Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacognosy wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
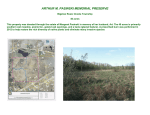
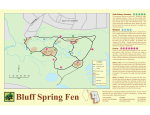
International Journal of Obesity (1999) 23, 723±732 ß 1999 Stockton Press All rights reserved 0307±0565/99 $12.00 http://www.stockton-press.co.uk/ijo Synergistic interactions between Fen¯uramine and Phentermine PJ Wellman1* and TJ Maher2 1 Behavioral Neuroscience Program, Texas A&M University, College Station, Texas 77843-4235, USA and 2Division of Pharmaceutical Sciences, Massachusetts College of Pharmacy and Health Sciences, 179 Longwood Avenue, Boston, Massachusetts 02115, USA `Fen-phen' refers to the off-label combination of the appetite suppressants fen¯uramine and phentermine. The rationale for the fen-phen combination was that the two drugs exerted independent actions on brain satiety mechanisms so that it was possible to use lower doses of each drug and yet retain a common action on suppressing appetite while minimizing adverse drug effects. The focus of the present review is to consider whether fen¯uramine and phentermine exert actions that are additive in nature or whether these two drugs exhibit drug-drug synergism. The fen-phen combination results in synergism for the suppression of appetite and body weight, the reduction of brain serotonin levels, pulmonary vasoconstriction and valve disease. Fen-phen synergism may re¯ect changes in the pharmacokinetics of drug distribution, common actions on membrane ion currents, or interactions between neuronal release and reuptake mechanisms with MAO-mediated transmitter degradation. The synergism between fen¯uramine and phentermine highlights the need to more completely understand the pharmacology and neurochemistry of appetite suppressants prior to use in combination pharmacotherapy for the treatment of obesity. Keywords: monoamine oxidase inhibitors; serotonin; drug-drug interactions; isobologram Introduction Obesity remains a chronic disorder of increasing prevalence1 that contributes to early death and health disorders.2 Moreover, obesity is known to have considerable psychological costs in the form of ostracism and discrimination.3 These physical and psychological costs provide ample motivation for obese and near-obese persons to lose body weight. Among the obesity treatments developed and implemented over the last 50 y are behavioral modi®cation, exercise, dietary restriction, surgical approaches such as gastric stapling and=or banding, and pharmacotherapy.4 The latter approach involves the use of centrally acting drugs to suppress appetite and reduce body weight5 and, more recently, agents that act peripherally to diminish absorption of dietary fat from the gastrointestinal tract (for example, Orlistat). Many factors have contributed to resistance to pharmacotherapy including the beliefs that: obesity is not a disease but a psychological issue, that the effects of appetite suppressants are modest at best, and that all appetite suppressants share common actions with the dangerous stimulant amphetamine.5 Moreover, a major concern remains that any weight *Correspondence: Paul J Wellman, Behavioral Neuroscience Program, Texas A&M University, College Station, Texas 778434235, USA. E-mail: [email protected] Received 5 November 1998; revised 16 February 1999; accepted 3 March 1999 lost during treatment with an appetite suppressant is quickly regained when the drug is terminated. Weintraub et al 6 reported on a novel approach to the pharmacological treatment of obesity using combinations of appetite suppressants rather than traditional monotherapy. This clinical trial employed a combination of fen¯uramine (30 mg prior to dinner) with phentermine (15 mg in the morning) and compared the weight reducing effects of this combination with that induced by fen¯uramine alone (20 mg ± 3 times per day) or phentermine alone (30 mg in the morning). Over a 24 week period, the combination of low doses of these anorexic medications produced a weight loss (8 kg) greater than that of placebo (4 kg), but that was equivalent to the monotherapies (fen¯uramine alone or phentermine alone). Moreover, fewer adverse effects were reported for the combination of fen-phen than for either drug alone. In 1992, Weintraub et al 7 reported on a 4-y study that examined the impact on body weight of a combination of phentermine with fen¯uramine. This study similarly noted that the fen-phen combination produced substantial weight loss in some subjects and that this combination therapy could be used for as long as 4 y.7 The fen-phen approach to pharmacotherapy was widely adopted following the Weintraub et al 7 publication. Sales of each appetite suppressant soared and it is estimated that some 18 million prescriptions were written for the fen-phen combination between 1992 and 1997.8 However, fen¯uramine and the active enantiomer dexfen¯uramine (dexfen) were withdrawn from the market in September 1997 following Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher 724 mounting concerns that use of the fen¯uramines was associated with valvular disease9 and that appetite suppressant use has been associated with the development of primary pulmonary hypertension (PPH: 10 ± 15). The use of fen¯uramine or dexfen¯uramine in combination with phentermine was `off-label' in the sense that although each of these drugs had been approved for use in the treatment of obesity, the FDA had not explicitly approved this combination of drugs. The FDA had subjected each of these drugs individually to varying degrees of scrutiny for safety and ef®cacy. There was a presumption on the part of some that one could rationally predict the safety and ef®cacy pro®le of the combination therapy from earlier research studies using each monotherapy alone. As a consequence, there appear to have been no preclinical studies conducted to determine the safety of the combination of a fen¯uramine with phentermine. Unfortunately at the time of development of the fen-phen pharmacotherapy, our understanding of the pharmacology of fen¯uramine and of phentermine was incomplete while our understanding of the fenphen combination was essentially nonexistent. Rationale for the fen-phen combination There exist two different rationales for the fen-phen combination therapy. The ®rst is that a combination of low doses of two drugs that share a common clinical effect (for example, suppression of appetite) will summate to produce a desired clinical effect. Because adverse side effects are usually a function of dose, combining low doses of different drugs should ideally maintain the desired clinical