Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Baker Heart and Diabetes Institute wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
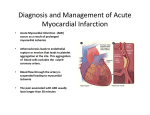
Myocardial Infarction Ischemic heart muscle necrosis. significant cause of death worldwide. 33% -50% die before they can reach the hospital lethal arrhythmia Sudden Cardiac Death Arrhythmias are caused by electrical abnormalities of ischemic myocardium and conduction system. 1 • Most common coronary involved is proximal left anterior descending (LAD) artery (40% to 50% of all MI). infarction of anterior wall of left ventricle + anterior two thirds of the ventricular septum + heart apex 2 frequency of MIs rises with increasing age and presence of other risk factors such as hypertension, smoking, and diabetes. 10% of MIs occur in people younger than 40 years. 3 4 Clinical Features of MI 1) Severe, crushing substernal chest pain radiating to neck, jaw, epigastrium, or left arm. • MI can be entirely asymptomatic in 10% to 15% (silent infarcts) common in: 1- diabetes mellitus (peripheral neuropathies) 2- in the elderly 2- rapid and weak pulse. 5- nausea (posterior-MI). 6- cardiogenic shock (massive MI >40% of left ventricle) 7- dyspnea (impaired myocardial contractility & dysfunction of mitral valvepulmonary congestion and edema). Evaluation of MI • Clinical signs and symptoms • Electrocardiographic(ECG) abnormalities • Laboratory evaluation: - blood levels of molecules leaking out of injured myocardial cells through damaged cell membranes. 9 Cardiac enzymes in MI • These molecules include : 1- myoglobin. 2- cardiac troponins T and I (TnT, TnI): the best markers for acute MI. 3- creatine kinase (CK, specifically myocardial-specific isoform= CK-MB) 4- lactate dehydrogenase 10 Microscopic changes of MI and its repair. (<24 hr) coagulative necrosis and wavy fibers. 2- to 3-day old - infarct Dense neutrophil infiltrate (7 to 10 days) phagocytic macrophages removal of necrotic myocytes up to 14 days Granulation tissue. several weeks dense collagenous scar. 11 Microscopic features of myocardial infarction and its repair (detailed) . (<24 hr) coagulative necrosis and wavy fibers Necrotic cells are separated by edema fluid 12 Microscopic features of myocardial infarction and its repair. (detailed) 2- to 3-day old infarct Dense neutrophil infiltrate 13 Microscopic features of myocardial infarction and its repair. (detailed) 7 to 10 days) complete removal of necrotic myocytes by phagocytic macrophages 14 Microscopic features of myocardial infarction and its repair. up to 14 days Granulation tissue = loose connective tissue (blue) and abundant capillaries (red) 15 Microscopic features of myocardial infarction and its repair. several weeks Healed myocardial infarct consisting of a dense collagenous scar (blue) 16 Consequences and Complications of MI 1- Death: 50% of the deaths: pts never reach the hospital (due to arrhythmias) 17 Consequences and Complications of MI (cont.): 2- cardiogenic shock. - (10% to 15%) after acute MI - large infarcts ( >40% of Left ventricle). - 70% mortality rate; (2/3 of in-hospital deaths). 18 Consequences and Complications of MI (cont.): 3-Myocardial rupture Complications of myocardial rupture include: (1) rupture of free wall hemopericardium & cardiac tamponade (usually fatal) (2) rupture of septum VSD and left-to-right shunt (3) papillary muscle rupture severe mitral regurgitation 19 myocardial rupture 20 Consequences and Complications of MI (cont.): 4-Pericarditis. - 2 to 3 days post-transmural MI - spontaneously resolves with time - immunologic mechanism. 5-Infarct expansion. - stretching, thinning, and dilation of the infarct region 21 Consequences and Complications of MI (cont.): 6-Mural thrombus. -local loss of contractility (stasis) + endocardial damage 7-Ventricular aneurysm. - A late complication - large infarct heals with the formation of thin scar tissue 22 Ventricular aneurysm Complications of ventricular aneurysms include: 1-mural thrombus 2-arrhythmias 3-heart failure 23 Consequences and Complications of MI (cont.): 8-Papillary muscle dysfunction (postinfarct mitral regurgitation ) 9-Progressive late heart failure 24 Long-term prognosis after MI depends on many factors, the most important of which are: - left ventricular function - severity of atherosclerosis of remaining viable myocardium. Mortality rate within the first year =30% • Thereafter, the annual mortality rate is 3% 25 Chronic Ischemic Heart Disease • post-infarction cardiac decompensation • exhaustion of the hypertrophic viable myocardium = progressive heart failure (CHF) 26 Sudden Cardiac Death (SCD) • Definition: unexpected death from cardiac causes either without symptoms or within 1 to 24 hours of symptom onset . • The most common mechanism is ventricular fibrillation (arrythmia). • The most common underlying cause is Coronary artery disease • With younger victims, other non-atherosclerotic causes are more common: 27 Other non-atherosclerotic causes of SCD • • • • • • • Congenital coronary arterial abnormalities Aortic valve stenosis Mitral valve prolapse Myocarditis Dilated or hypertrophic cardiomyopathy Pulmonary hypertension Hereditary or acquired abnormalities of the cardiac conduction system. • Isolated myocardial hypertrophy. • unknown ??. 28