Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Heart failure wikipedia , lookup
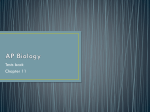
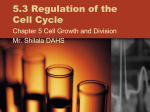
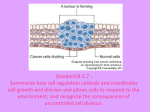
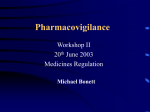
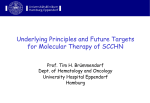
Am J Physiol Heart Circ Physiol 288: H1925–H1930, 2005; doi:10.1152/ajpheart.01054.2004. Involvement of mitogen-activated protein kinases in adriamycin-induced cardiomyopathy H. Lou, I. Danelisen, and P. K. Singal Institute of Cardiovascular Sciences, Department of Physiology, St. Boniface General Hospital Research Centre, Faculty of Medicine, University of Manitoba, Winnipeg, Canada Submitted 13 October 2004; accepted in final form 1 December 2004 dilated cardiomyopathy; oxidative stress and apoptosis ADRIAMYCIN (ADR), an anthracycline antibiotic, has been widely used in the treatment of a variety of tumors and carcinomas; however, its clinical application is limited by its irreversible cardiac side effect of cardiomyopathy and congestive heart failure (13, 22). The characteristic features of ADRinduced cardiomyopathy (AIC) include dose dependency, refractoriness to inotropic support, dilation of the membrane tubular system, myofibril drop out, and lack of inflammatory cytokine upregulation (13, 17, 22). Although the mechanism of AIC is multifactorial, increased oxidative stress due to overproduction of free radicals and antioxidant-deficit play an Address for reprint requests and other correspondence: P. K. Singal, Institute of Cardiovascular Sciences, St. Boniface General Hospital Research Centre, Rm. 3022, 351 Tache Ave., Winnipeg, Manitoba R2H 2A6, Canada (E-mail: [email protected]). http://www.ajpheart.org important role (16, 23). In addition, cardiac cell apoptosis has been suggested to be associated with AIC (2, 11). However, the role of oxidative stress in the intracellular signaling pathways and cardiomyocyte apoptosis in AIC remains unknown. Mitogen-activated protein kinase (MAPK) signaling pathways are the primary intermediator of induction of apoptosis by oxidative stress. There are three major MAPK families, including extracellular signal-regulated kinases (ERKs), p38, and c-Jun NH2-terminal kinases (JNKs). In the cardiovascular system, ERK1/2 are potently and rapidly activated by growth factors and hypertrophic agents thereby mediating cell survival as well as offer cytoprotection (24, 26). In contrast, JNKs and p38-MAPKs are activated by cellular stresses, including oxidative stress, and are thought to correlate with cardiomyocyte apoptosis and cardiac pathologies (12, 21, 28). The current study investigated the role of ERK1/2, p38, and JNKs MAPKs in the early stage of AIC and heart failure in rats. Because the antioxidant probucol can completely prevent AIC by reducing oxidative stress, modulatory effects of probucol on ADR-induced changes in MAPKs were investigated. Pro- and anti-apoptotic proteins caspase-3, Bax, and Bcl-xl were also examined to define the significance of MAPKs and cardiomyocyte apoptotic signaling in AIC. MATERIALS AND METHODS Animal groups and treatment. ADR-induced cardiomyopathy and heart failure were produced according to the established protocol (23). Male Sprague-Dawley rats (250 ⫾ 10 g body wt) were divided into four groups: control, ADR, ADR ⫹ probucol, and probucol. ADR was administered in six equal doses (2.5 mg 䡠 kg⫺1 䡠 dose⫺1 ip), on alternate days, over a period of 2 wk for a cumulative dose of 15 mg/kg. Probucol was given in 12 doses for a period of 2 wk before the administration of ADR and 2 wk during the administration of ADR (cumulative dose 120 mg/kg ip). After the final injection, rats in the early stage of cardiomyopathy were anesthetized with an intraperitoneal injection of a ketamine (90 mg/kg) and xylazine (10 mg/kg) mixture and euthanized at 1, 2, 4, and 24 h. Rats for the late-stage studies were observed for body weight, general appearance, behavior, and mortality for 3 wk. At the end of the 3-wk posttreatment period, animals were assessed