effect (that is, those effects will add together) while reducing the incidence of unwanted side effects. A secondary notion behind combining these two drugs is that fen¯uramine acts as a depressant while phentermine acts as a stimulant.16 Fen¯uramine is a racemic mixture of two enantiomers, levofen¯uramine (levofen) and dexfen. Whereas, levofen has been shown to exert antidopaminergic (for example, sedative) activity, phentermine has dopaminergic properties. Mixing phentermine with racemic fen¯uramine would theoretically cancel out these dopaminergic effects, so as to minimize patient complaints and improve compliance. Fen-phen combination therapy, however, rests on the assumption that the two drugs to be combined produce their clinical effects (appetite suppression) and adverse effects via independent mechanisms. The essence of combination therapy is that the two drugs show at least additivity: that is, their combined effects should be predictable knowing the action of each drug alone. The notion of additivity is crucial for both the clinical and adverse effects of the combination drugs. If the two drugs are less than additive in their clinical effect, then the combination will be less effective. Of greater interest is the possibility that the two drugs will mutually amplify their respective clinical effects resulting in drug-drug synergism. A synergistic combination produces a greater effect than that associated with the simple sum of effects of both drugs alone. It is interesting to note that synergism between phentermine and fen¯uramine was an issue raised by Weintraub et al 6 in their original fen-phen study: `Our data also suggest a synergistic effect of the two medications used together. The combination treatment group showed a marked, sustained increase in total fullness whereas mean results from participants receiving the other active treatments remained near baseline and similar to the placebo response. It appears that the combination of half doses of two treatments that by themselves have no effect, even in full doses, results in increased effects ± in this case total fullness.' (6: pages 1147 ± 1148.) Synergism may apply not only to the clinical outcomes of the fen-phen combination, but also to the adverse reactions associated with the combination. Thus, the primary emphasis of the present review is to consider the known synergism between the fen¯uramines and phentermine with regard to eating and body weight, cardiovascular activity (valve disease and PPH), and central nervous system activity. Neuropharmacology of Fen¯uramine and Phentermine The FDA approved Phentermine in 1959 while fen¯uramine was approved in 1973. The assumption of most investigators was that fen¯uramine acted to reduce feeding by indirectly enhancing serotonin activity in brain.17 ± 19 Fen and=or its desethylated metabolite (norfen) blocks the reuptake of serotonin into axon terminals, and at higher doses releases 5-HT from presynaptic terminals.20,21 Thus, the net effect of these actions is to increase 5-HT activity within the synapse, leading to suppression of appetite, and eventually to weight loss. Additionally, Curzon and coworkers22 have also suggested that fen¯uramine anorexia may partly re¯ect direct actions of fen at brain 5HT receptors (for example 5 HT2c receptors). Unlike fen¯uramine, phentermine has been viewed as a dopaminergic agonist similar in action and mechanism to amphetamine.23,24 An emerging theme of the recent research literature is the realization that phentermine is not only a dopaminergic agonist, but that this drug, at doses that reduce appetite, exerts important indirect effects on serotonergic neurotransmission. A secondary emphasis of the present review is that the conjoint effects of phentermine and of fen¯uramine on serotonin neurotransmission may help to explain the clinical ef®cacy of the fen-phen combination, as well as those synergistic actions of fen-phen that result in toxicity. Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher Synergistic Interactions between Phentermine and Fen¯uramine Food intake and body weight Only recently has the interaction between phentermine and a fen¯uramine been formally examined in animal studies of eating. Roth and Rowland25 examined the impact of daily IP administration of either dexfen (2 mg=kg), phentermine (5 mg=kg) or a mixture of dexfen=phentermine (2 mg=kg 5 mg=kg) on food intake and body weight in rats (see Figure 1). Daily administration of 5 mg=kg=d phentermine alone had minimal effects on food intake in rats, whereas 2 mg=kg=d dexfen produced a signi®cant reduction in food intake. More importantly, when 2 mg=kg dexfen was combined with 5 mg=kg phentermine, the combination yielded a larger suppression of food intake than that produced by 2 mg=kg dexfen alone. A similar synergy between dexfen and phentermine was evident with respect to the reduction of body weight in this study. The ®ndings of Roth and Rowland25 document a synergism between dexfen and phentermine on eating and body weight in the rat. In order to further assess fen-phen synergism over a wide range of drug doses, Roth and Rowland conducted a follow-up study using the isobologram technique to index drug-drug interactions that occur between phentermine and dexfen¯uramine.26 The isobolographic technique considers the potency of each of two drugs on food intake.27 A dose-response curve for appetite suppression is generated for each drug alone and these curves are in turn used to predict the dose-additive function for the two drugs (that is those doses that in combination would be expected to produce a 50% reduction in food intake). To examine whether the drugs are additive Figure 1 Effects of repeated administration of vehicle (open circle), DEXFEN (open triangle: 2 mg=kg), PHEN (®lled square: 5 mg=kg) and the combination (®lled diamond) of DEXFEN (2 mg=kg) and PHEN (5 mg=kg) on mean intake of sweetened milk on 11 consecutive days. (From Roth JD and Rowland NE. Ef®cacy of administration of dexfen¯uramine and phentermine, alone and in combination, on ingestive behaviour and body weight in rats. #1998, Springer-Verlag). in nature, the experimenter examines how closely various combinations of the drugs of interest produce the expected reductions in food intake. The results from the Roth and Rowland26 study con®rm a synergism between dexfen and phentermine on food intake in free-feeding rats (see Figure 2). The dose-response curves for dexfen and for phentermine are represented along the x and y axes, respectively. The solid line represents the theoretical dose additive line: that is, combinations of doses tested along this line