Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DNA vaccination wikipedia , lookup
Common cold wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Vaccination policy wikipedia , lookup
Marburg virus disease wikipedia , lookup
Herd immunity wikipedia , lookup
West Nile fever wikipedia , lookup
Immunocontraception wikipedia , lookup
Hepatitis B wikipedia , lookup
Henipavirus wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Globalization and disease wikipedia , lookup
Non-specific effect of vaccines wikipedia , lookup
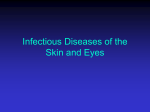
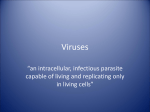
SUPPLEMENT ARTICLE Biological Feasibility of Measles Eradication William J. Moss1 and Peter Strebel2 1Department of Epidemiology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; and 2World Health Organization, Geneva, Switzerland Recent progress in reducing global measles mortality has renewed interest in measles eradication. Three biological criteria are deemed important for disease eradication: (1) humans are the sole pathogen reservoir; (2) accurate diagnostic tests exist; and (3) an effective, practical intervention is available at reasonable cost. Interruption of transmission in large geographical areas for prolonged periods further supports the feasibility of eradication. Measles is thought by many experts to meet these criteria: no nonhuman reservoir is known to exist, accurate diagnostic tests are available, and attenuated measles vaccines are effective and immunogenic. Measles has been eliminated in large geographical areas, including the Americas. Measles eradication is biologically feasible. The challenges for measles eradication will be logistical, political, and financial. Measles elimination refers to the interruption of measles virus transmission within a defined geographic area, such as country, continent, or World Health Organization region, whereas measles eradication is the global interruption of measles virus transmission such that control efforts could be stopped. The feasibility of measles eradication has been discussed for more than 30 years, beginning in the late 1960s when the long-term protective immunity induced by measles vaccines was becoming evident [1]. Three biological criteria are deemed important for disease eradication: (1) humans are the sole pathogen reservoir; (2) accurate diagnostic tests exist; and (3) an effective, practical intervention is available at reasonable cost [2]. Interruption of transmission in large geographical areas for prolonged periods further supports the feasibility of eradication. Measles is thought by many experts to meet these criteria [3]. In this article, we review the biological feasibility of measles eradication and consider potential biological obstacles to eradication. Potential conflicts of interest: none reported. Supplement sponsorship: This article is part of a supplement entitled ''Global Progress Toward Measles Eradication and Prevention of Rubella and Congenital Rubella Syndrome,'' which was sponsored by the Centers for Disease Control and Prevention. Correspondence: William J. Moss, MD, MPH, Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, 615 North Wolfe Street, Baltimore, MD 21205 ([email protected]). The Journal of Infectious Diseases 2011;204:S47–S53 Ó The Author 2011. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected] 0022-1899 (print)/1537-6613 (online)/2011/204S1-0008$14.00 DOI: 10.1093/infdis/jir065 ARE HUMANS THE ONLY RESERVOIR FOR MEASLES VIRUS? Measles virus infection is presumed to be sustained through an unbroken chain of human-to-human transmission, and no animal or environmental reservoir is known to exist. However, nonhuman primates can be infected with measles virus and can develop an illness similar to measles in humans with rash, coryza, and conjunctivitis. Many primate species are susceptible to measles virus infection, including Macaca mulatta, M. fascicularis, M. radiata, M. cyclopis, Papio cristatus, Cercopithecus aethiops, Saimiri sciureus, Colobus quereza, Pan troglodytes, Callithrix jacchus, Saguinus oedipus, S. fuscicollis, and Aotus trivirgatus [4]. Much of the evidence for the susceptibility of these nonhuman primates comes from laboratory colonies and the use of nonhuman primates as animal models for the study of measles virus pathogenesis. Interestingly, serological studies have demonstrated evidence of prior measles virus infection in free-ranging populations of nonhuman primates, outside of laboratory colonies. One-fourth of 47 Rhesus macaques in southern India [5] and one-third