hemodynamically, and the heart, lung, and liver tissues were collected for the further studies. All animal treatment procedures were according to the guidelines of the Animal Care Committee of the University of Manitoba. Cardiac function and hemodynamic study. After the 3 wk of the last injection, rats were anesthetized by inhalation of isoflurane and oxygen. The right carotid artery was cannulated with a microtip pressure transducer (model SPR-249; Millar Instruments, Houston, TX) to monitor the blood pressure heart function. With the use of the The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 0363-6135/05 $8.00 Copyright © 2005 the American Physiological Society H1925 Downloaded from http://ajpheart.physiology.org/ by 10.220.33.4 on June 16, 2017 Lou, H., I. Danelisen, and P. K. Singal. Involvement of mitogenactivated protein kinases in adriamycin-induced cardiomyopathy. Am J Physiol Heart Circ Physiol 288: H1925–H1930, 2005; doi: 10.1152/ajpheart.01054.2004.—The current study investigated the phosphorylation of mitogen-activated protein kinases (MAPKs) as well as pro- and anti-apoptotic proteins in adriamycin (ADR)-induced cardiomyopathy (AIC) and heart failure in rats. Modulatory effects of antioxidant probucol on the activation of MAPKs were also examined. Male rats were administered with ADR (15 mg/kg body wt ip, over 2 wk) with and without probucol (120 mg/kg body wt for 4 wk ip). Hearts from these animals were studied at 1- to 24-h as well as at 3-wk posttreatment durations. In the 3-wk group, ADR depressed cardiac function, increased left ventricular end-diastolic pressure (LVEDP), and caused dyspnea and mortality. These changes were prevented by probucol. Phosphorylation of extracellular signal-regulated kinase (ERK)1/2, in the early stage of AIC, showed a biphasic response, with a maximum increase to 513% seen at 4 h, followed by a decrease to 66.8% at 3 wk after the last injection of ADR. Phosphorylation of p38 and c-Jun NH2-terminal kinases (JNKs) showed a steady increase through 2, 4, and 24 h and 3 wk (116% to 148%). In gene microarray analysis at 3 wk (heart failure stage), mRNA expression for both ERK1/2 and p38 kinases was decreased, whereas JNK mRNA was undetectable. Probucol completely prevented these MAPK changes. Activation of caspase-3 as well as the increase in the ratio of Bax to Bcl-xl were seen at early time points (1–24 h) as well as in the heart failure stage (3 wk). It is suggested that a transient increase in ERK1/2 at a shorter interval indicate an early adaptive response, and failure of this response corresponded with heart failure. In contrast, a gradual and persistent increase in p38 and JNK MAPKs as well as in caspase-3 and the Bax-to-Bcl-xl ratio may contribute in the initiation of apoptosis and progression of heart failure. Because probucol modulated changes in cellular signaling pathways and cardiac function, it is likely that oxidative stress plays a key role in AIC and heart failure. H1926 MAP KINASES AND HEART FAILURE Table 1. Effects of probucol on adriamycin-induced changes in the late stage (3 wk) group Parameter Control ADR ADR⫹Pro Pro Body weight, g LVSP, mmHg LVEDP, mmHg ⫹dP/dt, mmHg/s ⫺dP/dt, mmHg/s ASP, mmHg ADP, mmHg Liver, wet-to-dry wt ratio Lung, wet-to-dry wt ratio Heart-to-body wt ratio Mortality, % 529.5⫾19.8 121.7⫾6.2 3.10⫾0.54 10,931⫾311 12,245⫾96 120.3⫾1.3 87.6⫾1.7 3.14⫾0.04 4.93⫾0.02 2.52⫾0.07 0 335.9⫾18.0* 96.5⫾0.7* 13.2⫾1.51* 8,631⫾114* 8,797⫾251* 93.2⫾1.6* 62.3⫾2.7* 3.47⫾0.10* 5.18⫾0.04* 2.13⫾0.09* 30 406.8⫾15.9 108.5⫾2.8 3.4⫾0.76 10,469⫾298 11,800⫾198 107.5⫾2.1 84.2⫾29 3.18⫾0.08 4.97⫾0.02 2.54⫾0.06 0 526.9⫾16.8 123.6⫾4.6 2.9⫾1.3 11,235⫾146 12,685⫾306 117.6⫾1.8 90.6⫾1.9 3.12⫾0.05 4.91⫾0.05 2.48⫾0.04 0 software AcqKnowledge for Windows 3.0 (Biopac Systems, Goleta, CA), left ventricular systolic pressure (LVSP), left ventricular enddiastolic pressure (LVEDP), the maximum rate of isovolumic pressure development (⫹dP/dtmax), the maximum rate of isovolumic pressure decay (⫺dP/dtmax), aortic systolic pressure (ASP), and