed by His bundle pacing at a heart rate of 57-85 beats/min. Note that the QRS is the same as that recorded during spontaneous ventricular activity, (panel A), and the stimulus to R wave interval (PI-R = 40 nsec) is exactly the same as the measured BH'-V interval. (From Circulation 41: 77, 1970.) Circulation, Volume XLVIII, August 1973 JUNCTIONAL RHYTHMS 311 Table 2 Electrophysiological and Pharmacological Characteristics of Pacemakers in Patients with Complete Heart Block Group A Group B QRS duration (msec) Heart rates (beats/min) Site of block by His electrogram recording 0.08-0.10 45-60 Proximnal to His 36-43 recording Distal to His 0.08-0.10 recording or Response to atropine Marked increase in rate (35-45 beats/min) No appreciable rate change ( 5 beats/min) Probable site of pacer A-V node His bundle intra-His lesion Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 atropine the heart rate accelerated from a rate of 40 to 75 beats/min (fig. 5). In fig. 6 another patient who exhibited complete heart block and a narrow QRS complex was studied using His bundle-electrocardiography. In this case the His bundle recording showed that there were two deflections recorded on the His bundle electrogram (BE )-one associated with atrial activity (BH) and the other preceding ventricular activity (BH' )27 That both these deflections emanate from the His bundle was validated by recordings during an induced premature beat (PI) which widened the A-H interval from 90 to 150 msec, an increase that indicates that this deflection (BH) was not part of atrial activity. In addition, panels B and C illustrate that pacing from the His bundle recording electrodes produced capture of the ventricles with 1:1 conduction. During pacing the same QRS morphology was produced as in the unpaced state in all leads, and the time interval from the pacer impulse to ventricular activation (PI-R) was the same as the unpaced H-V time seen in panel A (40 msec). Atropine induced no significant change of rate (an increase of 5 beats or less) in contrast to its marked effect on the first patient discussed. In table 2 this series of patients with complete heart block is separated into two groups, each showing a narrow QRS complex. In group A the heart rates ranged from 45 to 60 beats/min and invariably increased significantly with atropine. In group B the heart rates ranged from 35 to 45 beats/min and the block was located distal to the recorded His bundle deflection. In several cases intra-His bundle lesions could be discerned by recording of double but dissociated His bundle deflections (see fig. 6). There was no appreciable effect of atropine on heart rate in these patients. These differential responses to atropine in patients with block proximal to the recorded H deflection or blocks localized within the His bundle have also Circulation, Volume XLVIII, August 1973 been reported recently by Rosen et al.29 Thus, the site of block in patients with complete heart block and narrow QRS can be differentiated on the basis of escape rates and heart rate response to atropine. Conclusion In summary, studies in both the experimental animal and in man indicate that rhythms arising in the A-V junction can be differentiated into at least two groups. Basic electrophysiologic studies indicate that action potentials in the A-V node and His bundle clearly respond differently to rate changes and to acetylcholine. Experimentally created A-V nodal and His bundle rhythms have different escape rates and chronotropic responses to ouabain. In addition, conduction times from His bundle to atrium in A-V nodal rhythms and during His bundle pacing at the same rate are significantly different. In man, A-V nodal escape rhythms are relatively fast (45-60 beats/min) and the rate increases markedly in response to atropine. Escape rhythms arising in the His bundle are somewhat slower (35-45 beats/min), and their rate is relatively unchanged by atropine. References 1. ZAHN A: Experimentelle untersuchungen ueber die reizbildung und reizleitung im atrioventrikular knoten. Arch Ces physiol 151: 247, 1913 2. HOFFMAN BF, CRANEFIELD PF: Electrophysiology