of 15 wild macaques in Indonesia had serological evidence of measles virus infection [6]. Presumably, measles virus infection resulted from human-to-animal transmission, perhaps followed by limited spread within the primate population. Justification for the conclusion that wild primate populations do not serve as natural reservoirs is based on the Biological Feasibility of Measles Eradication d JID 2011:204 (Suppl 1) d S47 critical population size necessary to sustain transmission of highly infectious measles virus. To provide a sufficient number of new susceptibles through births to maintain measles virus transmission in humans, a population size of several hundred thousand persons with 5000–10,000 births per year is required [7]. If measles virus is as infectious in primates, wild populations of up to several hundred individuals [8] are not of sufficient size. ARE THERE ACCURATE DIAGNOSTIC TESTS FOR MEASLES? Several diagnostic tests for measles exist, although some are limited by low positive predictive value in low transmission settings [9]. Measles is readily diagnosed by clinicians familiar with the disease in endemic areas or during outbreaks, but clinical diagnosis is more difficult when incidence is low. In low-transmission settings, other pathogens or inflammatory reactions are responsible for the majority of illnesses with fever and rash. Koplik spots are especially helpful because they appear early and are pathognomonic, but with the declining incidence of measles fewer clinicians can recognize them. The rash of measles may be absent or delayed in immunocompromised or severely malnourished children with impaired cellular immunity, also impeding clinical diagnosis. Serology is the most commonly used method of laboratory diagnosis. The detection of measles virus-specific immunoglobulin M (IgM) antibodies in a single specimen of serum or oral fluid is considered diagnostic of acute infection, as is a 4-fold or greater increase in measles virus-specific immunoglobulin G (IgG) antibodies between acute and convalescent serum samples. Measles virus-specific IgM antibodies may not be detectable until 4 days after rash onset and usually fall to undetectable concentrations within 4–8 weeks. Measles also can be confirmed by isolating measles virus in cell culture from respiratory secretions, nasopharyngeal and conjunctival swabs, blood, or urine. Although Vero cells are commonly used for neutralization tests using laboratory-adapted measles virus strains, a derivative (B95-a) of the Epstein-Barr virus-transformed marmoset B lymphocyte cell line B95-8 has greater sensitivity than Vero cells for the isolation of wild-type strains of measles virus. Expression of the measles virus receptor CD150 (SLAM) on Vero cells enhances the ability to isolate wild-type measles virus strains in tissue culture. Detection of measles virus RNA by reverse transcriptase-PCR (RT-PCR) amplification of RNA extracted from clinical specimens can be accomplished using primers targeted to highly conserved regions of measles virus genes. When combined with nucleotide sequencing, these assays permit the precise identification and characterization of measles virus genotypes for molecular epidemiological studies and can distinguish wild-type and vaccine measles virus strains. However, measles virus RNA may persist for several months in both healthy and S48 d JID 2011:204 (Suppl 1) d Moss and Strebel immunocompromised children [10] and under experimental conditions in macaques [11]. Consequently, detection of measles virus RNA does not necessarily indicate acute infection. Limitations of current diagnostic tests for measles, specifically IgM enzyme immunoassays (EIAs), are the potential for both false negative and false positive results. Concentrations of IgM antibodies may be low during the first three days of the rash, resulting in false negative test results [12]. False positive results may occur in the presence of rheumatoid factor and certain viral coinfections, including rubella, parvovirus B19, and human herpes virus 6. In addition, laboratory testing is usually only performed on suspected cases; thus, persons with uncharacteristic or minimal signs or symptoms may be missed. Although these limitations may pose challenges to the diagnosis of measles in certain individuals, available diagnostic tests are unlikely to miss measles outbreaks or sustained measles virus transmission. ARE THERE EFFECTIVE INTERVENTIONS FOR MEASLES? Two broad approaches have been used to measure the effectiveness of measles vaccines: the effectiveness