aortic diastolic pressure (ADP) were recorded. Tissue weights and sample collection. The livers and lungs were weighed, chopped into small pieces, and dried in an oven at 65°C until a stable weight was recorded. The liver and lung wet-to-dry weight ratios were obtained (23). The hearts were quickly removed, and the ventricles were weighed and cut into two pieces. One-half of the heart was stored in RNA-Later solution (from Ambion) for gene-chip analysis, and the other half was kept in liquid nitrogen for other studies. Affymetrix gene-chip probe array analyses. Total RNA was isolated (TriReagent kits) and purified (QIAGEN kits). Two mRNA samples each from the control, ADR, and ADR ⫹ probucol groups were sent to The Centre for Applied Genomics (Hospital for Sick Children) for rat genome array (U34A) analyses. Western blot analysis. Phosphorylated and total ERK1/2, p38, and JNKs MAPKs were examined by Western blot analysis, using PhosphoPlus MAPKs antibody kits (Cell Signaling Technology). For protein isolation, the frozen heart tissues were powdered in liquid nitrogen and then suspended in cell lysis buffer [20 mM Tris (pH 7.5), 150 mM NaCl, 1 mM EDTA, 1 mM EGTA, 2.5 mM sodium pyrophosphate, 1 mM -glycerolphosphate, 1 mM Na3VO4, and 1 g/ml leupeptin]. The samples were homogenized and sonicated. The lysates were centrifuged at 14,000 rpm for 10 min, and the supernatant was transferred into a new tube and stored at 80°C. The quantity of the protein in the samples was measured by a dye-binding assay (Bio-Rad Laboratories) using bovine serum albumin as a standard. The isolated protein was subjected to SDS-PAGE and transferred to 0.45-m nitrocellulose membranes. The detection of membrane-bound proteins was performed with BM chemiluminescence blotting substrate (POD) kit (from Roche). The bands were visualized with Fluor S-MultiImager MAX system (Bio-Rad) and quantified by image analysis software (Quantity One, Bio-Rad). Pro- and anti-apoptotic proteins, caspase-3, Bax, and Bcl-xl were examined with their specific antibodies (bought from Cell Signaling Technology). Statistical analysis. Data were expressed as means ⫾ SE. Group means were compared by one-way ANOVA, and the Bonferroni’s test was used to identify differences between groups. The accepted level of significance was P ⬍ 0.05. RESULTS General observations, body weight, tissue weight, and hemodynamics. At the earlier time points (1–24 h), animals in all of the groups did not show any dyspnea or ascites, and no mortality was seen. During the 3-wk posttreatment period, rats in the ADR group developed a progressively enlarged abdomen, ascites, and dyspnea and showed 30% mortality related to Table 2. DNA microarray analysis for gene expression of MAPK signaling cascade proteins in the late-stage (3 wk) group Control Accession No. AJ00542 M61177 M64300 M64301 U73142 L27112 L27129 X96488 L27128 L04485 L14936 U48596 U23438 ADR ⫹ Pro ADR Gene Description Signal Detection Signal Detection Signal Detection BMK1/ERK5 protein ERK1 ERK2 ERK3 p38 MAPK SAP kinase ␣II mRNA SAP kinase ␥-isoform mRNA for SAP kinase-3 SAP kinase -isoform MAP kinase MKK2 MEKK1 MKP-2 18.4 22.5 101.5 278.6 305.5 9.1 26.8 36.2 4 188.1 95.2 53.2 6.2 A A P P P A A A A P A P A 10.6 108.3 63 238.1 117.8 22.1 24.8 32.9 14.4 281.7 85 16.8 4.9 A A P P P A A A A P A A A 16.4 124 93.9 188.2 269.5 12.2 17.9 40.6 8.8 309.8 174.6 46.8 14.1 A A P P P A A A A P A P A A, absent; P, present. Average of two independent assays. ERK, extracellular signal-regulated kinase 1; MAPK, mitogen-activated protein kinase; SAP, stress-activated protein kinase; MKK2, MAPK kinase; MEKK1, MAPK kinase kinase; MKP-2, MAPK phosphatase; ADR, adriamycin; Pro, Probucol. AJP-Heart Circ Physiol • VOL 288 • APRIL 2005 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.4 on June 16, 2017 Data are means ⫾ SE of 5– 6 rats in each group. Because of the high mortality in the adriamycin (ADR) group, the starting number of animals was higher. ADR, adriamycin; Pro, Probucol; LVSP, left ventricular systolic