of the Heart. New York, McGraw-Hill, 1960, ch 6 3. SCHERF D, SHOOKHOFF C: Experimentelle unter suchungen ueber die umker-extrasystole. Wein Arch Inn Med 12: 501, 1926 4. SCHERF D, COHEN J: The Atrioventricular Node and Selected Cardiac Arrhythmias. New York, Grune and Stratton, 1964, pp 48-58 5. HOFFNIAN BF, CRANEFIELD PF: The physiological basis of cardiac arrhythmias. Amer J Med 37: 670, 1964 6. DAMATO AN, LAU SH: His bundle rhythms. Circulation 40: 527, 1969 312 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 7. PICK A, LANGENDORF R: Recent advances in the differential diagnosis of A-V junctional arrhythmias. Amer Heart J 76: 553, 1968 8. HOFFMAN BF, PAES DE CARVALHo A, DEMELLO WC: Electrical activity of single fibers in the A-V node. Nature 181: 66, 1958 9. MATSUDA K, HosHi T, KAMEYAMA S: Action potential of the A-V node. Tohoku J Exptl Med 68: 8, 1958 10. PAES DE CARVALHO A, ALMEIDA DF: Spread of activity through the A-V node. Circ Res 8: 801, 1960 11. LEV M, WIDRAN J, ERICKSON EE: A method for the histopathologic study of the atrioventricular node, bundle and bundle branches. AMA Arch Path 52: 72, 1951 12. HUDSON REB: The human conducting system and its examination. J Clin Path 16: 492, 1963 13. ROSENBAUM MB, ELIZARI MV, LAZZARI JO: The Hemiblocks. Tampa Tracings, 1970, ch 2 14. MOORE EN: Microelectrode studies on concealment of multiple premature atrial responses. Circ Res 18: 660, 1966 15. MooRE EN: Microelectrode studies on retrograde concealment of multiple premature ventricular responses. Cire Res 20: 88, 1967 16. MOORE EN: Observations on concealed conduction in atrial fibrillation. Circ Res 21: 201, 1967 17. CRANEFIELD PF, HOFFMAN BE, PAES DE CARVALHO A: Effects of acetylcholine on single fibers of the atrioventricular node. Circ Res 7: 19, 1959 18. WATANABE Y, DREIFUS LS: Sites of impulse formation within the atrioventricular junction of the rabbit. Circ Res 19: 717, 1968 19. SCHERLAG BJ, ABELLEIRA JL, NARULA OS, SAMET P: The differential effects of Ouabain on sinus A-V nodal, His bundle and idioventricular rhythms. Amer Heart J 81: 227, 1971 SCHERLAG, LAZZARA, HELFANT 20. SCHERLAG BJ, ABELLEIRA JL, SAMET P: Differentiation of middle, lower A-V nodal and His bundle rhythms in the dog. (abstr) Fed Proc 28: 587, 1970 21. DAMATO AN, LAU SN, BERKOWITZ WD, ROSEN KM, Lisi KR: Recording of specialized conducting fibers (A-V nodal, His bundle and right bundle branch) in man using an electrode catheter technique. Circulation 39: 435, 1969 22. DAMATO AN, LAU SH, BOBB GA, WIT AL: Recording of A-V nodal activity in the intact dog heart. Amer Heart J 80: 353, 1970 23. SCHERLAG BJ: Recording of A-V nodal activity (letter to the editor). Amer Heart J 81: 579, 1971 24. SCHER AM, RODRIGUEZ MI, HAMLIN RL: Observations on atrioventricular conduction and on distribution of the impulse in the ventricles of ruminants and other mammals. In The Specialized Tissues of the Heart, edited by PAES DE CARVALHO A, DEMELLO WC HOFFMAN BF. Amsterdam, Elsevier Co, 1961, p 159 25. HOFFMAN BF, CRANEFIELD PF, STUcKEY JH, BAGDONAS AA: Electrical activity during the P-R interval. Circ Res 8: 1200, 1960 26. NARULA OS, SCHERLAC BJ, SAMET P: His bundle blocks and His bundle rhythms (abstr). Dis of Chest 56: 238, 1969 27. NARULA OS, SCHERLAG BJ, JAVIER RP, HILDNER FJ, SAMET P: Analysis of the A-V conduction defect in complete heart block utilizing His bundle electrograms. Circulation 41: 437, 1970 28. NARULA OS, SCHERLAG BJ, SAMET P: Pervenous pacing of the specialized conducting system in man: His bundle and A-V nodal stimulation. Circulation 41: 77, 1970 29. ROSEN KM, MEHTA A, RAHIMmrOoLA SH, MILLER RA: Sites of congenital and surgical heart block as defined by His bundle-electrocardiography. Circulation 44: 883, 1971 Circulation, Volume XLVIII, August 1973 Differentiation of "A-V Junctional Rhythms" BENJAMIN J. SCHERLAG, RALPH LAZZARA and RICHARD H. HELFANT Circulation. 1973;48:304-312 doi: 10.1161/01.CIR.48.2.304 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1973 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/48/2/304 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/