of measles vaccines in preventing clinical measles and measurement of vaccine immunogenicity. Measles vaccine effectiveness has been evaluated in numerous studies. A review of 69 published studies of measles vaccine effectiveness from 1969 to 2006 found an overall estimate of measles vaccine effectiveness of 90% [13]. Median measles vaccine effectiveness was estimated to be 77% when administered between 9 and 11 months of age, and 92% when administered at 12 months or older. These findings are consistent with immunogenicity studies. Measles vaccine immunogenicity is commonly assessed by measuring IgG antibodies to measles virus. Antibodies first appear between 12 and 15 days after vaccination and typically peak at 21–28 days. The protective efficacy of antibodies to measles virus is illustrated by protection conferred to infants from passively acquired maternal antibodies and the protection of exposed, susceptible individuals following administration of anti-measles virus immunoglobulin. Consequently, antibody concentrations serve as useful surrogate markers of protection [14], despite the fact that cell-mediated immunity is important for viral clearance [15]. The proportion of children who develop protective antibody concentrations following measles vaccination depends on the presence of inhibitory maternal antibodies and the immunologic maturity of the vaccine recipient, as well as the dose and strain of vaccine virus. Frequently cited figures are that 85% of children develop protective antibody concentrations when given 1 dose of measles vaccine at 9 months of age, and 90%–95% respond when vaccinated at 12 months of age [16]. In a review of measles vaccine immunogenicity (Figure 1) [17], the median proportion Figure 1. Box plots showing the proportion of children who respond to standard-titer measles vaccine by age at vaccination. Source: Moss WJ, Scott S. WHO Immunological Basis for Immunization Series: Measles. Geneva, Switzerland: World Health Organzation, 2009. of children responding was 89.6% (mean, 86.7; minimum, 56; maximum, 100; interquartile range [IQR], 82–95) in 44 studies in which children were vaccinated between 8 and 9 months of age; 92.2% (mean, 88.2; minimum, 59; maximum, 100; IQR 84–96) in 24 studies in which children were vaccinated between 9 and 10 months of age; and 99% (mean, 95.7; minimum, 80; maximum, 100; IQR, 93–100) in 21 studies in which children were vaccinated between 11 and 12 months of age. Several biological factors determine measles vaccine effectiveness and immunogenicity. Age at vaccination is the most important determinant. Antibody responses to measles vaccine increase with age up to 15 months, due to the presence of inhibitory maternal antibodies and immaturity of the immune system. This immaturity of the immune system in neonates and young infants includes a limited B cell repertoire and inefficient mechanisms of antigen presentation and T cell help [18]. Although protective, maternally acquired antibodies interfere with the immune responses to the attenuated measles vaccine by inhibiting replication of vaccine virus necessary for an effective immune response. In general, maternally acquired antibodies are no longer present in the majority of children by 6–9 months of age [19]. A few studies suggest that concurrent acute infections may interfere with the immune response to measles vaccine [20], although many studies reported no effect and mild illnesses are not a contraindication to measles vaccination. Most published studies found that malnourished children have equivalent seroconversion rates after measles vaccination compared with children who are well nourished. Host genetic background affects the likelihood of developing protective immune responses following measles vaccination. Polymorphisms in human immune response genes influence immune responses to measles vaccine, including class I and class II human leukocyte antigen (HLA) types and non-HLA alleles [21]. Single-nucleotide polymorphisms (SNPs) in cytokine and cytokine receptor genes, as well as SNPs in the measles virus receptors (SLAM and CD46), also were associated with differences in antibody and cellular immune responses to measles vaccine. However, in general, most people develop protective antibody concentrations after a second dose of measles vaccine, regardless of genetic background. Measles virus transmission can be interrupted by achieving high levels of population immunity with measles vaccines, such that the probability of an infected case coming in contact with a susceptible individual is