pressure; LVEDP, left ventricular end-diastolic pressure; ⫹dP/dt, rate of pressure development; ⫺dP/dt rate of pressure decay; ASP, aortic systolic pressure; ADP, aortic diastolic pressure. *P ⬍ 0.05 compared with control group. MAP KINASES AND HEART FAILURE AJP-Heart Circ Physiol • VOL Downloaded from http://ajpheart.physiology.org/ by 10.220.33.4 on June 16, 2017 heart failure. The ascites was hemorrhagic and ranged 50 –140 ml. The livers of ADR-treated rats were enlarged and appeared dark in color. There was a significant increase in the wet-to-dry weight ratio in the liver and lung (Table 1). During the 2-wk treatment period, animals in the ADR and ADR ⫹ probucol groups showed a significant decrease in heart and body weights. But there was a gain in body weight in the posttreatment duration. However, this weight gain never reached the weights of animals in the control group. In the 3-wk group, aortic systolic pressure (ASP), aortic diastolic pressure (ADP), and left ventricular peak systolic pressure (LVSP) were significantly lower in the ADR group. However, LVEDP was elevated more than fourfold in the ADR group. ⫾dP/dt values were depressed in the ADR group. Probucol prevented these changes as well as heart failure (Table 1). Myocardial MAPKs mRNA expression in ADR-induced heart failure. Gene expression of myocardial ERK1/2, p38, and JNKs kinases and their tiered cascade proteins at the heart failure stage was analyzed using DNA microarrays analysis, and the results are shown in Table 2. ERK2 and p38 mRNA expression was decreased in the failing hearts in the ADR group. JNK gene expression was undetectable in both ADR and control groups. Expression of MEKK1, an ERK1/2 kinases upstream stimulator, was also decreased in the ADR group. Probucol modulated these decreases in mRNA levels of ERK2 and p38 and MEKK1 kinases. Phosphorylation of different MAPKs in the early stage of AIC. Phosphorylation of ERK1/2, p38, and JNK kinases in the myocardium at 1, 2, 4, and 24 h after the last injection of ADR was studied, and the data are shown in Fig. 1, A–C. Phosphorylation of ERK1/2, in the early stage of AIC, showed a biphasic response (Fig. 1A). There was a 167% increase at 1 h, 209% at 2 h, and a 513% peak in the 4-h group. At 24 h, it decreased to 197% of control. Phosphorylation of p38 showed a steady increase through 2, 4, and 24 h (119%, 138%, and 148%, respectively), as shown in Fig. 1B. A gradual increase phosphorylation of JNK was also seen through 1, 2, 4, and 24 h (116%, 124%, 127%, and 148%, respecitvely), as shown in Fig. 1C. Phosphorylation of different MAPKs in ADR-induced heart failure. After 3 wk of posttreatment, phosphorylation of ERK1/2, p38, and JNK kinases was examined in the hearts from the control, ADR, ADR ⫹ probucol, and probucol groups, and the data are shown in Fig. 2, A–C. Phosphorylation of ERK1/2 showed a significant reduction by 66.8% of the control, and probucol prevented this decrease (Fig. 2A). In contrast, as shown in Fig. 2, B and C, phosphorylation of both p38 and JNK showed a significant increase to about 148% and 147%, respectively, in the ADR group compared with the control group. Probucol in the ADR ⫹ probucol group prevented this ADR-induced activation of p38 and JNKs kinases. Caspase-3 and Bax/Bcl-xl in AIC. Full length as well as cleaved caspase-3 proteins were examined in both early and late stages of AIC by Western blot analysis, and these data are shown in Fig. 3. The activity of caspase-3 was expressed as the ratio of cleaved caspase-3 over full length of caspase-3. When compared with the ratio in the control heart set at 100%, caspase-3 was activated in both the early and late stages of H1927 Fig. 1. A–C: phosphorylation of extracellular signal-regulated kinase (ERK1/2) (A), p38 (B), and c-Jun NH2 terminal kinase (JNK, C) mitogenactivated protein (MAP) kinases in adriamycin (ADR)-induced early cardiomyopathy (at 1 to 24 h). UP, myocardial phosphorylated MAP kinase was measured by Western blot analysis with a phospho-specific MAP kinase antibody. Total amounts of MAP kinases were examined from the same stripped membranes for each kinase with the kinase-specific antibodies. LP, densitometric analysis of MAP kinases activities. Values are the ratio of phospho-specific MAP kinases to total MAP kinases. Results were normalized for all experiments by a random setting of the densitometer of the control heart samples as 100%. Data in the LP are means ⫾ SE from 4 hearts in independent experiments. *P ⬍ 0.05 vs. control. 