Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Artificial gene synthesis wikipedia , lookup
Sexual dimorphism wikipedia , lookup
Medical genetics wikipedia , lookup
Designer baby wikipedia , lookup
Gene expression programming wikipedia , lookup
Causes of transsexuality wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Biology and sexual orientation wikipedia , lookup
Microevolution wikipedia , lookup
Genome (book) wikipedia , lookup
Neocentromere wikipedia , lookup
X-inactivation wikipedia , lookup
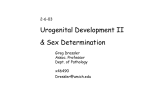
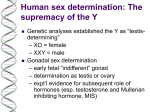
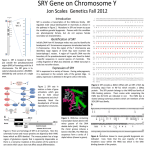
31 Case Report A CURIOUS CASE OF A 46,XX MALE: AN UNUSUAL CAUSE OF PRIMARY HYPOGONADISM Oren Steen,1 Elizabeth McCready,2 John Booth1 Division of Endocrinology and Metabolism, McMaster University, 1280 Main Street West, Hamilton, Ontario, L8S 4L8, Canada. 1 Department of Pathology and Molecular Medicine, McMaster University, 1280 Main Street West, 2 Author for Correspondence: Oren Steen Email: [email protected] Conflict of Interest: The authors have no conflicts of interest to disclose. Hamilton, Ontario, L8S 4L8, Canada. ABSTRACT: Background: 46,XX testicular disorder of sexual development is a rare cause of primary hypogonadism, characterized by a male phenotype despite a female (i.e. 46,XX) karyotype. In the vast majority of cases, it is caused by a translocation of Y chromosomal material (containing the SRY gene) onto an X chromosome. Case presentation: A 38 year-old male was referred to the endocrinology clinic for hypogonadism. His symptoms included decreased energy, diminished libido, weight gain and gynecomastia. There was no history of testicular torsion or trauma, cryptorchidism, orchitis, chemotherapy or radiation therapy. Despite 3 years of unprotected intercourse, his partner had not conceived. Physical examination was significant for bilateral gynecomastia, reduced androgen-dependent hair growth, and small, soft testes. Laboratory investigations revealed evidence of primary hypogonadism (low testosterone and elevated gonadotropins). Cytogenetic analysis revealed a 46,XX karyotype with an SRY translocation onto the short arm of the X chromosome. Conclusion: We present a rare case of 46,XX testicular disorder of sexual development, a consequence of translocation of the SRY gene onto an X chromosome. We will review its epidemiology, pathogenesis, presentation, diagnosis and management. P INTRODUCTION: rimary hypogonadism in males involves an intrinsic abnormality in the testes. It presents with low serum testosterone and elevated gonadotropins (follicle stimulating hormone (FSH) and luteinizing hormone (LH)). In contrast, central hypogonadism involves impaired pituitary (secondary hypogonadism) or hypothalamic function (tertiary hypogonadism), resulting in low serum testosterone and low or inappropriately normal gonadotropins. Consequences of hypogonadism depend on its age of onset, but may include ambiguous or female genitalia if established in the first trimester of gestation; absence or arrest of pubertal development if occurring at pubertal age; or loss of libido, erectile dysfunction, gynecomastia, decreased muscle and bone mass, fatigue and loss of body hair if established during adulthood.1 Common etiologies of primary hypogonadism include Klinefelter syndrome, bilateral torsion, orchitis, orchidectomy, and testicular trauma (induced by surgery, radiation or chemotherapy).2 We report a rare case of a 46,XX testicular disorder of sexual development (DSD): a phenotypic male with a female karyotype. WWW.MUMJ.ORG Case Report 32 McMASTER UNIVERSITY MEDICAL JOURNAL CASE PRESENTATION: A 38-year-old Caucasian male was seen in the endocrinology clinic for hypogonadism. He presented with a 6 month history of decreased energy, diminished libido, 18 kg weight gain and gynecomastia. No changes in his voice or frequency of shaving were noted, although he mentioned that he only shaved once or twice weekly. He denied any history of mumps or other testicular infections, testicular trauma, torsion or cryptorchidism. He had never received chemotherapy or radiotherapy. His puberty was timely but incomplete: He exhibited scarce facial hair, as well as decreased hair growth on his arms, legs, axillae and abdomen. He