low [22]. However, a 2-dose measles immunization schedule is necessary to achieve the 95% population immunity necessary to interrupt measles virus transmission. This can be readily understood by the fact that 95% vaccine coverage with a vaccine providing protection to 95% of recipients only achieves 90% population immunity. Two strategies to administer the second dose of measles vaccine are through routine immunization services or mass immunization campaigns (called supplementary immunization activities), an approach first developed by the Pan American Health Organization (PAHO) for South and Central America and modeled after polio eradication strategies. Attenuated measles vaccines have some characteristics that limit their effectiveness or increase their risk-benefit ratio in some populations. First, these vaccines are not immunogenic in young infants, necessitating vaccine administration at 9 months of age or older. Second, measles vaccines are relatively heatstable in the lyophilized form but rapidly lose potency when exposed to heat after reconstitution, potentially reducing effectiveness if improperly stored. Third, live viral vaccines are potentially harmful to immunocompromised persons and may cause disease as a result of vaccine virus replication [23]. A recent systematic review concluded that measles vaccines appear to be safe in children infected with human immunodeficiency virus (HIV), but there is an absence of studies reporting relevant information [24]. Despite these limitations, the attenuated measles vaccines currently used have a history of proven safety and effectiveness over the past 40 years and have resulted in dramatic reductions in measles incidence, morbidity, and mortality (Figure 2). IS THERE EVIDENCE OF SUSTAINED INTERRUPTION OF MEASLES VIRUS TRANSMISSION IN LARGE GEOGRAPHIC AREAS? Measles elimination was achieved in the United States in 2000 and in the Americas by November 2002 [25]. Small outbreaks of primary and secondary cases may occur following importation from outside the region but sustained transmission does not occur, as exemplified by recent measles outbreaks in the United Biological Feasibility of Measles Eradication d JID 2011:204 (Suppl 1) d S49 described. Thus, there is no evidence for persistent shedding of infectious measles virus. Sustained Transmission Through Subclinical Infection Figure 2. Estimated number of measles deaths worldwide, 2000–2008. Adapted from Weekly Epidemiological Record 2009;85:513. States [26]. Four other World Health Organization (WHO) regions have set measles elimination goals: African, Eastern Mediterranean, Europe, and Western Pacific. The remaining WHO region, South-East Asia, has a goal to reduce measles mortality by 90% by 2010 compared with 2000 levels. These ambitious goals have resulted in part from successful implementation of the WHO/UNICEF strategy of providing the second dose of measles vaccine through supplementary immunization activities, resulting in dramatic declines in incidence and mortality (Figure 1). The largest recent decrease in measles mortality was in Africa, where measles mortality decreased 91% from 2000–2006, accounting for 70% of the global reduction in measles mortality [27]. POTENTIAL BIOLOGICAL BARRIERS TO MEASLES ERADICATION Persistent Human Reservoirs Persistent infection with transmissible measles virus would pose a biological barrier to eradication. Measles virus is known to establish persistent infection in persons with subacute sclerosing panenephalitis (SSPE). SSPE is a rare delayed complication of measles that occurs in 1:100,000 to 1:10,000 cases [28], typically 6–8 years after acute measles in the first 2 years of life. Neurons and glial cells contain typical measles virus nuclear and cytoplasmic inclusion bodies. However, virion assembly and budding is defective, and multiple mutations occur throughout the measles virus genome, especially hypermutations within the M gene and alterations in the H and F genes. As a consequence, infectious measles virus is not present. Prolonged shedding of measles virus RNA for several months has been described in HIV-infected children [29], although it is not clear if this represents infectious virions and a prolongation of the period of infectivity. Transmission of measles vaccine virus has not been S50 d JID 2011:204 (Suppl 1) d Moss and Strebel As diagnostic tests for acute measles virus infection are most often performed on clinically suspected cases, subclinical infection resulting in sustained measles virus transmission would pose a barrier to