288 • APRIL 2005 • www.ajpheart.org H1928 MAP KINASES AND HEART FAILURE AIC, and its activity was increased in a time-dependent manner. Pro- as well as anti-apoptotic proteins Bax and Bcl-xl were detected in both early and late stages of AIC using Western blot analysis, and the data are shown in Fig. 4. The ratio of Bax over Bcl-xl showed a significant increase starting at 4 h after the last injection of ADR and it continued to rise for 3 wk (Fig. 4). DISCUSSION The current study is the first to investigate the MAPK signaling pathways and pro- and anti-apoptotic proteins in both early and late stages of AIC. The major findings are the following: 1) ADR treatment activated all three MAPKs at early time points in the evolution of cardiomyopathy; 2) phosphorylation of ERK1/2 was upregulated at early time points, followed by a decline in the heart failure stage; 3) phosphorylation of P38 and JNK MAPKs was elevated at all time points during the progression of heart failure; 4) antioxidant probucol modulated the phosphorylation of all three MAPKs, indicating the activation of MAPKs through oxidative stress; and 5) myocardial proapoptotic proteins were activated in both early and late stages of AIC, which were shown as the activation of caspase-3 and increase in the ratio of Bax to Bcl-xl. MAPKs in ADR-induced heart failure. Myocardial MAPKs have been examined extensively in heart failure patients; however, there is a significant variance in the information reported. In this regard, activities of all three MAPKs were reported to be elevated in human patients with heart failure due to ischeFig. 2. A–C: effects of ADR with and without probucol (Pro) on the activity of MAPKs, ERK1/2 (A), p38 (B), and JNKs (C) in ADR-induced heart failure. UP, myocardial phosphorylated MAP kinases were measured by Western blot analysis with phospho-specific MAPKs antibody. Total amount of MAP kinases were examined from the same stripped membrane for each MAP kinase with the kinase-specific antibodies. LP, densitometric analysis of MAP kinase activation. Values are the ratio of phospho-specific MAP kinases to total MAP kinases. Results were normalized for all experiments by a random setting of the densitometer of the control heart samples as 100%. Data in the LP are means ⫾ SE from 4 hearts in independent experiments. *P ⬍ 0.05 vs. control; #P ⬍ 0.05 vs. ADR. AJP-Heart Circ Physiol • VOL 288 • APRIL 2005 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.4 on June 16, 2017 Fig. 3. Time course (1 h, 2 h, 4 h, 24 h, and 3 wk) of activation of caspase-3 in AIC. UP, myocardial caspase-3 was measured by Western blot analysis with cleaved caspase-3 antibody, and the same stripped membrane was examined with caspase-3 antibody. LP, densitometry analysis of caspase-3 activation. Values are the ratio of cleaved caspase-3 to full length of caspase-3. Results were normalized by setting the densitometer of the control samples as 100%. MAP KINASES AND HEART FAILURE mic cardiomyopathy and idiopathic dilated cardiomyopathy (8). In another study, only the activities of JNK and p38 were reported to be increased, whereas ERK1/2 had no change in heart failure due to ischemic heart disease (7). In contrast, decreased activity of p38 was reported in the failing myocardium from ischemic and idiopathic dilated cardiomyopathy (14). These are a few examples from many suggesting that MAPKs may be differentially regulated. Thus an unique balance among MAPKs pathways may exist, depending on the stage of heart failure as well as the types of the stimulus. A study of the time course