had normal (i.e. Tanner Stage 5) public hair. His voice remained midpubertal in pitch. His muscle bulk did not increase with exercise. Despite 3 years of unprotected intercourse, his partner had not conceived. He had social difficulties during his youth and was never particularly athletic. In an effort to alleviate his hypogonadal symptoms, he had been started on oral testosterone undecanoate several weeks before his referral with limited effect. His past medical history was significant for a motor vehicle collision resulting in a dashboard injury to his knees, a right scapholunate ligament repair, dyslipidemia and GERD. His medications included simvastatin, esomeprazole and testosterone undecanoate capsules. He was divorced, though newly engaged to a different partner, and worked as a carpenter. He quit smoking three years prior, consumed one to two alcoholic beverages per week, and denied illicit drug use. Family history was significant for type 2 diabetes and “heart problems” in his father. Figure 1. G -banded karyotype of the patient demonstrating a female karyotype, with two X chromosomes and the absence of a Y chromosome. On examination, he weighed 117 kg. His blood pressure was 126/92 mmHg and his heart rate was 76 bpm. Respiratory and cardiac examinations were within normal limits. He had Tanner stage III gynecomastia bilaterally with palpable glandular tissue. Abdominal examination was remarkable for a reduced amount of hair growth. His testicles were soft, measuring 6 mL on the right and 8 mL on the left (normal range 15-20 mL). No varicoceles were detected. Laboratory investigations revealed a total testosterone level of 2.0 nmol/L (normal range 7.6-31.4 nmol/L), LH 29 IU/L (normal range 2-9 IU/L) and FSH 45 IU/L (normal range 2-12 IU/L). Prolactin and iron studies were normal. A karyotype was requested to assess the possibility of Klinefelter syndrome. The chromosomal analysis using G-banding (550 bands of resolution) revealed a 46,XX karyotype (Figure 1). Polymerase chain reaction (PCR) analysis showed amplification of the SRY locus, a gene on the Y-chromosome (p11.31). Fluorescence in situ hybridization (FISH) analysis confirmed translocation of the implicated SRY gene to the short arm of the X chromosome (Figure 2). A follow-up appointment was arranged with the genetic counseling service. DISCUSSION Our patient had 46,XX testicular DSD, which is a rare cause of primary hypogonadism. The differential diagnosis for primary hypogonadism is quite broad, and is listed in Table 1. VOLUME 11 NO. 1 | 2014 Figure 2. F ISH analysis. Metaphase FISH using a FISH probe for the X chromosome centromere (green) and the SRY locus (red). The SRY probe hybridized to the distal end of the short arm of one X chromosome homolog suggesting the presence of Y chromosomal material on one copy of the X chromosome. 33 PRIMARY HYPOGONADISM IN 46,XX MALE Table 1. Causes of primary hypogonadism in males. FETAL ONSET 1. Whole gonadal dysfunction Gonadal dysgenesis: Chromosome defects: Deletions of Yp, 9p, XX/XY, XY/X, other mosaicisms Gene mutations: SRY, CBX2, MAMLD1, SF1, WT1, SOX9, DHH, XH2, DHCR, TSPYL1, etc. Vanishing testes Klinefelter syndrome 46,XX disorder of sexual development Ovotesticular DSD XX males 2. Dissociated gonadal dysfunction Leydig cells Hypoplasia/aplasia: LH/CG-R mutation Steroidogenic defects: CYP11A1, CYP17A1, HSD3B2, POR, CYB5A, or HSD17B3 mutation INSL3 mutations Sertoli cells FSH receptor mutation AMH mutation POST-NATAL ONSET 1. Whole gonadal dysfunction Prader-Willi syndrome* X-linked adrenal hypoplasia congenita* Cranial radiotherapy and chemotherapy* Lead intoxication* Marijuana consumption* Total body irradiation* Orchitis Testicular torsion or trauma Down syndrome Varicocele Chronic illnesses: e.g. granulomatous diseases, amyloidosis, cystic fibrosis, chronic pulmonary disease, renal failure, neurologic disorders Late-onset hypogonadism 2. Dissociated gonadal dysfunction Y chromosome deletions and microdeletions: AZF Gene mutations: CILD1, USP9Y, etc. Chemotherapy Abdominopelvic radiotherapy Pharmacological treatments: spironolactone, ketoconazole * indicates combined central and primary hypogonadism Adapted from (1) with permission. EPIDEMIOLOGY 46,XX testicular (DSD, formerly known as “XX male syndrome”, was