eradication. Subclinical measles is defined as a 4-fold rise in measles virus-specific IgG antibodies following exposure to wild-type measles virus in an asymptomatic individual, presumably with some prior measles immunity. Subclinical infection may be important in boosting protective antibody concentrations in children with waning immunity [30] but raises a concern that persons with incomplete immunity and subclinical infection may be capable of transmitting measles virus [31]. In an investigation of potential measles virus shedding from persons with subclinical infection, measles virus was not detected by culture or reverse transcriptase-polymerase chain reaction from any of 133 contacts of 6 subclinical cases with laboratory-confirmed measles [32]. Whether partially immune individuals with subclinical infection can sustain measles virus transmission in the absence of clinical cases is unlikely. Waning Vaccine Immunity If vaccine induced immunity is short-lived, revaccination efforts would need to be enhanced to maintain the high levels of population immunity required for measles eradication. Although the duration of immunity following measles vaccination is more variable and shorter than following wild-type measles virus infection, protective immunity persists for decades even in countries where measles is no longer endemic and immunological boosting from wild-type measles virus infection does not occur [33]. The purpose of a 2-dose schedule for measles vaccination is to immunize children with primary vaccine failure (as well as those previously unvaccinated) and not to serve as a booster dose for persons with waning immunity. Furthermore, although antibody concentrations induced by vaccination may decline over time and become undetectable, immunological memory persists and vaccinated persons produce an anamnestic measles virus-specific immune response following exposure to wild-type measles virus. Thus, waning immunity is unlikely to be a biological barrier to measles eradication. Measles Virus Genetic Diversity Theoretically, selective pressure on measles viruses to mutate neutralizing epitopes and escape the protective immune responses induced by vaccines could be a biological obstacle to measles eradication. Estimates of mutation rates in measles virus range from 1024 to 1023 per nucleotide per year [34]. However, despite the high degree of genetic variation expected of a singlestranded RNA virus, mutations in the measles virus genome have not reduced the protective immunity induced by measles vaccines. Serum specimens from vaccinated persons and from persons naturally infected during the 1950s and 1960s had comparable neutralization titers to vaccine viruses and to more recently isolated wild-type measles viruses, although serum samples from persons infected in the 1990s had higher neutralization titers to the homologous wild-type virus [35]. As an example of how genetic changes have not significantly altered important antigenic epitopes, measles virus isolates from a genotype circulating in the Peoples Republic of China during 1993 and 1994 differed from other wild type viruses by as much as 6.9% in the hemagglutinin (H) gene and 7.0% in the nucleocapsid (N) gene, but did not differ significantly from other wild-type viruses in their anti-H monoclonal antibody binding patterns and were neutralized by human post-vaccination antiserum [36]. Thus, neutralizing epitopes on the H protein are highly conserved among measles virus strains, likely because of functional constraints on the amino acid sequence and tertiary structure of the surface proteins [37]. Measles virus remains a monotypic virus for which protective immunity is induced by vaccine strains first isolated in the 1950’s. Measles Outbreaks in Populations With High Levels of Population Immunity Numerous outbreak investigations highlight the challenges of sustaining measles elimination. Despite very high levels of measles vaccine coverage and population immunity overall, clustering of susceptible persons can lead to outbreaks. In 2005, a 17-year-old girl with measles returned to the United States from Romania and attended a church gathering of over 500 people [38]. Despite 98% measles vaccination coverage in the state of Indiana (among 6th graders), 34 cases of measles resulted, of whom 94% were unvaccinated. Of greater concern is the potential for more sustained transmission of measles virus. A measles outbreak of 94 cases occurred in Quebec, Canada, in 2007 and led to transmission within several unrelated networks of unvaccinated persons, despite