should yield a 50% suppression of eating in rats. The two open circles in the ®gure represent the ED50 value of one drug in combination with various doses of the other drug. In one instance, the investigators combined 0.5 mg=kg dexfen with various phentermine doses. The dose additive curve predicts that about 5 mg=kg of phentermine would be required to elicit a 50% reduction in eating in combination with 0.5 mg=kg dexfen. The actual dose required was approximately 2.0 mg=kg phentermine. Similarly, when 2.5 mg=kg of phentermine was combined with various doses of dexfen, less dexfen was required to elicit a 50% reduction of eating than that predicted by the dose-additive line. The line (dotted) that bounds either side of the dose-additive line represents the 95% con®dence interval. In each instance, the combinations of dexfen and phen required smaller doses to suppress food intake by 50% than that predicted by the dose-additive line (note that each point lies outside the 95% CI). This study con®rms and extends their earlier observations and supports the notion that the dexfen-phen combination is synergistic with regard to the suppression of food intake in rats. It will be important to further extend these studies using the fen-phen combination, as this was the combination most commonly used in people. Figure 2 Isobologram of the effects of either 0.5 mg=kg dexfen in combination with various doses of phentermine or 2.5 mg=kg phentermine in combination with various doses of dex-fen. In each instance, the drug-drug combinations induced greater suppressions of eating than that predicted on the basis of dose-additivity. The dotted lines represent the 95% con®dence intervals. (Figure reprinted with permission from Roth and Rowland,26 courtesy of Elsevier Science, Amsterdam). 725 Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher 726 An advantage presumably conferred on the fenphen combination is a reduced pro®le of adverse drug effects because the combination allowed for lower doses of each drug to be used to reduce appetite and body weight. This section considers whether the adverse effects of the fen-phen combination exhibit synergy as was evident for appetite suppression. Primary pulmonary hypertension Primary pulmonary hypertension (PPH) is a rare, progressive, and generally incurable disorder involving increased pulmonary artery pressure and increased vascular resistance eventually leading to heart failure. The incidence rate of PPH is 1 ± 2 cases per million in the general population. Exposure to speci®c appetite suppressants can increase the incidence of PPH. In the 1960's, PPH was linked to the use of the appetite suppressant aminorex.13,28 More recently, PPH has been reported to be linked to the chronic use of dexfen and fen¯uramine10,11,14,15,29 Moreover, exposure to phentermine alone has resulted in reported cases of PPH.30 ± 32 Serotonin has long been thought to play a role in the development of PPH.33,34 In the 1970's, a group of German investigators explored the concept that enhancement of systemic serotonin might induce vasoconstriction and in turn contribute to the development of PPH. Subsequently, Herve et al 35 reported that PPH patients exhibit a signi®cant increase in plasma serotonin and exhibit a greater release of serotonin from aggregated platelets. Moreover, pulmonary arterial tissue taken from PPH patients exhibits greater sensitivity to serotonin relative to tissue from control patients.36 One proposed animal model of PPH indicates a link between serotonin and pulmonary hypertension. For example, rats injected with the toxic alkaloid monocrotaline (MCT) develop elevated pulmonary pressures37 within 21 days after MCT treatment. Kanai et al 38 noted that plasma serotonin levels are increased in rats 12 h after MCT treatment and that chronic pretreatment of MCT rats with the serotonin antagonist DV-7028 suppressed medial pulmonary artery hypertrophy, right ventricular hypertrophy, and pulmonary artery pressure. As noted above, phentermine use is known to produce PPH in some patients and this drug is known to interact with and to modulate serotonin activity within the pulmonary system. Seiler et al 34 reported that phentermine prolongs the vasoconstrictive action of serotonin in the isolated rat lung. More recently, Reeve et al 39 examined pulmonary artery (PA) pressure in the isolated rat lung by administering a series of vasoconstrictive stimuli (angiotensin II or hypoxia), as well as a series of infusions of vehicle followed by dexfen, or phentermine followed by dexfen. This report notes that phentermine pretreatment (10 and 100 uM) enhanced the vasoconstrictive activity of dexfen (10 and 100 uM). Although phentermine alone had no impact on PA pressure, preexposure to phentermine signi®cantly enhanced the vasoconstriction in response to dexfen. These studies indicate that phentermine increases the vasoconstrictive activity of fen¯uramine, an effect that has been argued as contributing to the induction of PPH.33 As described below, the ability of phentermine to attenuate the metabolism of serotonin could be the underlying mechanism to explain this ®nding. An issue to be resolved in future epidemiological studies is whether the combination of fen¯uramine and phentermine leads to a risk for PPH that re¯ects the additive PPH risk for each drug or whether the risk for PPH with the combination re¯ects the type of synergism evident for appetite suppression. Valvular heart disease Connolly et al 9 reported varying degress of valvular regurgitation in a series of 24 fen-phen users. Subsequent histopathological analyses revealed a thickening of the affected valves resulting in reduced valve mobility. Subsequent studies have sought to establish the incidence of valve disease as a function of anorexigen exposure. Although phentermine alone rarely produces valve disease, an evolving ®nding has been that the combination of phentermine with a fen¯uramine produces a greater incidence of valve disease than that associated with a fen¯uramine alone. Since the original report by Connolly et al 9 there have been a number of studies published and presented at meetings that report on the incidence of valvulopathies following treatment-with fen, dexfen and=or phen. These studies report a wide range of valvulopathy incidence for anorexigen exposure ranging from greater than 35% incidence down to 2 ± 4% (a value equal to control). These studies utilize a wide range of protocols. Not all the studies report on the incidence in control groups or when utilized, some control groups are not appropriately age=weight=sex matched, the durations of exposure vary