initially described by Albert de la Chapelle and colleagues in 1964.3 It is a rare disorder with an incidence of 1 in 20,000-25,000 male newborns.4-8 80-90% of cases are SRY (sex-determining region Y)-positive; 10-20% are SRY-negative.4-6 PATHOGENESIS During paternal meiosis, “crossing over”, or genetic recombination of chromosomal material, takes place between the X and Y chromosomes at homologous sequences of nucleotides known as pseudoautosomal regions.4 Certain regions of the Y chromosome – known as sex-determining regions – do not normally participate in recombination.9 One such region includes the SRY gene (located on Yp11.3), which plays a pivotal role in the development of the embryonic testes, and hence male sex determination.4,5,10 As a consequence of erroneous recombination involving the SRY gene, patients with 46,XX DSD ultimately have a male phenotype despite possessing a female (i.e. 46,XX) karyotype. Translocation of the SRY gene to the X chromosome is almost always a de novo translocation, although rarely it may be inherited.11 Other rare possibilities include a de novo or inherited translocation of SRY to an autosome.11 Consistent with their male phenotype, these patients exhibit male psychosexual identification.12 Infertility is caused by the absence of the spermatogenesis locus on the long arm of the Y chromosome, which contains three AZF (azoospermia factor) regions.6,9 SRY-negative 46,XX DSD includes patients with ovotesticular-DSD (true hermaphrodites having both testicular and ovarian tissue in the gonads) and testicular-DSD (both gonads are testes with no evidence of ovarian tissue).6 Their phenotype may result from excessive or absent actions of other important genetic factors within the sexual differentiation cascade, including SOX9, DAX-1, Ad4BP/SF-1, WT1 and GATA4.5,10, Unlike their SRY-positive counterparts, SRYnegative 46,XX DSD patients often present with ambiguous genitalia at birth with a high incidence of penoscrotal hypospadias and cryptorchidism, and almost invariably develop gynecomastia around the time of puberty.6,11 True hermaphrodites may have a uterus or hemi-uterus, as well as female-range estrogen levels.11 CLINICAL PRESENTATION Patients present with primary hypogonadism manifesting as small testes (microorchidism), gynecomastia, non-obstructive azoospermia and infertility.4,5,8 Penile size is normal, and Müllerian structures are absent.11 Testes are generally soft, but may become firmer with age.11 Furthermore, these patients may display poor facial hair growth and female pubic hair distribution.6,8 One notable difference between 46,XX testicular DSD and Klinefelter syndrome is that shorter-thanaverage stature is often seen in the former, which may be related to the absence of specific growth-related genes on the Y chromosome.5,8 In addition, there is no association between learning disorders or behavioural issues and 46,XX testicular DSD.11 Although not WWW.MUMJ.ORG Case Report 34 McMASTER UNIVERSITY MEDICAL JOURNAL warranted for diagnosis, testicular biopsy generally demonstrates a decrease in size and number of seminiferous tubules, peritubular fibrosis, absence of germ cells, and Leydig cell hyperplasia.13 In 46,XX testicular DSD, testosterone levels are normal during puberty but they begin to decline during adulthood leading to primary hypogonadism.4 Diagnosis in adulthood during investigations for infertility is a classic occurrence.4-6 46,XX karyotypic abnormalities have been reported with an incidence of 0.9% in azoospermic males.14 DIAGNOSIS Diagnosis of 46,XX testicular DSD requires cytogenetic analysis, which reveals a normal female (46,XX) karyotype. Next, FISH of an SRY probe to metaphase chromosomes should be undertaken, in order to determine the nature of the rearrangement.11This may involve SRY translocated on an X chromosome (most common scenario), or rarely, SRY translocated on an autosome.11 It is important to determine the nature of the rearrangement, as the modes of inheritance and implications for genetic counseling are different.11 Although PCR for SRY is more sensitive than FISH, it cannot establish the nature of the chromosomal rearrangement, and hence the inheritance pattern.11 MANAGEMENT With respect to management of 46,XX testicular DSD, patients may benefit from