an estimated level of population immunity of 95% [39]. No epidemiological link was identified for approximately one-third of laboratory confirmed cases and no source was found for the index case. The ease of global travel allows for measles virus importation and this risk will only be abolished by measles eradication. Impact of the HIV-1 Pandemic In regions of high HIV prevalence, HIV-infected children may play a role in the sustaining measles virus transmission. Children with defective cell-mediated immunity can develop measles without the characteristic rash [40], hampering clinical diagnosis. Children born to HIV-infected mothers have lower concentrations of passively acquired maternal antibodies, increasing susceptibility to measles at an earlier age than children born to uninfected mothers [41, 42], and protective antibody concentrations following vaccination may wane within 2–3 years in many HIV-infected children not receiving antiretroviral therapy [43], creating a potential pool of susceptible children. A study in South Africa found lower levels of vaccine effectiveness among HIV-infected compared with uninfected children, although the number of HIV-infected children studied was small [44]. Thus, population immunity could be reduced in regions of high HIV-1 prevalence despite high levels of measles vaccine coverage. Counteracting the increased susceptibility of HIV-infected children is their high mortality rate, particularly in sub-Saharan Africa, such that these children do not live long enough to build up a sizeable pool of susceptible children [45]. Successful control of measles in the countries of southern Africa suggests that the HIV1 epidemic is not a major barrier to measles control [46], although coinfection with HIV may have exacerbated the large measles outbreaks that occurred in countries of southern and eastern Africa in 2010. This may change with increased access to antiretroviral therapy, which may prolong survival without enhancing protective immunity in the absence of revaccination. Using a dynamic, age-structured mathematical model, the prevalence of measles increased almost one-third after introduction of antiretroviral therapy into a hypothetical population of children with a high prevalence of HIV-1 infection [47]. Potential Use of Measles Virus as an Agent of Bioterrorism The high infectivity of measles virus is a characteristic suitable to a bioterrorist agent, but high levels of measles vaccination coverage throughout the world would protect many persons from the deliberate release of measles virus. Genetic engineering of a measles virus strain that was not neutralized by antibodies induced by the current measles vaccines would likely have reduced infectivity, as suggested by the fact that wild-type measles virus has not mutated to alter neutralizing epitopes. Whether the threat from bioterrorism precludes stopping measles vaccination after eradication is unclear but, at the least, a single-dose rather than a 2-dose measles vaccination strategy could be adopted [48]. RESEARCH NEEDS Much is known about the biological feasibility of measles eradication, specifically the absence of nonhuman reservoirs, the positive predictive value of IgM assays for diagnosis, and the effectiveness and immunogenicity of measles vaccines. However, continued research on biological factors (as well as operational and programmatic research) will be useful to furthering the goal of measles eradication, including the (1) development of a rapid, point-of-care test for measles and rubella that would enable laboratory confirmation of the outbreak in the field and more timely and targeted outbreak response measures; (2) progress towards developing the ideal measles vaccine, which would be inexpensive, safe, heat-stable, immunogenic in neonates or very young infants, and administered as a single dose without needle Biological Feasibility of Measles Eradication d JID 2011:204 (Suppl 1) d S51 or syringe [49]; (3) deeper understanding of the impact of heterogeneities and clustering of susceptibles in sustaining measles virus transmission [50]; and (4) evaluation of existing tools and strategies in the most challenging settings (eg, settings with very high birth rates, large-scale migration, and weak infrastructure). CONCLUSIONS Measles eradication is biologically feasible with available diagnostic assays and vaccines, and elimination has been achieved in large geographical areas. While the major challenges for measles eradication will be logistical, financial, and the garnering of sufficient political will, an active research agenda is needed to refine current tools and strategies. Funding Immunization, Vaccines and Biologicals, World Health Organization (to W. J. M.) and the National Institute of Allergy and Infectious Diseases (grant number AI070018 to W. J. M.). References 1. Sencer DJ, Dull HB, Langmuir AD. Epidemiologic basis for eradication of measles in 1967. Public Health Rep 1967; 82:253–6. 