of changes in MAPKs during the pathogenesis of heart failure, such as is done in this study, is important to sketch a comprehensive picture. Our data show that ERK1/2 was activated early but transiently and downregulated during the heart failure stage. The early upregulation may have been an adaptive and protective response. In contrast, phosphorylation of p38 and JNKs kinases increased early and persisted until the heart failure stage, suggesting that these kinases may play a dominant role in the progression of AIC and heart failure. MAPKs and ADR-induced oxidative stress. It has been well documented that oxidative stress activates MAPKs. In the perfused rat heart and cultured cardiomycytes, H2O2 activated all three MAPKs (1, 3, 19). N-(2-mercaptopropionyl)-glycine, DMSO, and catalase, but not SOD, markedly depressed daunomycin-mediated activation of MAPKs, suggesting that ⫺OH and H2O2, but not O⫺ 2 are mainly involved in the activation of MAPKs (30). All three MAPKs were also reported to be activated in ischemia-reperfusion injury, mediated by oxidative stress (20). It is widely accepted that ADR induces cardiomyopathy by producing reactive oxygen species as well as by decreasing the antioxidant reserve (2). In our previous report, with the use of the same AIC model, lipid peroxidation occurred as early as 1 h and continued to increase up to 24 h, and there was a corresponding decrease in glutathione peroxidase and MnSOD activities (15). In the present study, antioxidant probucol markedly modulated ADR-induced changes in the phosphorylation of all three MAPKs, indicating that the ADRAJP-Heart Circ Physiol • VOL induced activation of MAPKs may also be modulated through increased oxidative stress. MAPKs and ADR-induced apoptosis. Isolated rat cardiomyocytes exposed to ADR showed the occurrence of apoptosis in terminal deoxynucleotidyl transferase-mediated dUTP nickend labeling assay, DNA laddering, and electron microscopic evaluation (2, 9, 10). Time-dependent apoptosis was also observed in ADR-treated rats at a cumulative dose of 15 mg/kg. The data revealed a biphasic response of apoptosis, peaking at 4 and 21 days after ADR treatment (11). It is also reported that apoptosis occurred in both cardiomyocytes and endothelial cells in ADR-treated rats at a cumulated dose of 24 mg/kg for over 2 wk (29). Even a single dose of ADR at 15 mg/kg also induced apoptosis in the mice (9). In the current study, activation of caspase-3 as well as the increase in the ratio of Bax to Bcl-xl were shown in both early AIC and heart failure. These changes were preceded as well as accompanied by the activation of p38 and JNK kinases. These MAPKs have been indicated to mediate death signaling pathways in response to ischemia-reperfusion, oxidative stress, hypoxia, and -adrenergic stimulation (4). ERK1/2 and p38 kinases were reported to play an opposite role in daunomycin-induced apoptosis. Inhibition of ERK1/2 activation was demonstrated to increase daunomycin-induced apoptosis, whereas p38 inhibitor reduced the numbers of apoptotic cells (30). On the basis of the results obtained from the present study as well as existing reports, it is suggested that MAPKs play an important role in the ADR-induced apoptosis. It was surprising to note that p38 mRNA expression was downregulated while its activity was increased. It is likely that there exists a highly differentiated p38 pathways that is mediated by different isoforms of the p38 MAPKs. For example, the p38␣ isoform was shown to play an important role in the induction of apoptosis, whereas p38 was capable of inducing a typical hypertrophic response in cardiomyocytes (3, 9, 27). Because cardiomyocyte apoptosis is shown to be induced in the AIC, it is possible that in the heart failure stage of AIC, p38 mRNA expression was decreased due to the downregulation of the p38 isoform, whereas p38␣ may not change or may even increase. However, when the phosphorylation of p38 was detected, p38␣ may be the dominant isoform in the determination of the p38 activity. The