psychological support, particularly after disclosing their diagnosis.11 They require lifelong endocrinology follow-up with regular bone mineral density (BMD) measurements and treatment of osteopenia, as well as testosterone supplementation.5 The latter is generally initiated after age 14 at low doses, and gradually increased to reach adult levels.11 Our patient had a suboptimal response to oral testosterone undecanoate, conceivably because the latter is known to have unreliable oral bioavailability, fluctuating serum levels and a short half-life, necessitating multiple daily dosing.15 For these reasons, intramuscular and transdermal testosterone preparations are preferable. Gynecomastia, if still a concern following testosterone replacement therapy, can be treated by reduction mammoplasty.11 The only available fertility option short of adoption involves artificial insemination via donor sperm.5, with success rates on the order of 14% per cycle and 77% after 12 cycles.16 Genetic counseling would also be beneficial in order to educate patients on the nature, inheritance and implications of their condition.11 CONCLUSION We report a rare case of 46, XX testicular DSD with an SRY translocation on the short arm of an X chromosome. Cytogenetic analysis is a crucial investigative tool for this particular condition. These patients benefit from genetic counseling and lifelong endocrinology follow-up. Abbreviations FSH: follicle-stimulating hormone; LH: luteinizing hormone; G-banding: Giemsa banding; PCR: polymerase chain reaction; SRY: sex determining region Y; FISH: fluorescence in situ hybridization; DSD: disorder of sexual development; AZF: azoospermia factor. References 1. Rey RA, Grinspon RP, Gottlieb S et al. Male hypogonadism: an extended classification based on a developmental, endocrine physiology-based approach. Andrology. 2013;1(1):3-16. 2. Yin A, Swerdloff R. Treating hypogonadism in younger males. Expert Opin Pharmacother. 2010;11(9):1529-40. 3. de la Chapelle A, Hortling H, Niemi M, Wennstroem J. XX sex chromosomes in a human male: first case. Acta Med Scand. 1964;175(Suppl 412):25-8. 4. Gunes S, Asci R, Okten G et al. Two males with SRY-positive 46,XX testicular disorder of sex development. Syst Biol Reprod Med. 2013;59:42-7. 5. Ryan NAJ, Akbar S. A case report of an incidental finding of a 46,XX, SRY-negative male with masculine phenotype during standard fertility workup with review of the literature and proposed immediate long-term management guidance. Fertil Steril. 2013;99(5):1273-6. 6. Alves C, Braid Z, Coeli FB, de Mello MP. 46,XX male - testicular disorder of sexual differentiation (DSD): hormonal, molecular and cytogenetic studies. Arq Bras Endocrinol. 2010;54(8):685-9. 7. Wang T, Liu JH, Yang J et al. 46,XX male sex reversal syndrome: a case report and review of the genetic basis. Andrologia. 2009;41:59-62. 8. Jain M, V V, Chaudhary I, Halder A. The Sertoli Cell Only Syndrome and Glaucoma in a Sex-Determining Region Y (SRY) Positive XX Infertile Male. J Clin Diagn Res. 2013;7(7):1457-9. 9. L emaitre C, Braga MD, Gautier C et al. Footprints of inversions at present and past pseudoautosomal boundaries in human sex chromosomes. Genome Biol Evol. 2009;1:56-66. 10. Gao X, Chen G, Huang J et al. Clinical, cytogenic and molecular analysis with 46,XX male reversal syndrome: case reports. Assist Reprod Genet. 2013;30:431-5. 11. Vilain EJ. 46,XX Testicular Disorder of Sex Development. in GeneReviewsTM [Internet]. In: Pagon RA, Bird TD, Dolan CR et al, editors. Seattle (WA): University of Washington, Seattle, 2013. 12. de la Chapelle A. Analytic review: nature and origin of males with XX sex chromosomes. Am J Hum Genet. 1972;24(1):71-105. 13. de la Chapelle A. The etiology of maleness in XX men. Hum Genet. 1981;58:105-16. 14. Cavkaytar S, Batioglu S, Gunel M et al. Genetic evaluation of severe male factor infertility in Turkey: a cross-sectional study. Hum Fertil. 2012;15(2):100-6. 15. Nieschlag E, Behre HM, Bouchard P et al. Testosterone replacement therapy: current trends and future directions. Hum Reprod Update. 2004;10(5):409-19. 16. De Brucker M, Haentjens P, Evenepoel J et al. Cumulative delivery rates in different age groups after artificial insemination with donor sperm. Hum Reprod. 2009;24(8):1891-9. VOLUME 11 NO. 1 | 2014