widely, and the criteria used to de®ne valvulopathy severity are often inconsistent from study to study. Only a few of these studies have explicitly compared the incidence of valve disease for a fen¯uramine alone versus a group exposed to a fen¯uramine used in combination with phentermine. In the ®rst study by Khan et al,40 the odds ratio for cardiac valve abnormalities that met their case de®nition by echocardiography in patients taking dexfen alone was 12.7, whereas for those patients taking dexfen plus phentermine, or fen plus phentermine, the odds ratio increased to 24.5 and 26.3, respectively. While these authors acknowledge that the variation in duration of treatment between the groups makes interpretation dif®cult, the addition of phentermine appears to signi®cantly increase the likelihood of valvulopathy. In the second study by Wee et al 41 patients who for various reasons had undergone echocardiographic analysis prior to being prescribed fenphen or dexfen were reevaluated following cessation Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher of therapy. Of the 46 patients included in the study, only two had worsening or newly developed valvulopathies that met FDA criteria (mild aortic or moderate mitral regurgitation). Both of these patients had taken fen-phen. None of the patients who had taken dexfen developed valvulopathies. However, despite the desirability of this study design, so few patients were included so as to prevent a de®nitive conclusion regarding the in¯uence of phentermine addition. A study by Gross et al 42 reported that aortic insuf®ciency (AI) in fen-phen patients was signi®cantly altered by duration of exposure (greater than 9 months) and by dose of the combination (greater than 60 mg). Given that phentermine alone probably does not induce valve disease, the ®nding that dose combinations greater than 60 mg=d increase the likelihood of valve disease indicates that phentermine is not inert when given in combination with fen¯uramine. This latter ®nding supports the notion that mixing phentermine with fen¯uramine increases the impact of fen¯uramine on valve disease. A study by Gardin et al 43 similarly noted an increase in the incidence of mild or greater aortic regurgitation associated with fen-phen. While the control group incidence was 4.1%, the dexfen and fen-phen group incidences were 8.9% and 13.7%, respectively. In a study by Shively et al 44 the incidence of valvulopathy meeting FDA criteria was 3% in nontreated controls and 7% in patients treated with dexfen. However, when the potentially confounding factor of concomitant use of drugs reported to inhibit monoamine oxidase (for example, estrogens, thyroid) was excluded, the incidence of valve disease decreased to 4%, a value not signi®cantly different from control. The signi®cance of this ®nding relates to the observation that phentermine is an inhibitor of monoamine oxidase, the enzyme that inactivates serotonin.45 This ®nding lends further support to the notion that valve disease associated with fen-phen re¯ects enhanced systemic serotonin activity. Valve disease similar to that noted by Connolly et al 9 has been noted in carcinoid disease as well as in ergotamine toxicity.46,47 Carcinoid syndrome involves hypersecretion of serotonin whereas ergotamine is thought to exert direct actions at serotonin receptors. Whereas fen-phen-associated valve disease appears to involve primarily the left-side of the heart,9 carcinoid disease involves right side heart valves46 and ergotamine alters valves on either side of the heart.47 Fishman33 argues that the difference in pattern of valve disease re¯ects the role of the lung in the inactivation of serotonin. In carcinoid syndrome, the lung retains the ability to remove circulating serotonin, thus the valve damage is primarily on the right side whereas during fen-phen use, the lung is impaired in the ability to clear serotonin, in part because phentermine inhibits MAO and this impairs the metabolism of serotonin within the endothelium. While none of the above studies possesses the ideal experimental design, or is large enough to yield a de®nitive conclusion, each appears to support a role of phentermine in increasing the likelihood of valvulopathy in patients taking one of the fen¯uramines. Unfortunately, the appropriate study that would control for all the experimental variables and have the appropriate statistical power cannot be undertaken since the fen¯uramines are no longer available for use in humans. Brain and peripheral serotonin Serotonin (5-HT) is an indolamine transmitter found in the brain as well as the periphery. The raphe nuclei are among the primary sources of 5-HT neurons in brain and these neurons project diffusely to frontal cortex, striatum, hippocampus, hypothalamus, and brain stem. Acute exposure to very large doses of fen¯uramine reduces brain levels of serotonin.48 Although most of bodily 5-HT is found in the periphery within gut and blood platelets, few studies have examined the impact of fen¯uramine alone or in combination with phentermine on peripheral 5-HT levels and 5-HT activity. The importance of this remarkable gap is evident given recent suggestions that fen-phen alterations of systemic 5-HT may represent a primary mechanism by which to explain the impact of fen-phen therapy on the incidence of valve disease and of PPH.33,34 Table 1 Authors Species PHEN dose mg=kg (CUMUL) Baumann et al 49 Mouse 7 (56) 12 (96) Halladay et al50 Rat Lew et al 51* Rat 5 (20), 20 (80) McCann et al 52 FEN Dose mg=kg (CUMUL) Brain regions 3 (24), 10 (80), 30 (240) Forebrain 16 (128) Striatum 3.125 (12.5), 12.5 (50) Nuc accumbens Striatum Amygdala Hypothalamus Fr. Parietal cortex Hippocampus Mouse 20 (160), 40 (320), 10 (80) Striatum Hypothalamus Hippocampus Cortex Impact of FEN Evidence of on regional 5-HT synergism? ? 