possibility of posttranslational changes and/or reduced degradation of this protein kinase cannot be excluded. Apart from inducing apoptosis, the activation of caspase-3 in the heart has also been reported to result in depressed cardiac function, myofibril disruption, and sarcomere disorganization through its ability to cleave cardiac myofibrillar proteins, such as ventricular myosin light chain, ␣-actin, ␣-actinin, and troponin T (6, 18). Therefore, the activation of apoptotic signaling proteins may mediate both cardiac dysfunction and apoptosis in the progression of AIC. In conclusion, the present study suggests that ADR-induced oxidative stress may stimulate MAPKs signaling pathways, leading to activation of proapoptotic proteins, myocardial apoptosis, and progression of heart failure. Exploring the potential for modulating MAPK pathways would likely result in novel approaches to prevent or treat AIC and heart failure. 288 • APRIL 2005 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.4 on June 16, 2017 Fig. 4. Time course of the ratio of Bax to Bcl-xl in the AIC. UP, myocardial Bax and Bcl-xl proteins were measured by Western blot analysis with their specific antibodies. Two proteins were detected from the same stripped membrane. LP, densitometry analysis of Bax and Bcl-xl. Values are the ratio of Bax to Bcl-xl normalized by setting the densitometer of the control samples as 100%. H1929 H1930 MAP KINASES AND HEART FAILURE GRANTS The study was supported by the Canadian Institutes of Health Research and the Heart and Stroke Foundation of Manitoba (Interdisciplinary Health Research Team on Gene Environment). H. Lou is supported by a student fellowship from the University of Manitoba. I. Danelisen is supported by the student fellowship from the Heart and Stroke Foundation of Canada. REFERENCES AJP-Heart Circ Physiol • VOL 288 • APRIL 2005 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.4 on June 16, 2017 1. Aikawa R, Komuro I, Yamazaki T, Zou Y, Kudoh S, Tanaka M, Shiojima I, Hiroi Y, and Yazaki Y. Oxidative stress activates extracellular signal-regulated kinases through Src and Ras in cultured cardiac myocytes of neonatal rats. J Clin Invest 100: 1813–1821, 1997. 2. Arola OJ, Saraste A, Pulkki K, Kallajoki M, Parvinen M, and Voipio-Pulkki LM. Acute doxorubicin cardiotoxicity involves cardiomyocyte apoptosis. Cancer Res 60: 1789 –1792, 2000. 3. Bogoyevitch MA, Gillespie-Brown J, Ketterman AJ, Fuller SJ, Ben Levy R, Ashworth A, Marshall CJ, and Sugden PH. Stimulation of the stress-activated mitogen-activated protein kinase subfamilies in perfused heart. p38/RK mitogen-activated protein kinases and c-Jun N-terminal kinases are activated by ischemia/reperfusion. Circ Res 79: 162–173, 1996. 4. Bueno OF and Molkentin JD. Involvement of extracellular signalregulated kinases 1/2 in cardiac hypertrophy and cell death. Circ Res 91: 776 –781, 2002. 5. Clerk A, Michael A, and Sugden PH. Stimulation of multiple mitogenactivated protein kinase sub-families by oxidative stress and phosphorylation of the small heat shock protein, HSP25/27, in neonatal ventricular myocytes. Biochem J 333: 581–589, 1998. 6. Communal C, Sumandea M, de Tombe P, Narula J, Solaro RJ, and Hajjar RJ. Functional consequences of caspase activation in cardiac myocytes. Proc Natl Acad Sci USA 99: 6252– 6256, 2002. 7. Cook SA, Sugden PH, and Clerk A. Activation of c-Jun N-terminal kinases and p38-mitogen-activated protein kinases in human heart failure secondary to ischaemic heart disease. J Mol Cell Cardiol 31: 1429 –1434, 1999. 8. Haq S, Choukroun G, Lim H, Tymitz KM, del Monte F, Gwathmey J, Grazette L, Michael A, Hajjar R, Force T, and Molkentin JD. Differential activation of signal transduction pathways in human hearts with hypertrophy versus advanced heart failure. Circulation 103: 670 – 677, 2001. 9. Kang YJ, Zhou ZX, Wang GW, Buridi A, and Klein JB. Suppression by metallothionein of doxorubicin-induced cardiomyocyte apoptosis through inhibition of p38 mitogen-activated protein kinases. J Biol Chem 275: 13690 –13698, 2000. 