2. The eradication of infectious diseases (Report of the dahlem workshop on the eradication of infectious diseases, Berlin, March 16–22, 1997). New York: Wiley, 1998. 3. Orenstein WA, Strebel PM, Papania M, Sutter RW, Bellini WJ, Cochi SL. Measles eradication: is it in our future? Am J Public Health 2000; 90:1521–5. 4. Jones-Engel L, Engel GA, Schillaci MA, et al. Considering humanprimate transmission of measles virus through the prism of risk analysis. Am J Primatol 2006; 68:868–79. 5. Bhatt PN, Brandt CD, Weiss R, Fox JP, Shaffer MF. Viral infections of monkeys in their natural habitat in southern India. II. Serological evidence of viral infection. Am J Trop Med Hyg 1966; 15:561–6. 6. Jones-Engel L, Engel GA, Schillaci MA, Babo R, Froehlich J. Detection of antibodies to selected human pathogens among wild and pet macaques (Macaca tonkeana) in Sulawesi, Indonesia. Am J Primatol 2001; 54:171–8. 7. Black FL. Measles endemicity in insular populations: critical community size and its evolutionary implication. J Theor Biol 1966; 11:207–11. 8. Clutton-Brock TH, Harvey PH. Primate ecology and social organization. J Zoology 1977; 183:1–30. 9. Dietz V, Rota J, Izurieta H, Carrasco P, Bellini W. The laboratory confirmation of suspected measles cases in settings of low measles transmission: conclusions from the experience in the Americas. Bull World Health Organ 2004; 82:852–7. 10. Riddell MA, Moss WJ, Hauer D, Monze M, Griffin DE. Slow clearance of measles virus RNA after acute infection. J Clin Virol 2007; 39:312–7. 11. Pan CH, Valsamakis A, Colella T, et al. Inaugural Article: Modulation of disease, T cell responses, and measles virus clearance in monkeys vaccinated with H-encoding alphavirus replicon particles. Proc Natl Acad Sci U S A 2005; 102:11581–8. 12. Helfand RF, Kebede S, Mercader S, Gary HE Jr., Beyene H, Bellini WJ. The effect of timing of sample collection on the detection of measlesspecific IgM in serum and oral fluid samples after primary measles vaccination. Epidemiol Infect 1999; 123:451–6. S52 d JID 2011:204 (Suppl 1) d Moss and Strebel 13. Uzicanin A. Field effectiveness of measles containing vaccines— literature review. Meeting of the SAGE working group for measles, Geneva, Switzerland, 2009. http://www.who.int/immunization/sage/ 2_Measles_vaccine_effectiveness_Uzicanin.pdf. J Infect Dis. 2011; 203. doi: 10.1093/jid/jir102. 14. Chen RT, Markowitz LE, Albrecht P, et al. Measles antibody: reevaluation of protective titers. J Infect Dis 1990; 162:1036–42. 15. Permar SR, Klumpp SA, Mansfield KG, et al. Role of CD8(1) lymphocytes in control and clearance of measles virus infection of rhesus monkeys. J Virol 2003; 77:4396–400. 16. Cutts FT, Grabowsky M, Markowitz LE. The effect of dose and strain of live attenuated measles vaccines on serological responses in young infants. Biologicals 1995; 23:95–106. 17. Moss WJ, Scott S. WHO immunological basis for immunization series: measles. Geneva, Switzerland: World Health Organzation, 2009. 18. Gans HA, Arvin AM, Galinus J, Logan L, DeHovitz R, Maldonado Y. Deficiency of the humoral immune response to measles vaccine in infants immunized at age 6 months. JAMA 1998; 280:527–32. 19. Caceres VM, Strebel PM, Sutter RW. Factors determining prevalence of maternal antibody to measles virus throughout infancy: a review. Clin Infect Dis 2000; 31:110–9. 20. Krober MS, Stracener CE, Bass JW. Decreased measles antibody response after measles-mumps-rubella vaccine in infants with colds. JAMA 1991; 265:2095–6. 21. Ovsyannikova IG, Pankratz VS, Vierkant RA, Jacobson RM, Poland GA. Human leukocyte antigen haplotypes in the genetic control of immune response to measles-mumps-rubella vaccine. J Infect Dis 2006; 193:655–63. 22. Gay NJ. The theory of measles elimination: implications for the design of elimination strategies. J Infect Dis 2004; 189(Suppl. 1):S2–S35. 23. Moss WJ, Clements CJ, Halsey NA. Immunization of children at risk of infection with human immunodeficiency virus. Bull World Health Organ 2003; 81:61–70. 24. Scott P, Moss WJ, Gilani Z, Low N. Safety and immunogenicity of measles vaccine in HIV-infected children: systematic review and metaanalysis. J Infect Dis 2011; 203. doi: 10.1093/jid/jir071. 