7 68% 7 16% 7 27% 7 38% 7 43% 7 50% 7 53% 7 15% 7 17% 7 27% 7 37% *Rats treated with fen-phen once per hour for 4 hours (all other treatments are 2=day for 4 days) None None PHEN5: YES PHEN 20: NO PHEN5: YES PHEN 20: NO PHEN5: YES PHEN 20: NO PHEN5: No PHEN 20: NO FHEN5: YES PHEN20: NO PHEN5: NO PHEN 20: NO PHEN 20: NO PHEN 40: YES PHEN20: YES PHEN40: YES PHEN 20: NO PHEN 40: NO PHEN 20: NO PHEN 40: NO 727 Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher 728 Several recent research efforts have examined the potential interactions between fen¯uramine and phentermine on brain 5-HT activity. These four extant studies are summarized in Table 1. The table presents the authors, species used, dose per injection (typically twice per day for 4 d), the cumulative dose of phentermine or fen¯uramine, the brain regions examined in the study, the impact of fen alone on 5-HT brain concentration, and whether the study observed an outcome consistent with synergism. The ®rst study was that of Baumann et al 49 who examined the changes in mouse forebrain 5-HT associated with twice a day exposure for 4 days to either 3, 10 or 30 mg=kg fen¯uramine alone or these fen¯uramine doses in combination with a single dose of 7 mg=kg phentermine. The second study of Table 2 was carried out by Halladay et al 50 who examined the impact of 16 mg=kg fen¯uramine (twice per day for 4 days) on striatal 5-HT levels as well as the impact of 12 mg=kg phentermine given in combination with the 16 mg=kg fen¯uramine regimen. Neither the Baumann study nor the Halladay study noted evidence of synergism with regard to reductions of brain serotonin content. These two studies use different species and a common exposure regimen. The studies, however are limited by the use of only a single dose of phentermine, and only examined changes in serotonin in but a single brain region. Moreover, because these severe fen¯uramine exposure regimens produced signi®cant acute reductions in brain indole content, demonstration of synergistic effects with addition of phentermine is made dif®cult. The last two entries of Table 1 provide some evidence of a synergistic interaction between phentermine and fen¯uramine on brain serotonin levels. In the Lew et al 51 study, rats were injected every hour for 4 hours with various combinations of fen-phen and then sacri®ced either 7 d or 28 d later. The rats were treated each time with either 3.125 or 12.5 mg=kg fen¯uramine, with either 5 or 20 mg=kg phentermine, or a combination of 5 mg=kg phentermine with 3.125 mg=kg fen¯uramine or 20 mg=kg phentermine with 3.125 mg=kg fen¯uramine. These authors examined changes in 5-HT levels in each of six brain regions. Four hourly injections of either 3.125 or 12.5 mg=kg fen induced dose-dependent reductions in brain serotonin in each of the six brain regions. While the 5.0 mg=kg dose of phentermine alone did not alter serotonin content in any of the six brain regions, this phentermine dose (a no effect dose for alteration of brain serotonin) enhanced the impact of 3.125 mg=kg fen dosing regimen on reducing serotonin in four of the six brain regions. In the last entry of Table 1, McCann et al 52 treated mice twice per day for 4 days with either 10 mg=kg fen, 20 or 40 mg=kg phentermine or a combination of 10 mg=kg fen with either 20 or 40 mg=kg phentermine. Levels of brain serotonin were not altered by phentermine alone. Fen¯uramine reduced brain serotonin levels and this effect was enhanced by coadministration of phentermine in hypothalamus and striatum but not in hippocampus or cortex. These studies indicate that phentermine, which by itself did not alter brain serotonin levels, enhances the impact of fen¯uramine on reducing brain serotonin levels. Table 1 also presents the impact of fen¯uramine alone on changes in regional serotonin levels. One factor that may partly explain whether fen-phen synergism is observed is the basal level of depletion produced by a test regimen of fen¯uramine. In the Lew et al 51 study, synergism was most likely observed when fen¯uramine alone produced a small decrease in regional serotonin. A similar pattern was evident in the McCann et al 52 study in which phentermine was most likely to yield synergism when the impact of fen¯uramine alone on serotonin within a brain region was small. These results suggest that the failure to observe synergism in the Halladay et al 50 study may re¯ect a ceiling effect on depletion of striatal serotonin, thereby masking any possible synergistic effect of phentermine in combination with fen¯uramine. The available studies on the interaction of phentermine with fen¯uramine on central serotonin levels utilize widely varying dose ranges and exposure regimens. A key aspect is that such studies tend to use high-dose repeated administration regimens. Further studies using a wider range of pharmacologically relevant dosages and longer exposure durations will further indicate the extent to which phentermine and fen¯uramine exhibit synergism with regard to alteration of brain serotonin systems. Similar caveats apply to future studies of the impact of fen-phen on systemic 5-HT activity. Potential mechanisms underlying fen-phen synergism Whereas the prior sections present the current state of the literature on fen-phen synergism, this section turns to a discussion of the potential explanations for such synergism. Pharmacokinetics A pharmacokinetic explanation would suggest that phentermine exposure alters the absorption, distribution, metabolism and=or elimination of fen¯uramine. The impact of phentermine on fen¯uramine pharmacokinetics is a key issue. There are data available as to whether exposure to anorexic agents similar in structure to phentermine alters fen¯uramine bioactivity. Hunsinger et al 53 reported that rats given a series of daily injections of 4.0 mg=kg=day amphetamine exhibited a greater sensitivity to the toxic actions of fen relative to rats given daily injections of vehicle. Speci®cally, amphetamine preexposure lowered the Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher LD50 value for fen from 97 mg=kg to 68 mg=kg (53). Moreover, amphetamine preexposure increased the brain levels of fen relative to that evident in rats given vehicle pretreatment. The Hunsinger et al 53 study indicates that exposure to amphetamine alters the pharmacokinetics of fen so as to prolong the duration of action and impact of fen. Given the similarity between amphetamine and phentermine in structure, activity and mechanism of action, it is reasonable to expect that phentermine exposure would also alter fen levels in brain. As described below, phentermine, like d-amphetamine, is known to competitively inhibit the enzyme that metabolizes fen and 5-HT. Additionally, fen, at these high doses, may also release dopamine and norepinephrine, thus enhancing `aggregation toxicity' of amphetamine. Thus, the increased toxicity and CNS accumulation of fen observed above might result, in part, from an interference of metabolism of fen and=or 5-HT produced by phentermine. Ion channels Changes in ion channel activity and the resulting changes in membrane potential are key elements in cell function. Weir and colleagues54 examined the impact of anorexic agents on K channel currents in smooth muscle cells taken from rat pulmonary artery. Both fen and dexfen inhibited K channel current, induced membrane depolarization and produced vasoconstriction in smooth muscle cells. More recently, dexfen has been shown