10. Kumar D, Kirshenbaum L, Li T, Danelisen I, and Singal P. Apoptosis in isolated adult cardiomyocytes exposed to adriamycin. Ann NY Acad Sci 874: 156 –168, 1999. 11. Kumar D, Kirshenbaum LA, Li T, Danelisen I, and Singal PK. Apoptosis in adriamycin cardiomyopathy and its modulation by probucol. Antioxid Redox Signal 3: 135–145, 2001. 12. Kyriakis JM and Avruch J. Sounding the alarm: protein kinase cascades activated by stress and inflammation. J Biol Chem 271: 24313–24316, 1996. 13. Lefrak EA, Pitha J, Rosenheim S, and Gottlieb JA. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer 32: 302–314, 1973. 14. Lemke LE, Bloem LJ, Fouts R, Esterman M, Sandusky G, and Vlahos CJ. Decreased p38 MAPK activity in end-stage failing human myocardium: p38 MAPK alpha is the predominant isoform expressed in human heart. J Mol Cell Cardiol 33: 1527–1540, 2001. 15. Li T, Danelisen I, and Singal PK. Early changes in myocardial antioxidant enzymes in rats treated with adriamycin. Mol Cell Biochem 232: 19 –26, 2002. 16. Li T and Singal PK. Adriamycin-induced early changes in myocardial antioxidant enzymes and their modulation by probucol. Circulation 102: 2105–2110, 2000. 17. Lou H, Danelisen I, and Singal PK. Cytokines are not upregulated in adriamycin-induced cardiomyopathy and heart failure. J Mol Cell Cardiol 36: 683– 690, 2004. 18. Moretti A, Weig HJ, Ott T, Seyfarth M, Holthoff HP, Grewe D, Gillitzer A, Bott-Flugel L, Schomig A, Ungerer M, and Laugwitz KL. Essential myosin light chain as a target for caspase-3 in failing myocardium. Proc Natl Acad Sci USA 99: 11860 –11865, 2002. 19. Sabri A, Byron KL, Samarel AM, Bell J, and Lucchesi PA. Hydrogen peroxide activates mitogen-activated protein kinases and Na⫹-H⫹ exchange in neonatal rat cardiac myocytes. Circ Res 82: 1053–1062, 1998. 20. Sawyer DB, Siwik DA, Xiao L, Pimentel DR, Singh K, and Colucci WS. Role of oxidative stress in myocardial hypertrophy and failure. J Mol Cell Cardiol 34: 379 –388, 2002. 21. Sheng Z, Knowlton K, Chen J, Hoshijima M, Brown JH, and Chien KR. Cardiotrophin 1 (CT-1) inhibition of cardiac myocyte apoptosis via a mitogen-activated protein kinase-dependent pathway. Divergence from downstream CT-1 signals for myocardial cell hypertrophy. J Biol Chem 272: 5783–5791, 1997. 22. Singal PK and Iliskovic N. Doxorubicin-induced cardiomyopathy. N Engl J Med 339: 900 –905, 1998. 23. Siveski-Iliskovic N, Kaul N, and Singal PK. Probucol promotes endogenous antioxidants and provides protection against adriamycin-induced cardiomyopathy in rats. Circulation 89: 2829 –2835, 1994. 24. Sugden PH and Bogoyevitch MA. Intracellular signalling through protein kinases in the heart. Cardiovasc Res 30: 478 – 492, 1995. 25. Sugden PH and Clerk A. “Stress-responsive” mitogen-activated protein kinases (c-Jun N-terminal kinases and p38 mitogen-activated protein kinases) in the myocardium. Circ Res 83: 345–352, 1998. 26. Wang X, Martindale JL, Liu Y, and Holbrook NJ. The cellular response to oxidative stress: influences of mitogen-activated protein kinase signalling pathways on cell survival. Biochem J 333: 291–300, 1998. 27. Wang Y, Huang S, Sah VP, Ross J Jr, Brown JH, Han J, and Chien KR. Cardiac muscle cell hypertrophy and apoptosis induced by distinct members of the p38 mitogen-activated protein kinase family. J Biol Chem 273: 2161–2168, 1998. 28. Wang Y, Su B, Sah VP, Brown JH, Han J, and Chien KR. Cardiac hypertrophy induced by mitogen-activated protein kinase kinase 7, a specific activator for c-Jun NH2-terminal kinase in ventricular muscle cells. J Biol Chem 273: 5423–5426, 1998. 29. Wu S, Ko YS, Teng MS, Ko YL, Hsu LA, Hsueh C, Chou YY, Liew CC, and Lee YS. Adriamycin-induced cardiomyocyte and endothelial cell apoptosis: in vitro and in vivo studies. J Mol Cell Cardiol 34: 1595–1607, 2002. 30. Zhu W, Zou Y, Aikawa R, Harada K, Kudoh S, Uozumi H, Hayashi D, Gu Y, Yamazaki T, Nagai R, Yazaki Y, and Komuro I. MAPK superfamily plays an important role in daunomycin-induced apoptosis of cardiac myocytes. Circulation 100: 2100 –2107, 1999.