25. Orenstein WA, Papania MJ, Wharton ME. Measles elimination in the United States. J Infect Dis 2004; 189(Suppl. 1):S1–S3. 26. Sugerman DE, Barskey AE, Delea MG, et al. Measles outbreak in a highly vaccinated population, San Diego, 2008: Role of the intentionally undervaccinated. Pediatrics 2010; 125:747–55. 27. World Health Organization. Progress in global measles control and mortality reduction, 2000–2006. Wkly Epidemiol Rec 2007; 82:418–24. 28. Bellini WJ, Rota JS, Lowe LE, et al. Subacute sclerosing panencephalitis: more cases of this fatal disease are prevented by measles immunization than was previously recognized. J Infect Dis 2005; 192:1686–93. 29. Permar SR, Moss WJ, Ryon JJ, et al. Prolonged measles virus shedding in human immunodeficiency virus-infected children, detected by reverse transcriptase-polymerase chain reaction. J Infect Dis 2001; 183: 532–8. 30. Whittle HC, Aaby P, Samb B, Jensen H, Bennett J, Simondon F. Effect of subclinical infection on maintaining immunity against measles in vaccinated children in West Africa. Lancet 1999; 353:98–101. 31. Mossong J, Nokes DJ, Edmunds WJ, Cox MJ, Ratnam S, Muller CP. Modeling the impact of subclinical measles transmission in vaccinated populations with waning immunity. Am J Epidemiol 1999; 150:1238–49. 32. Lievano FA, Papania MJ, Helfand RF, et al. Lack of evidence of measles virus shedding in people with inapparent measles virus infections. J Infect Dis 2004; 189(Suppl. 1):S165–S170. 33. Dine MS, Hutchins SS, Thomas A, Williams I, Bellini WJ, Redd SC. Persistence of vaccine-induced antibody to measles 26–33 years after vaccination. J Infect Dis 2004; 189(Suppl. 1):S123–30. 34. Kuhne M, Brown DW, Jin L. Genetic variability of measles virus in acute and persistent infections. Infect Genet Evol 2006; 6:269–76. 35. Tamin A, Rota PA, Wang ZD, Heath JL, Anderson LJ, Bellini WJ. Antigenic analysis of current wild type and vaccine strains of measles virus. J Infect Dis 1994; 170:795–801. 36. Xu W, Tamin A, Rota JS, Zhang L, Bellini WJ, Rota PA. New genetic group of measles virus isolated in the People’s Republic of China. Virus Res 1998; 54:147–56. 37. Frank SA, Bush RM. Barriers to antigenic escape by pathogens: trade-off between reproductive rate and antigenic mutability. BMC Evol Biol 2007; 7:229. 38. Parker AA, Staggs W, Dayan GH, et al. Implications of a 2005 measles outbreak in Indiana for sustained elimination of measles in the United States. N Engl J Med 2006; 355:447–55. 39. Dallaire F, De Serres G, Tremblay FW, Markowski F, Tipples G. Long-lasting measles outbreak affecting several unrelated networks of unvaccinated persons. J Infect Dis 2009; 200:1602–5. 40. Moss WJ, Cutts F, Griffin DE. Implications of the human immunodeficiency virus epidemic for control and eradication of measles. Clin Infect Dis 1999; 29:106–12. 41. Moss WJ, Monze M, Ryon JJ, Quinn TC, Griffin DE, Cutts F. Prospective study of measles in hospitalized human immunodeficiency virus (HIV)-infected and HIV-uninfected children in Zambia. Clin Infect Dis 2002; 35:189–96. 42. Scott S, Moss WJ, Cousens S, et al. The influence of HIV-1 exposure and infection on levels of passively acquired antibodies to measles virus in Zambian infants. Clin Infect Dis 2007; 45:1417–24. 43. Moss WJ, Scott S, Mugala N, et al. Immunogenicity of standard-titer measles vaccine in HIV-1-infected and uninfected Zambian children: an observational study. J Infect Dis 2007; 196:347–55. 44. McMorrow ML, Gebremedhin G, van den Heever J, et al. Measles outbreak in South Africa, 2003–2005. S Afr Med J 2009; 99:314–9. 45. Helfand RF, Moss WJ, Harpaz R, Scott S, Cutts F. Evaluating the impact of the HIV pandemic on measles control and elimination. Bull World Health Organ 2005; 83:329–37. 46. Otten M, Kezaala R, Fall A, et al. Public-health impact of accelerated measles control in the WHO African Region 2000–03. Lancet 2005; 366:832–9. 47. Scott S, Mossong J, Moss WJ, Cutts FT, Cousens S. Predicted impact of the HIV-1 epidemic on measles in developing countries: results from a dynamic age-structured model. Int J Epidemiol 2008; 37:356–67. 48. Meissner HC, Strebel PM, Orenstein WA. Measles vaccines and the potential for worldwide eradication of measles. Pediatrics 2004; 114:1065–9. 49. Griffin DE, Pan CH, Moss WJ. Measles vaccines. Front Biosci 2008; 13:1352–70. 50. Glass K, Kappey K, Grenfell BT. The effect of heterogeneity in measles vaccination on population immunity. Epidemiol Infect 2004; 132:675–83. Biological Feasibility of Measles Eradication d JID 2011:204 (Suppl 1) d S53