to increase Ca levels within smooth muscle cells.55 These studies of peripheral cardiac muscle cells have not assessed whether K channel inhibition or elevation of intracellular Ca is enhanced by co-administration of fen or dexfen with phentermine and whether these effects occur at therapeutically relevant concentrations. Weir and colleagues56 have argued that abnormal ion channel activity appears to increase the susceptibility to the development of PPH after exposure to fen¯uramine. Serotonergic actions of phentermine Inhibition of MAO by phentermine In the 1970's, two independent research groups reported that a variety of anorexic drugs had inhibitory actions on monoamine oxidase (MAO), an intracellular enzyme that inactivates serotonin.57,58 Seiler et al 34 suggested that the MAO-inhibitory (MAOI) action of phentermine might account for the ®nding that phentermine prolonged the action of serotonin infusion on perfusion pressure in the isolated rat lung preparation. MAO inhibition by phentermine would also account for the ®ndings of Morita and Mehendale59 in which phentermine delayed the metabolism of 5-HT in rabbit lung. The observation that phentermine inhibits MAO was recently con®rmed and extended by Maher et al 45 who noted that phentermine is as potent in its inhibition of MAO as is iproniazid, an MAOI drug used to treat depression in some countries. The importance of these ®ndings is that MAO represents one of two major mechanisms by which serotonin is inactivated. The other mechanism, of course, is its reuptake into the nerve terminals or, in the periphery, into platelets. If phentermine, an MAO inhibitor, were to be combined with fen¯uramine, a drug that releases serotonin and blocks its reuptake, the expectation would be a further rise in serotoninergic activity. Thus, the combination of phentermine and a fen¯uramine would produce increases in serotonin activity that would appear as a synergism between the two drugs. As noted above, the incidence of valve disease to the fen¯uramines is reduced to control values when subjects are excluded who were exposed to the coadministration of MAO inhibitors with a fen¯uramine.44 Further support for the notion that fen-phen synergism re¯ects MAO inhibition by phentermine is provided by a study in which pretreatment of rats with the MAOI clorgyline potentiated the appetite suppressant effects of fen¯uramine.60 Thus, inhibition of MAO is suf®cient to interact with and to potentiate the appetite suppressant actions of fen¯uramine. Presumably, such effects would also occur when phentermine (an MAOI drug) were coadministered with a fen¯uramine (cf.25,26 ). Release of serotonin by phentermine The conventional wisdom has been that phentermine does not interact with central serotonin neurons in any signi®cant manner. Three recent studies using the microdialysis technique suggest that while phentermine alone has minimal impact on release of 5-HT, phentermine may further enhance the extracellular 5HT increase induced by fen¯uramine. A study by Balcioglu and Wurtman61 examined the impact of phentermine on striatal dopamine and serotonin levels in conscious rats using the microdialysis technique. Their ®ndings demonstrated that 2 and 5 mg=kg phentermine did not alter serotonin within the striatum but did signi®cantly increase striatal dopamine over baseline levels. A second study by Shoaib et al 62 noted that phentermine alone, at doses of 1.0 and 2.0 mg=kg, slightly increased the extracellular levels of 5-HT in rat nucleus accumbens, but that the serotonergic action of phentermine was much less marked than its impact on brain dopamine. More importantly, the Shoaib et al 62 study noted that the mixture of phentermine with fen¯uramine had an additive effect on increasing brain serotonin levels, an observation consistent with the MAOI effect of phentermine. A third microdialysis study by Balcioglu and Wurtman63 reported that whereas 2 mg=kg phentermine alone did not alter striatal serotonin 729 Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher 730 levels, a combination of 2 mg=kg phentermine with 1 mg=kg fen¯uramine produced a 330% increase in striatal serotonin in rat in contrast to the 182% increase in striatal serotonin induced by 1 mg=kg fen¯uramine only. These studies document that the acute effects of fen¯uramine on brain serotonin are enhanced by the addition of phentermine. Given that phentermine alone has minimal impact on brain serotonin level, this enhancement would be viewed as synergistic. These studies are limited by the small range of doses tested, by the use of mostly acute exposure to phentermine (acute exposure to fen produces increases in extracellular serotonin levels while chronic high dose fen exposure can produce declines in brain serotonin content), and by the sampling of extracellular serotonin in a limited number of brain regions. Hypothalamic serotonin, for example, is likely more important for the understanding of the impact of fen-phen on eating than is serotonin within the striatum. As was noted above, few studies have examined the action of phentermine on serotonin in the periphery. Fristrom et al 64 noted that phentermine released serotonin from rabbit blood platelets. Platelets are the major storage pool for 5-HT in blood. A more recent study in humans, indicates that phentermine may also play a role in enhancing the level of serotonin in blood platelets. Maher et al 45 reported that the administration of either 15 mg or 30 mg phentermine to human volunteers increased platelet serotonin levels by approximately 70% after one hour but did not alter plasma levels of serotonin, indicating that this effect on platelet serotonin activity probably relates to the MAO inhibition effected by phentermine. Moreover, few studies have examined the impact of the fen-phen combination on platelet 5HT activity. Redmon et al 65 reported that chronic fen-phen exposure did not alter plasma serotonin levels. This report, however, used only a single assessment of plasma serotonin (24 h after last dose) for subjects taking fen-phen, and this study did not assess platelet serotonin levels in fen-phen treated subjects. Conclusions The fen-phen combination enjoyed wide acceptance because this combination was thought to reduce body weight (and associated risks of obesity) in the absence of signi®cant risk. A remarkable aspect of fen-phen use in the treatment of human obesity is the fact that this use occurred `off-label' without animal studies to either understand the mechanism(s) of action of the fen-phen combination or to substantiate the safety of the fen-phen combination. Animal studies clearly indicate a synergism between phentermine and dex- fen¯uramine on the reduction of appetite and body weight in rats.25,26 Animal studies have also demonstrated synergism between phentermine and fen¯uramine on reduction of brain serotonin levels,51,52 and between dexfen¯uramine and phentermine on vasoconstriction of pulmonary arterial vessels.39 Recent studies indicate the coadministration of phentermine increases the incidence of valve disease associated with fen¯uramine or dexfen¯uramine. Further animal studies are required to con®rm the magnitude of synergism between phentermine and the fen¯uramines. Further epidemiological studies are needed to assess the extent to which synergism is evident in the impact of fen¯uramine in the cardiovascular system. In each instance, investigators will need to consider the use of appropriate designs that allow for the determination of synergism between phentermine and the fen¯uramines. A secondary issue of the present review is that synergism between phentermine and fen¯uramine can be viewed in the context of a drug-drug interaction. Fen¯uramine increases serotonin release and blocks reuptake of serotonin whereas phentermine may increase serotonin levels indirectly via inhibition of MAO. These interactions would be expected to enhance serotonin activity leading to a synergism of clinical effect (for example, suppressed appetite and body weight) as well as adverse effects associated with excessive serotoninergic activity. The fen-phen experience may increase our understanding of the mechanisms of action of these appetite suppressants, alone and in combination, and is likely to lead to the future development of appetite suppressant regimens with known ef®cacy and safety. Acknowledgements Dr Wellman and Dr Maher have acted, or have been approached to act as consultants and=or expert witnesses for both sides involved in litigation over fenphen in the USA. References 1 Kuczmarski RJ, Flegal KM, Campbell SM, Johnson CL. Increasing prevalence of overweight among US adults. The National Health and Nutrition Examination Surveys, 1960 to 1991. JAMA 1994; 272: 205 ± 211. 2 Bray GA. Health hazards of obesity. Endocrinol Metabol Clin N Am 1996; 25: 907 ± 919. 3 Pingitore R, Dugoni BL, Tindale RS, Spring B. Bias against overweight job applicants in a simulated employment interview. J Appl Psychol 1994; 79: 909 ± 917. 4 Blackburn GL, Miller D, Chan S. Pharmaceutical treatment of obesity. Nursing Clin of N Am 1997; 32: 831 ± 848. 5 Bray GA. Use and abuse of appetite-suppressant drugs in the treatment of obesity. Ann Int Med 1993; 119=7:Pt 2: 1 ± 13. 6 Weintraub M, Hasday JD, Mushlin AI, Lockwood DH. A double-blind clinical trial in weight control. Use of fen¯uramine and phentermine alone and in combination. Arch Internal Med 1984; 144: 1143 ± 1148. 7 Weintraub M. Long-term weight control study: conclusions. Clin Pharmacol Therap 1994; 51: 642 ± 646. Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher 8 Kassirer JP, Angell M. Losing weight ± An ill-fated new years resolution. New Eng J Med 1998; 338: 52 ± 54. 9 Connolly HM, Crary JL, McGoon MD, Hensrud DD, Edwards BS, Edwards WD, Schaff HV. Valvular heart disease associated with fen¯uramine-phentermine. New Eng J Med 1977; 337: 581 ± 588. 10 Abenhaim L, Moride Y, Brenot F, Rich S, Benichou J, Kurz X, Higenbottam T, Oakley C, Wouters E, Aubier M, Simonneau G, Begaud B. Appetite-suppressant drugs and the risk of primary pulmonary hypertension. International Primary Pulmonary Hypertension Study Group. New Eng J Med 1996; 335=9: 609 ± 616. 11 Brenot F, Herve P, Petipretz P, Paren F, Duroux P, Simonneau G. Primary pulmonary hypertension and fen¯uramine use. Brit Hrt J 1993; 70: 537 ± 541. 12 Delcroix M, Kurz X, Walckiers D, Demedts M, Naeije R. High incidence of primary pulmonary hypertension associated with appetite suppressants in Belgium. Eur Respir J 1998; 12: 271 ± 276. 13 Follath F, Burkart F, Schweize, W. Drug-induced pulmonary hypertension? BMJ 1971; 1=5743: 265 ± 266. 14 Mark EJ, Patalas ED, Chang HT, Evans RJ, Kessler SC. Fatal pulmonary hypertension associated with short-term use of fen¯uramine and phentermine. New Eng J Med 1997; 337: 602 ± 606. 15 Simonneau G, Fartoukh M, Sitbon O, Humbert M, Jagot JL, Herve P. Primary pulmonary hypertension associated with the use of fen¯uramine derivatives. Chest 1998; 114=3: Suppl, S195 ± S199. 16 Rea WP, Rothman RB, Shippenberg TS. Evaluation of the conditioned reinforcing effects of phentermine and fen¯uramine in the rat - concordance with clinical studies. Synapse 1998; 30: 107 ± 111. 17 Blundell JE. Is there a role for serotonin (5-hydroxytryptamine) in feeding? In J Obes 1977; 1: 15 ± 42. 18 Garattini S. Biological actions of drugs affecting serotonin and eating. Obesity Res 1995; 3: (Suppl): S470. 19 Garattini S, Bizzi A, Caccia S, Mennini T, Samanin R. Progress in assessing the role of serotonin in the control of food intake. Clin Neuropharmacol 1988; 11: Suppl, S32. 20 Heal DJ, Cheetam SC, Prow MR, Martin KF, Buckett WR. A comparison of the effects on central 5-HT function of sibutramine hydrochloride and other weight modifying agents. Br. J. Pharmacol 1998; 125: 301 ± 308. 21 Gundlach C, Martin KF, Heal DJ, Auerbach SB. In vivo criteria to differentiate monoamine reuptake inhibitors from releasing agents: Sibutramine is a reuptake inhibitor. J Pharmacol Exp Therap 1997; 283: 581 ± 591. 22 Curzon G, Gibson EL, Oluyomi AO. Appetite suppression by commonly used drugs depends on 5-HT receptors but not on 5HT availability. Trends Pharmacol Sci 1977; 18: 21 ± 25. 23 Bray GA. Evaluation of drugs for treating obesity. Obesity Res 1995; 3: Suppl, S434. 24 Yelnosky J, Panasevich RE, Borrelli AR, Lawlor RB. Pharmacology of phentermine. Archives Internationales de Pharmacodynamie et de Therape 1969; 178: 62 ± 76. 25 Roth JD, Rowland NE. Ef®cacy of administration of dexfen¯uramine and phentermine, alone and in combination, on ingestive behavior and body weight in rats. Psychopharmacol 1998; 137: 99 ± 106. 26 Roth JD, Rowland NE. Anorectic ef®cacy of the fen¯uramine=phentermine combination in rats: additivity or synergy? Eur J Pharmacol 1999; in press. 27 Wellman PJ, Tow S, McMahon L. Isobolographic assessment of the effects of combinations of phenylpropanolamine and fen¯uramine on food intake in rats. Pharmacol Biochem Behav 1995; 50: 287 ± 291. 28 Gurtner HP, Aminorex and pulmonary hypertension. A review. Cor et Vasa 1985; 27: 160 ± 171. 29 Douglas JG, Munro JF, Kitchin AH, Muir AL, Proudfoot AT. Pulmonary hypertension and fen¯uramine. Br Med J 1981; 6296: 881 ± 883. 30 Backmann R, Dengler H, K Gahl, Greiser R, Jesdinsky HJ, Loogen F. Primary Pulmonary Hypertension. Darmstadt: Dr. Dietrich Steinkopff Publishers, 1972. 31 Heuer L, Benoit W, Hoydrich H, Kummer D, Schick J. Pulmonale hypertonie durch appetitzughr (Mirapront). Chir Praxix 1978; 23: 497 ± 504 (German). 32 Schnabel KH, Shatz V, Busch S, Just H. Drug-induced primary vascular pulmonary hypertension. Med Welt 1976; 27: 1300 ± 1303. 33 Fishman AP. Aminorex to Fen=Phen: An epidemic foretold. Circulation 1999; 99: 156 ± 161. 34 Seiler KU, Wassermann O, Wensky H. On the role of serotonin in the pathogenesis of pulmonary hypertension induced by anorectic drugs; an experimental study in the isolated perfused rat lung, II. Fen¯uramine, mazindol, mefenorex, phentermine and R 800. Clinical & Experimental Pharmacol Physiol 1976; 3: 323 ± 330. 35 Herve P, Launay J.M, Scrobohaci ML, Brenot F, Simoneau G, Pettipretz P, Poubeau P, Cerrina J, Duroux P, Drouet L. Increased plasma serotonin in primary pulmonary hypertension. Am J Med 1995; 99: 249 ± 254. 36 Brink C, Cerrina C, Labat C et al. The effects of contractile agonists on isolated pulmonary arterial and venous muscle preparations derived from patients with primary pulmonary hypertension Am Rev Respir Dis 1988; 137=part 2: A106. 37 Hosoda Y. Pathology of pulmonary hypertension: A human and experimental study. Pathol Intl 1994; 44: 241 ± 267. 38 Kanai Y, Hori S, Tanaka T, Yasuok M, Watanabe K, Aikaa N, Hosoda Y. Role of 5-hydroxytryptamine in the progression of monocrotaline induced pulmonary hypertension in rats. Cardiovasc Res 1993; 27: 1619 ± 1623. 39 Reeve HL, Nelson DP, Archer SL, Weir KE. The effects of ¯uoxetine, phentermine, and venlafaxine on pulmonary artery pressure and electrophysiology. Am J Physiol 1999; 213 ± 219. 40 Khan MA, Herzog CA, Stpeter JV, Hartley GG, Madlonkay R, Dick CD, Asinger RW, Vessey JT. The prevalence of cardiac valvular insuf®ciency assessed by transthoracic echocardiography in obese patients treated with appetite-suppressant drugs. New Eng J Med 1998; 339: 713 ± 718. 41 Wee CC, Phillips RS, Aurigemma G, Erban S, Kriegel G, Riley M, Douglas PS. Risk for valvular heart disease among users of fen¯uramine and dexfen¯uramine who underwent echocardiography before use of medication. Ann Internal Med 1998; 129: 870 ± 874. 42 Gross SD, Leper NB, Daley WL, Buchbinder NA, Hicky A, Samuels BA. Dose and duration of appetite suppressant activity impacts incidence of valvular heart disease. Circulation 1998; 138. 43 Gardin JM. An echocardiographic evaluation of patients exposed to anorexigens as compared to unmatched controls. Presentation at the 1988 meeting of the AHA, Dallas, TX. 44 Shively BK. Echocardiographic diagnosis. Presentation at the 1998 AHA meeting Dallas, Texas. 45 Maher TJ, Ulus IH, Wurtman RJ. Phentermine and other monoamine oxidase inhibitors may increase plasma serotonin when given with fen¯uramines. Lancet 1999; 353: 38. 46 Lundin, L. Carcinoid heart disease: A cardiologist's viewpoint. Acta Oncologica 1991; 30: 499 ± 502. 47 Red®eld MM, Nicholson WJ, Edwards WD, Tajk, AJ Valve disease associated with ergot alkaloid use: Echocardiographic and pathologic correlations. Ann Intern Med, 1992; 117: 50 ± 52. 48 McCann U, Hatzidimitriou G, Ridenour A, Fischer C, Yuan J, Katz J, Ricaurte G. Dexfen¯uramine and serotonin neurotoxicity: Further preclinical evidence that clinical caution is indicated. J Pharmacol Exptl Therapeut 1994; 269: 792 ± 798. 49 Baumann MH, Schuster CR, Rothman RB. Effects of phentermine and cocaine on fen¯uramine-induced depletion of serotonin in mouse brain. Drug Alc Dep 1996; 41: 71 ± 74. 50 Halladay AK, Fisher H, Wagner GC. Interaction of phentermine plus fen¯uramine: neurochemical and neurotoxic effects. Neurotoxicol 1998; 19: 177 ± 183. 731 Fen¯uramine ± Phentermine synergism PJ Wellman and TJ Maher 732 51 Lew R, Weisenberg B, Vosmer G, Seiden LS. Combined phentermine=fen¯uramine administration enhances depletion of serotonin from central terminal ®elds. Synapse 1997; 26: 36 ± 45. 52 McCann U, Jie Y, Ricaurte GA. Neurotoxic effects of (=7)fen¯uramine and phentermine, alone and in combination, on monoamine neurons in the mouse brain. Synapse 1998; 30: 239 ± 246. 53 Hunsinger RN, Kibbe AH, Wilson MC. The effect of previous d-amphetamine treatment on the disposition and lethality of fen¯uramine in the rat. Toxicol Appl Pharmacol 1985; 79: 236 ± 245. 54 Weir EK, Reeve HL, Huang JM, Michelakis E, Nelson DP, Hampl V, Archer SL. Anorexic agents aminorex, fen¯uramine, and dexfen¯uramine inhibit potassium current in rat pulmonary vascular smooth muscle and cause pulmonary vasoconstriction. Circulation 1996; 94: 2216 ± 2220. 55 Reeve H, Archer SL, Weir EK. (1998) Dexfen¯uramine releases intracellular Ca2 in rat pulmonary artery smooth muscle cells. Circulation, 1790. 56 Weir EK, Reeve HL, Johnson G, Michelakis ED, Nelson DP, Archer SL. A role for potassium channels in smooth muscle cells and platelets in the etiology of primary pulmonary hypertension. Chest 1998; 114=3: Suppl, S200 ± S204. 57 Moller-Nielsen I, Dubnick B. Pharmacology of chlorphentermine. In: Costa E. and Garattini (eds) Amphetamines and Related Compounds. Raven Press: New York, 1970, 63 ± 73. 58 Seiler KU, Wasserman O. MAO-inhibitory properties of anorectic drugs. J Pharm Pharmacol 1973; 25: 576 ± 578. 59 Morita T, Mehendale HM. Effects of chlorphentermine and phentermine on the pulmonary disposition of 5-hydroxytryptamine in the rat in vivo. Am Rev Respir Dis 1983; 127: 747 ± 750. 60 Aulakh CS, Hill JL, Wozniak KM, Murphy DL. Fen¯uramineinduced suppression of food intake and locomotor activity is differentially altered by the selective type A monoamine oxidase inhibitor clorgyline. Psychopharmacol 1988; 95: 313 ± 317. 61 Balcioglu A, Wurtman RJ. Effects of phentermine on striatal dopamine and serotonin release in conscious rats: in vivo microdialysis study. Intl J Obesity Rel Metabol Dis 1998; 22: 325 ± 328. 62 Shoaib M, Baumann MH, Rothman RB, Goldberg SR, Schindler CW. Behavioral and neurochemical characteristics of phentermine and fen¯uramine admininistered separately and as a mixture in rats. Psychopharmacol 1996; 131: 296 ± 306. 63 Balcioglu A, Wurtman RJ. Effects of fen¯uramine and phentermine (fen-phen) on dopamine and serotonin release in rat striatum: in vivo microdialysis study in conscious animals. Brain Res 1998; 813: 67 ± 72. 64 Fristrom S, Airaksinen MM, Halmekoski J. Release of platelet 5-hydroxytryptamine by some anorexic and other sympathomimetics and their acetyl derivatives. Acta Pharmacol Toxicologicol 1977; 41: 218 ± 224. 65 Redmon B, Raatz S, Bantle JP. Valvular heart disease associated with fen¯uramine-phentermine. New Eng J Med 1997; 337=24: 1773 ± 1774.